-
Question 1
Incorrect
-
A 50-year-old man comes in with an episode of alcoholic pancreatitis. He shows gradual improvement and is assessed at his 6-week follow-up. He has a bloated feeling in his upper abdomen and a fluid collection is discovered behind his stomach on imaging. His serum amylase levels are slightly elevated. What is the most probable cause?
Your Answer: Pancreatic abscess
Correct Answer: Pseudocyst
Explanation:It is improbable for pseudocysts to be detected within 4 weeks of an episode of acute pancreatitis. Nevertheless, they are more prevalent during this period and are linked to an elevated amylase level.
Acute pancreatitis can lead to various complications, both locally and systemically. Local complications include peripancreatic fluid collections, which occur in about 25% of cases and may develop into pseudocysts or abscesses. Pseudocysts are walled by fibrous or granulation tissue and typically occur 4 weeks or more after an attack of acute pancreatitis. Pancreatic necrosis, which involves both the pancreatic parenchyma and surrounding fat, can also occur and is directly linked to the extent of necrosis. Pancreatic abscesses may result from infected pseudocysts and can be treated with drainage methods. Haemorrhage may also occur, particularly in cases of infected necrosis.
Systemic complications of acute pancreatitis include acute respiratory distress syndrome, which has a high mortality rate of around 20%. Local complications such as peripancreatic fluid collections and pancreatic necrosis can also lead to systemic complications if left untreated. It is important to manage these complications appropriately, with conservative management being preferred for sterile necrosis and early necrosectomy being avoided unless necessary. Treatment options for local complications include endoscopic or surgical cystogastrostomy, aspiration, and drainage methods. Overall, prompt recognition and management of complications is crucial in improving outcomes for patients with acute pancreatitis.
-
This question is part of the following fields:
- Surgery
-
-
Question 2
Incorrect
-
A 50-year-old man presents to his GP with concerns about erectile dysfunction. He has been experiencing this for the past year and is feeling embarrassed and anxious about it, as it is causing issues in his marriage. On examination, the GP notes that the patient is overweight with a BMI of 27 kg/m2, but does not find any other abnormalities. The GP orders HbA1c and lipid tests. What other steps should the GP take at this point?
Your Answer: Prolactin and FSH/LH
Correct Answer: Morning testosterone
Explanation:The appropriate test to be conducted on all men with erectile dysfunction is the morning testosterone level check. Checking for Chlamydia and gonorrhoeae NAAT is not necessary. Prolactin and FSH/LH should only be checked if the testosterone level is low. Referring for counseling may be considered if psychological factors are suspected, but other tests should be conducted first. Endocrinology referral is not necessary at this stage, but may be considered if the testosterone level is found to be reduced.
Erectile dysfunction (ED) is a condition where a man is unable to achieve or maintain an erection that is sufficient for sexual activity. It is not a disease but a symptom that can be caused by organic, psychogenic, or mixed factors. It is important to differentiate between the causes of ED, with gradual onset of symptoms, lack of tumescence, and normal libido favoring an organic cause, while sudden onset of symptoms, decreased libido, and major life events favoring a psychogenic cause. Risk factors for ED include cardiovascular disease, alcohol use, and certain medications.
To assess for ED, it is recommended to measure lipid and fasting glucose serum levels to calculate cardiovascular risk, as well as free testosterone levels in the morning. If free testosterone is low or borderline, further assessment may be needed. PDE-5 inhibitors, such as sildenafil, are the first-line treatment for ED and should be prescribed to all patients regardless of the cause. Vacuum erection devices can be used as an alternative for those who cannot or will not take PDE-5 inhibitors.
For young men who have always had difficulty achieving an erection, referral to urology is appropriate. Additionally, people with ED who cycle for more than three hours per week should be advised to stop. Overall, ED is a common condition that can be effectively managed with appropriate treatment.
-
This question is part of the following fields:
- Surgery
-
-
Question 3
Correct
-
A 25-year-old man has had surgery for an inguinal hernia. After a week, he comes back with a wound that is red, painful, and oozing pus. What is the probable reason for this?
Your Answer: Infection with Staphylococcus aureus
Explanation:Staph aureus was responsible for the majority of infections, as per the given situation. Infections caused by strep pyogenes and other organisms were infrequent.
Preventing Surgical Site Infections
Surgical site infections (SSI) are a common complication following surgery, with up to 20% of all healthcare-associated infections being SSIs. These infections occur when there is a breach in tissue surfaces, allowing normal commensals and other pathogens to initiate infection. In many cases, the organisms causing the infection are derived from the patient’s own body. Measures that may increase the risk of SSI include shaving the wound using a razor, using a non-iodine impregnated incise drape, tissue hypoxia, and delayed administration of prophylactic antibiotics in tourniquet surgery.
To prevent SSIs, there are several steps that can be taken before, during, and after surgery. Before surgery, it is recommended to avoid routine removal of body hair and to use electric clippers with a single-use head if hair needs to be removed. Antibiotic prophylaxis should be considered for certain types of surgery, such as placement of a prosthesis or valve, clean-contaminated surgery, and contaminated surgery. Local formulary should be used, and a single-dose IV antibiotic should be given on anesthesia. If a tourniquet is to be used, prophylactic antibiotics should be given earlier.
During surgery, the skin should be prepared with alcoholic chlorhexidine, which has been shown to have the lowest incidence of SSI. The surgical site should be covered with a dressing, and wound edge protectors do not appear to confer any benefit. Postoperatively, tissue viability advice should be given for the management of surgical wounds healing by secondary intention. The use of diathermy for skin incisions is not advocated in the NICE guidelines, but several randomized controlled trials have demonstrated no increase in the risk of SSI when diathermy is used.
-
This question is part of the following fields:
- Surgery
-
-
Question 4
Incorrect
-
A 36-year-old male comes to the Emergency Department complaining of abdominal pain that has been bothering him for 10 hours. He feels the pain on his right side and it radiates from the side of his abdomen down to his groin. Upon urinalysis, blood and leukocytes are detected. He requests pain relief. What is the most suitable analgesic to administer based on the probable diagnosis?
Your Answer: Codeine
Correct Answer: Diclofenac
Explanation:The acute management of renal colic still recommends the utilization of IM diclofenac, according to guidelines.
The symptoms presented are typical of renal colic, including pain from the loin to the groin and urine dipstick results. For immediate relief of severe pain, the most effective method is administering intramuscular diclofenac at a dosage of 75 mg. For milder pain, the rectal or oral route may be used. It is important to check for any contraindications to NSAIDs, such as a history of gastric/duodenal ulcers or asthma.
The management of renal stones involves initial medication and investigations, including an NSAID for analgesia and a non-contrast CT KUB for imaging. Stones less than 5mm may pass spontaneously, but more intensive treatment is needed for ureteric obstruction or renal abnormalities. Treatment options include shockwave lithotripsy, ureteroscopy, and percutaneous nephrolithotomy. Prevention strategies include high fluid intake, low animal protein and salt diet, and medication such as thiazides diuretics for hypercalciuria and allopurinol for uric acid stones.
-
This question is part of the following fields:
- Surgery
-
-
Question 5
Incorrect
-
A 47-year-old man arrives at the emergency department complaining of severe abdominal pain. He is restless and describes the pain as 10/10, originating from the right side of his back and radiating to his right testicle. He has vomited once but has no other symptoms. His vital signs are stable except for a heart rate of 100 bpm. A urine dip reveals ++ blood. He is administered PR diclofenac and oramorph for pain relief. The following day, his pain is under control, and the tachycardia has subsided. A CTKUB is performed, which reveals no stones in the ureters but shows stranding of the peri-ureteric fat. There is no indication of any bowel or other abdominal organ pathology. What is the accurate diagnosis?
Your Answer: Ureteric rupture
Correct Answer: Spontaneously passed ureteric calculus
Explanation:If a ureteric calculus is not present, the presence of periureteric fat stranding may indicate recent stone passage. Most stones that are less than 5mm in the ureteric axis will pass on their own. Fat stranding can be seen beside the ureter, indicating recent stone passage, or beside the kidney, which may be a sign of pyelonephritis. Urothelial carcinoma typically presents with a chronically obstructed and hydronephrotic kidney, which may have been detected on a contrast CT scan. The patient’s symptoms and radiological findings do not suggest pyelonephritis or malingering. Ureteric rupture is rare and is usually caused by medical intervention, and a urinoma in the retroperitoneal space would be visible on a CTKUB.
Types of Renal Stones and their Appearance on X-ray
Renal stones, also known as kidney stones, are solid masses that form in the kidneys due to the accumulation of certain substances. There are different types of renal stones, each with a unique appearance on x-ray. Calcium oxalate stones are the most common, accounting for 40% of cases, and appear opaque on x-ray. Mixed calcium oxalate/phosphate stones and calcium phosphate stones also appear opaque and make up 25% and 10% of cases, respectively. Triple phosphate stones, which develop in alkaline urine and are composed of struvite, account for 10% of cases and appear opaque as well. Urate stones, which are radiolucent, make up 5-10% of cases. Cystine stones, which have a semi-opaque, ‘ground-glass’ appearance, are rare and only account for 1% of cases. Xanthine stones are the least common, accounting for less than 1% of cases, and are also radiolucent. Staghorn calculi, which involve the renal pelvis and extend into at least 2 calyces, are composed of triple phosphate and are more likely to develop in alkaline urine. Infections with Ureaplasma urealyticum and Proteus can increase the risk of their formation.
-
This question is part of the following fields:
- Surgery
-
-
Question 6
Correct
-
A 28-year-old male has come for his pre-operative assessment before his tonsillectomy due to recurrent tonsillitis. During the assessment, the anaesthetist asks about his family history and he reveals that his father and paternal grandfather both had malignant hyperthermia after receiving general anaesthesia. However, his mother and paternal grandmother have never had any adverse reactions to general anaesthesia. What is the likelihood of this patient experiencing a similar reaction after receiving general anaesthesia?
Your Answer: 50%
Explanation:Malignant Hyperthermia: A Condition Triggered by Anaesthetic Agents
Malignant hyperthermia is a medical condition that often occurs after the administration of anaesthetic agents. It is characterized by hyperpyrexia and muscle rigidity, which is caused by the excessive release of calcium ions from the sarcoplasmic reticulum of skeletal muscle. This condition is associated with defects in a gene on chromosome 19 that encodes the ryanodine receptor, which controls calcium release from the sarcoplasmic reticulum. Susceptibility to malignant hyperthermia is inherited in an autosomal dominant fashion. It is worth noting that neuroleptic malignant syndrome may have a similar aetiology.
The causative agents of malignant hyperthermia include halothane, suxamethonium, and other drugs such as antipsychotics (which can trigger neuroleptic malignant syndrome). To diagnose this condition, doctors may perform tests such as checking for elevated levels of creatine kinase and conducting contracture tests with halothane and caffeine.
The management of malignant hyperthermia involves the use of dantrolene, which prevents the release of calcium ions from the sarcoplasmic reticulum. With prompt and appropriate treatment, patients with malignant hyperthermia can recover fully. Therefore, it is essential to be aware of the risk factors and symptoms of this condition, especially when administering anaesthetic agents.
-
This question is part of the following fields:
- Surgery
-
-
Question 7
Incorrect
-
A 50-year-old woman presents with fever and pain in the upper right quadrant. Her blood work reveals an elevated CRP and an ultrasound confirms acute cholecystitis. The patient is administered analgesia and IV fluids. What other treatment options are likely to be prescribed for this patient?
Your Answer: Intravenous antibiotics + repeat ultrasound after 6 weeks
Correct Answer: Intravenous antibiotics + laparoscopic cholecystectomy within 1 week
Explanation:Acute cholecystitis is a condition where the gallbladder becomes inflamed. This is usually caused by gallstones, which are present in 90% of cases. The remaining 10% of cases are known as acalculous cholecystitis and are typically seen in severely ill patients who are hospitalized. The pathophysiology of acute cholecystitis is multifactorial and can be caused by gallbladder stasis, hypoperfusion, and infection. In immunosuppressed patients, it may develop due to Cryptosporidium or cytomegalovirus. This condition is associated with high morbidity and mortality rates.
The main symptom of acute cholecystitis is right upper quadrant pain, which may radiate to the right shoulder. Patients may also experience fever and signs of systemic upset. Murphy’s sign, which is inspiratory arrest upon palpation of the right upper quadrant, may be present. Liver function tests are typically normal, but deranged LFTs may indicate Mirizzi syndrome, which is caused by a gallstone impacted in the distal cystic duct, causing extrinsic compression of the common bile duct.
Ultrasound is the first-line investigation for acute cholecystitis. If the diagnosis remains unclear, cholescintigraphy (HIDA scan) may be used. In this test, technetium-labelled HIDA is injected IV and taken up selectively by hepatocytes and excreted into bile. In acute cholecystitis, there is cystic duct obstruction, and the gallbladder will not be visualized.
The treatment for acute cholecystitis involves intravenous antibiotics and cholecystectomy. NICE now recommends early laparoscopic cholecystectomy, within 1 week of diagnosis. Previously, surgery was delayed for several weeks until the inflammation had subsided. Pregnant women should also proceed to early laparoscopic cholecystectomy to reduce the chances of maternal-fetal complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 8
Incorrect
-
A 28-year-old male patient visits their GP complaining of abdominal pain and bloody diarrhoea that began six weeks ago. He has never experienced anything like this before and believes he may have lost some weight in the past three months. When asked about his family history, he mentions that his father was diagnosed with bowel cancer at the age of 30, and he remembers his grandfather having a stoma before he passed away when the patient was a child. The GP suspects bowel cancer and is concerned about a potential genetic abnormality. During colonoscopy, a large tumour is discovered in the ascending colon near the hepatic flexure, but the rest of the colonic mucosa appears normal. What is the most probable underlying genetic issue?
Your Answer: Von-Hippel Lindau Disease (VHL)
Correct Answer: Lynch Syndrome
Explanation:Familial adenomatous polyposis (FAP) has a mutation in the APC gene and is characterized by over 100 colonic adenomas and a 100% cancer risk. MYH-associated polyposis has a biallelic mutation of the MYH gene and is associated with multiple colonic polyps and a 100% cancer risk by age 60. Peutz-Jeghers syndrome has a mutation in the STK11 gene and is characterized by multiple benign intestinal hamartomas and an increased risk of GI cancers. Cowden disease has a mutation in the PTEN gene and is associated with multiple intestinal hamartomas and an 89% risk of cancer at any site. HNPCC (Lynch syndrome) has germline mutations of DNA mismatch repair genes and is associated with a high risk of colorectal and endometrial cancer. Screening and management strategies vary for each syndrome.
-
This question is part of the following fields:
- Surgery
-
-
Question 9
Incorrect
-
A 38-year-old woman is scheduled for a Caesarean section due to fetal distress. She expresses concern about the healing of her wound, as she had a previous surgical incision that became infected and resulted in abscess formation.
Which of the following underlying medical conditions places her at the highest risk for poor wound healing?Your Answer:
Correct Answer: Diabetes
Explanation:Factors Affecting Wound Healing: Diabetes, Hypertension, Asthma, Inflammatory Bowel Disease, and Psoriasis
Wound healing is a complex process that can be affected by various factors. Among these factors are certain medical conditions that can increase the risk of poor wound healing and post-surgical complications.
Diabetes, for instance, is a well-known risk factor for impaired wound healing. Patients with poorly controlled diabetes are particularly vulnerable to delayed wound healing and increased risk of infection. Therefore, it is crucial to ensure good diabetic control before and after surgery and closely monitor patients for any signs of infection or wound breakdown.
Hypertension, on the other hand, is not a common cause of poor wound healing, but severely uncontrolled hypertension that affects perfusion can increase the risk of wound breakdown. Asthma, unless accompanied by regular oral steroid use or persistent cough, is also unlikely to affect wound healing. Similarly, inflammatory bowel disease itself does not cause impaired wound healing, unless the patient is malnourished or on regular oral steroids.
Finally, psoriasis is not a common cause of impaired wound healing, but care should be taken to avoid any affected skin during surgery. Overall, understanding the impact of these medical conditions on wound healing can help healthcare providers optimize patient care and improve surgical outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 10
Incorrect
-
A 55 year old man visits his doctor complaining of a swollen scrotum. Although he had no discomfort, his wife urged him to seek medical attention. Upon examination, there is a swelling on the left side of the scrotal sac that is painless and fully transilluminates. The testicle cannot be felt. What is the probable cause of this condition?
Your Answer:
Correct Answer: Hydrocele
Explanation:The male patient has a swelling in his scrotal sac that is painless and allows light to pass through. The only possible diagnosis based on these symptoms is a hydrocele, which is a buildup of clear fluid around the testicles. This condition makes it difficult to feel the testes.
Causes and Management of Scrotal Swelling
Scrotal swelling can be caused by various conditions, including inguinal hernia, testicular tumors, acute epididymo-orchitis, epididymal cysts, hydrocele, testicular torsion, and varicocele. Inguinal hernia is characterized by inguinoscrotal swelling that cannot be examined above it, while testicular tumors often have a discrete testicular nodule and symptoms of metastatic disease. Acute epididymo-orchitis is often accompanied by dysuria and urethral discharge, while epididymal cysts are usually painless and occur in individuals over 40 years old. Hydrocele is a non-painful, soft fluctuant swelling that can be examined above, while testicular torsion is characterized by severe, sudden onset testicular pain and requires urgent surgery. Varicocele is characterized by varicosities of the pampiniform plexus and may affect fertility.
The management of scrotal swelling depends on the underlying condition. Testicular malignancy is treated with orchidectomy via an inguinal approach, while torsion requires prompt surgical exploration and testicular fixation. Varicoceles are usually managed conservatively, but surgery or radiological management can be considered if there are concerns about testicular function or infertility. Epididymal cysts can be excised using a scrotal approach, while hydroceles are managed differently in children and adults. In children, an inguinal approach is used to ligate the underlying pathology, while in adults, a scrotal approach is preferred to excise or plicate the hydrocele sac.
-
This question is part of the following fields:
- Surgery
-
-
Question 11
Incorrect
-
A 32-year-old man presents to the emergency department with a painful left calf. This has been slowly getting worse for the past 2 days and came without any warning. He uses cocaine regularly but has otherwise no medical history of note. He admits to sometimes using blood vessels on his hands and the front of his elbow to inject.
On examination, the left calf is paler than his right. Radial pulses can be felt, but his extensor digitorum is difficult to find on the left. He is unable to move his left foot. There is no tenderness, changes in calf size or systemic upset.
What is the most likely diagnosis?Your Answer:
Correct Answer: Acute limb ischaemia
Explanation:The 6 P’s – pale, pulseless, pain, paralysis, paraesthesia, and perishingly cold – are characteristic symptoms of acute limb-threatening ischaemia. A man with a sudden onset of lower leg pain, loss of distal pulses, pallor, and paralysis may have developed an arterial thrombus due to heroin injection into an artery instead of a vein. Although not all 6 symptoms may be present, this constellation of symptoms should raise suspicion of acute limb ischaemia. Compartment syndrome, which typically presents with tenderness and a precipitating event, is an important differential diagnosis. Critical limb ischaemia, caused by chronic arterial occlusion, is unlikely in this case as symptoms would have been present for longer than 2 weeks. Deep vein thrombosis, which presents with redness, swelling, and tenderness, is another important differential diagnosis that can be ruled out in this scenario.
Peripheral arterial disease can present in three main ways: intermittent claudication, critical limb ischaemia, and acute limb-threatening ischaemia. The latter is characterized by one or more of the 6 P’s: pale, pulseless, painful, paralysed, paraesthetic, and perishing with cold. Initial investigations include a handheld arterial Doppler examination and an ankle-brachial pressure index (ABI) if Doppler signals are present. It is important to determine whether the ischaemia is due to a thrombus or embolus, as this will guide management. Thrombus is suggested by pre-existing claudication with sudden deterioration, reduced or absent pulses in the contralateral limb, and evidence of widespread vascular disease. Embolus is suggested by a sudden onset of painful leg (<24 hours), no history of claudication, clinically obvious source of embolus, and no evidence of peripheral vascular disease. Initial management includes an ABC approach, analgesia, intravenous unfractionated heparin, and vascular review. Definitive management options include intra-arterial thrombolysis, surgical embolectomy, angioplasty, bypass surgery, or amputation for irreversible ischaemia.
-
This question is part of the following fields:
- Surgery
-
-
Question 12
Incorrect
-
A 38-year-old woman arrives at the emergency department complaining of intermittent pain in her right upper quadrant for the past 3 hours. She reports that the pain worsens after eating and spreads to her right shoulder blade. There are no signs of jaundice or fever.
What blood test results would be anticipated for a diagnosis of biliary colic?Your Answer:
Correct Answer: Normal ALP and γGT, normal AST and ALT, normal CRP
Explanation:Biliary colic is characterized by intermittent pain caused by a gallstone passing through the biliary tree. Unlike other gallstone-related conditions, such as cholecystitis, biliary colic does not cause fever or abnormal liver function tests/inflammatory markers. The absence of jaundice suggests that the stone is not obstructing the common bile duct, resulting in normal liver enzymes. Therefore, the correct answer is normal ALP and γGT, normal AST and ALT, and normal CRP. Referred pain may also be present at the tip of the scapula.
Biliary colic is a condition that occurs when gallstones pass through the biliary tree. The risk factors for this condition are commonly referred to as the ‘4 F’s’, which include being overweight, female, fertile, and over the age of forty. Other risk factors include diabetes, Crohn’s disease, rapid weight loss, and certain medications. Biliary colic occurs due to an increase in cholesterol, a decrease in bile salts, and biliary stasis. The pain associated with this condition is caused by the gallbladder contracting against a stone lodged in the cystic duct. Symptoms include right upper quadrant abdominal pain, nausea, and vomiting. Diagnosis is typically made through ultrasound. Elective laparoscopic cholecystectomy is the recommended treatment for biliary colic. However, around 15% of patients may have gallstones in the common bile duct at the time of surgery, which can result in obstructive jaundice. Other possible complications of gallstone-related disease include acute cholecystitis, ascending cholangitis, acute pancreatitis, gallstone ileus, and gallbladder cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 13
Incorrect
-
A 68-year-old woman presents to her GP with a shallow sore on her left leg that has not healed for 2 weeks. She is worried and seeks medical advice. Upon examination, the patient is found to be overweight with a BMI of 35.3 kg/m². An open sore measuring 5 x 3 cm is observed on the medial aspect of her left shin, superior to her medial malleolus. Additionally, an enlarged, tortuous vein is visible on her left calf, and her ABPI is 1.2 with palpable pedal pulses bilaterally. Based on this information, what is the indication for referral to vascular surgery?
Your Answer:
Correct Answer: She has a venous leg ulcer
Explanation:Patients with varicose veins and a venous leg ulcer, whether active or healed, should be referred to secondary care for treatment. NICE CKS guidelines state that referral is also necessary for patients with symptoms such as ‘heavy’ or ‘aching’ legs, skin changes associated with chronic venous insufficiency, or superficial vein thrombosis. The presence of varicose veins alone is not a sufficient reason for referral unless it is symptomatic or associated with the aforementioned conditions. It is important to consider the patient’s ideas, concerns, and expectations, but unsightliness alone is not a reason for referral. Referral is necessary if the patient’s ABPI is <0.8 or >1.3, as this may suggest mixed arterial/venous disease or unsuitability for compression therapy due to vessel calcification. Age is not a factor in referral criteria, as varicose veins can affect individuals of all ages, including young pregnant women.
Understanding Varicose Veins
Varicose veins are enlarged and twisted veins that occur when the valves in the veins become weak or damaged, causing blood to flow backward and pool in the veins. They are most commonly found in the legs due to the great saphenous vein and small saphenous vein reflux. Although they are a common condition, most patients do not require any medical intervention. However, some patients may experience symptoms such as aching, itching, and throbbing, while others may develop complications such as skin changes, bleeding, superficial thrombophlebitis, and venous ulceration.
To diagnose varicose veins, a venous duplex ultrasound is usually performed to detect retrograde venous flow. Treatment options include conservative measures such as leg elevation, weight loss, regular exercise, and graduated compression stockings. However, patients with significant or troublesome symptoms, skin changes, or complications may require referral to secondary care for further management. Possible treatments include endothermal ablation, foam sclerotherapy, or surgery.
Understanding varicose veins is important for patients to recognize the symptoms and seek medical attention if necessary. With proper management, patients can alleviate their symptoms and prevent complications from developing.
-
This question is part of the following fields:
- Surgery
-
-
Question 14
Incorrect
-
Which one of the following statements regarding male circumcision is correct?
Your Answer:
Correct Answer: Reduces the rate of HIV transmission
Explanation:Understanding Circumcision
Circumcision is a practice that has been carried out in various cultures for centuries. Today, it is mainly practiced by people of the Jewish and Islamic faith for religious or cultural reasons. However, it is important to note that circumcision for these reasons is not available on the NHS.
The medical benefits of circumcision are still a topic of debate. However, some studies have shown that it can reduce the risk of penile cancer, urinary tract infections, and sexually transmitted infections, including HIV.
There are also medical indications for circumcision, such as phimosis, recurrent balanitis, balanitis xerotica obliterans, and paraphimosis. It is crucial to rule out hypospadias before performing circumcision as the foreskin may be needed for surgical repair.
Circumcision can be performed under local or general anesthesia. It is a personal decision that should be made after careful consideration of the potential benefits and risks.
-
This question is part of the following fields:
- Surgery
-
-
Question 15
Incorrect
-
A 49-year-old female patient complains of loin pain and haematuria. Upon urine dipstick examination, the results show:
Blood ++++
Nitrites POS
Leucocytes +++
Protein ++
Further urine culture reveals a Proteus infection, while an x-ray confirms the presence of a stag-horn calculus in the left renal pelvis. What is the probable composition of the renal stone?Your Answer:
Correct Answer: Struvite
Explanation:Stag-horn calculi consist of struvite and develop in urine with high alkalinity, which is often caused by the presence of ammonia-producing bacteria.
Types of Renal Stones and their Appearance on X-ray
Renal stones, also known as kidney stones, are solid masses that form in the kidneys due to the accumulation of certain substances. There are different types of renal stones, each with a unique appearance on x-ray. Calcium oxalate stones are the most common, accounting for 40% of cases, and appear opaque on x-ray. Mixed calcium oxalate/phosphate stones and calcium phosphate stones also appear opaque and make up 25% and 10% of cases, respectively. Triple phosphate stones, which develop in alkaline urine and are composed of struvite, account for 10% of cases and appear opaque as well. Urate stones, which are radiolucent, make up 5-10% of cases. Cystine stones, which have a semi-opaque, ‘ground-glass’ appearance, are rare and only account for 1% of cases. Xanthine stones are the least common, accounting for less than 1% of cases, and are also radiolucent. Staghorn calculi, which involve the renal pelvis and extend into at least 2 calyces, are composed of triple phosphate and are more likely to develop in alkaline urine. Infections with Ureaplasma urealyticum and Proteus can increase the risk of their formation.
-
This question is part of the following fields:
- Surgery
-
-
Question 16
Incorrect
-
A 35-year-old male is being seen on the surgical ward round, four days after his abdominal surgery. He complains of a peculiar sensation over the wound while shifting in bed. Upon removing the dressings, it is discovered that the wound is gaping open, with visible internal organs. Despite this, his vital signs are all normal, and he does not seem to be bothered by the situation. The wound is covered with gauze impregnated with saline. While waiting for additional surgical assistance, what other urgent treatment should be provided?
Your Answer:
Correct Answer: IV ceftriaxone and metronidazole
Explanation:The initial management for abdominal wound dehiscence involves covering the wound with saline impregnated gauze and administering broad-spectrum antibiotics intravenously. In this case, a combination of ceftriaxone and metronidazole would be appropriate. Flucloxacillin is not broad enough to cover the range of organisms that may be present. While fluids are important, a 1 L stat bolus is excessive at this stage. Analgesia should be provided, but it is less urgent than antibiotics. Oxygen is not indicated based on the patient’s current condition.
Abdominal wound dehiscence is a serious issue that surgeons who perform abdominal surgery frequently encounter. It occurs when all layers of an abdominal mass closure fail, resulting in the protrusion of the viscera externally. This condition is associated with a 30% mortality rate and can be classified as either superficial or complete, depending on the extent of the wound failure.
Several factors increase the risk of abdominal wound dehiscence, including malnutrition, vitamin deficiencies, jaundice, steroid use, major wound contamination (such as faecal peritonitis), and poor surgical technique. To prevent this condition, the preferred method is the mass closure technique, also known as the Jenkins Rule.
When sudden full dehiscence occurs, the wound should be covered with saline impregnated gauze, and the patient should receive IV broad-spectrum antibiotics, analgesia, and IV fluids. Arrangements should also be made for a return to the operating theatre.
-
This question is part of the following fields:
- Surgery
-
-
Question 17
Incorrect
-
A 72-year-old man comes to the emergency department with abrupt onset of abdominal pain and fever. Upon examination, he appears ill and his abdomen is distended. His heart rate is 87/min, respiratory rate 27/min, blood pressure 143/93 mmHg, and temperature is 38.6 ºC. He has been experiencing constipation for the past week and has not passed air or feces. He has a history of active sigmoid cancer and type 2 diabetes that is managed with metformin. An erect chest x-ray reveals air beneath the left hemidiaphragm. What is the most appropriate surgical management plan?
Your Answer:
Correct Answer: Hartmann's procedure
Explanation:The appropriate surgical procedure for this patient is Hartmann’s procedure, which involves the removal of the rectum and sigmoid colon, formation of an end colostomy, and closure of the rectal stump. This is necessary due to the patient’s symptoms of perforation, which are likely caused by an occlusion from sigmoid cancer. A high anterior resection, left hemicolectomy, low anterior resection, and right hemicolectomy are not suitable options for this patient’s condition.
Colorectal cancer is typically diagnosed through CT scans and colonoscopies or CT colonography. Patients with tumors below the peritoneal reflection should also undergo MRI to evaluate their mesorectum. Once staging is complete, a treatment plan is formulated by a dedicated colorectal MDT meeting.
For colon cancer, surgery is the primary treatment option, with resectional surgery being the only cure. The procedure is tailored to the patient and tumor location, with lymphatic chains being resected based on arterial supply. Anastomosis is the preferred method of restoring continuity, but in some cases, an end stoma may be necessary. Chemotherapy is often offered to patients with risk factors for disease recurrence.
Rectal cancer management differs from colon cancer due to the rectum’s anatomical location. Tumors can be surgically resected with either an anterior resection or an abdominoperineal excision of rectum (APER). A meticulous dissection of the mesorectal fat and lymph nodes is integral to the procedure. Neoadjuvant radiotherapy is often offered to patients prior to resectional surgery, and those with obstructing rectal cancer should have a defunctioning loop colostomy.
Segmental resections based on blood supply and lymphatic drainage are the primary operations for cancer. The type of resection and anastomosis depend on the site of cancer. In emergency situations where the bowel has perforated, an end colostomy is often safer. Left-sided resections are more risky, but ileocolic anastomoses are relatively safe even in the emergency setting and do not need to be defunctioned.
-
This question is part of the following fields:
- Surgery
-
-
Question 18
Incorrect
-
A 50-year-old woman comes to the clinic with creamy nipple discharge. She had a mammogram screening a year ago which was normal. She smokes 10 cigarettes per day. Upon examination, there were no alarming findings. A repeat mammogram was conducted and no abnormalities were detected. Although she is concerned about the possibility of a tumor, she is not bothered by the discharge itself. Her serum prolactin level is provided below.
Prolactin 200 mIU/L (<600)
What is the most probable diagnosis and what would be the best initial treatment?Your Answer:
Correct Answer: Reassurance
Explanation:Duct ectasia does not require any specific treatment. However, lumpectomy may be used to treat breast masses if they meet certain criteria such as being small-sized and peripheral, and taking into account the patient’s preference. Mastectomy may be necessary for malignant breast masses if lumpectomy is not suitable. In young women with duct ectasia, microdochectomy may be performed if the condition is causing discomfort. It is also used to treat intraductal papilloma.
Understanding Duct Ectasia
Duct ectasia is a condition that affects the terminal breast ducts located within 3 cm of the nipple. It is a common condition that becomes more prevalent as women age. The condition is characterized by the dilation and shortening of the ducts, which can cause nipple retraction and creamy nipple discharge. It is important to note that duct ectasia can be mistaken for periductal mastitis, which is more common in younger women who smoke. Periductal mastitis typically presents with infections around the periareolar or subareolar areas and may recur.
When dealing with troublesome nipple discharge, treatment options may include microdochectomy for younger patients or total duct excision for older patients.
-
This question is part of the following fields:
- Surgery
-
-
Question 19
Incorrect
-
Which one of the following statements regarding varicoceles is accurate?
Your Answer:
Correct Answer: Over 80% occur on the left side
Explanation:Common Scrotal Problems and Their Features
Epididymal cysts, hydroceles, and varicoceles are the most common scrotal problems seen in primary care. Epididymal cysts are usually found posterior to the testicle and are separate from the body of the testicle. They may be associated with conditions such as polycystic kidney disease, cystic fibrosis, and von Hippel-Lindau syndrome. Diagnosis is confirmed by ultrasound, and management is usually supportive, although surgical removal or sclerotherapy may be attempted for larger or symptomatic cysts.
Hydroceles, on the other hand, describe the accumulation of fluid within the tunica vaginalis. They may be communicating or non-communicating, and may develop secondary to conditions such as epididymo-orchitis, testicular torsion, or testicular tumors. Hydroceles are usually soft, non-tender swellings of the hemi-scrotum that transilluminate with a pen torch. Diagnosis may be clinical, but ultrasound is required if there is any doubt about the diagnosis or if the underlying testis cannot be palpated. Management depends on the severity of the presentation, with infantile hydroceles generally repaired if they do not resolve spontaneously by the age of 1-2 years.
Varicoceles, on the other hand, are abnormal enlargements of the testicular veins that are usually asymptomatic but may be associated with subfertility. They are much more common on the left side and are classically described as a bag of worms. Diagnosis is confirmed by ultrasound with Doppler studies, and management is usually conservative, although surgery may be required if the patient is troubled by pain. There is ongoing debate regarding the effectiveness of surgery to treat infertility.
-
This question is part of the following fields:
- Surgery
-
-
Question 20
Incorrect
-
A 26-year-old male is brought in after a motorcycle accident. According to the paramedic, the patient has suffered a significant loss of blood due to an open femoral fracture, which has been reduced, and a haemothorax. The patient's blood pressure is 95/74 mmHg, and his heart rate is 128 bpm. Although conscious, the patient appears confused. What is the stage of haemorrhagic shock that this patient is experiencing?
Your Answer:
Correct Answer: Class III (30-40% blood loss)
Explanation:The patient is experiencing Class III haemorrhagic shock, indicated by their tachycardia and hypotension. They are not yet unconscious, ruling out Class IV shock. Class I shock would be fully compensated for, while Class II shock would only cause tachycardia. However, in Class III shock, confusion is also present. Class IV shock is characterized by severe hypotension and loss of consciousness.
Understanding Shock: Aetiology and Management
Shock is a condition that occurs when there is inadequate tissue perfusion. It can be caused by various factors, including sepsis, haemorrhage, neurogenic injury, cardiogenic events, and anaphylaxis. Septic shock is a major concern, with a mortality rate of over 40% in patients with severe sepsis. Haemorrhagic shock is often seen in trauma patients, and the severity is classified based on the amount of blood loss and associated physiological changes. Neurogenic shock occurs following spinal cord injury, leading to decreased peripheral vascular resistance and cardiac output. Cardiogenic shock is commonly caused by ischaemic heart disease or direct myocardial trauma. Anaphylactic shock is a severe hypersensitivity reaction that can be life-threatening.
The management of shock depends on the underlying cause. In septic shock, prompt administration of antibiotics and haemodynamic stabilisation are crucial. In haemorrhagic shock, controlling bleeding and maintaining circulating volume are essential. In neurogenic shock, peripheral vasoconstrictors are used to restore vascular tone. In cardiogenic shock, supportive treatment and surgery may be required. In anaphylactic shock, adrenaline is the most important drug and should be given as soon as possible.
Understanding the aetiology and management of shock is crucial for healthcare professionals to provide timely and appropriate interventions to improve patient outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 21
Incorrect
-
A 55-year-old man was brought to the emergency department with sudden abdominal pain and vomiting. The general surgeons diagnosed him with pancreatitis and he was given IV fluids and pain relief by the registrar. The FY1 was then asked to complete a Modified Glasgow Score to determine the severity of the pancreatitis. What information will the FY1 need to gather to complete this task?
Your Answer:
Correct Answer: Urea level
Explanation:The Modified Glasgow Score is utilized for predicting the severity of pancreatitis. If three or more of the following factors are identified within 48 hours of onset, it indicates severe pancreatitis: Pa02 <8 kPa, age >55 years, neutrophilia WBC >15×10^9, calcium <2mmol/L, renal function urea >16 mmol/L, enzymes LDH >600 ; AST >200, albumin <32g/L, and blood glucose >10 mmol/L. To remember these factors easily, one can use the acronym PANCREAS. This information can be found in the Oxford Handbook of Clinical Medicine, 9th edition, on pages 638-639.
Acute pancreatitis is a condition that is mainly caused by gallstones and alcohol in the UK. A popular mnemonic to remember the causes is GET SMASHED, which stands for gallstones, ethanol, trauma, steroids, mumps, autoimmune diseases, scorpion venom, hypertriglyceridaemia, hyperchylomicronaemia, hypercalcaemia, hypothermia, ERCP, and certain drugs. CT scans of patients with acute pancreatitis show diffuse parenchymal enlargement with oedema and indistinct margins. It is important to note that pancreatitis is seven times more common in patients taking mesalazine than sulfasalazine.
-
This question is part of the following fields:
- Surgery
-
-
Question 22
Incorrect
-
A 62-year-old man presents to the pre-admission clinic for assessment prior to an elective prostatectomy. You find no adverse past medical history and examination is unremarkable. An electrocardiogram (ECG) is indicated in all pre-operative patients undergoing major surgery who are over the age of 60. The ECG is shown below.
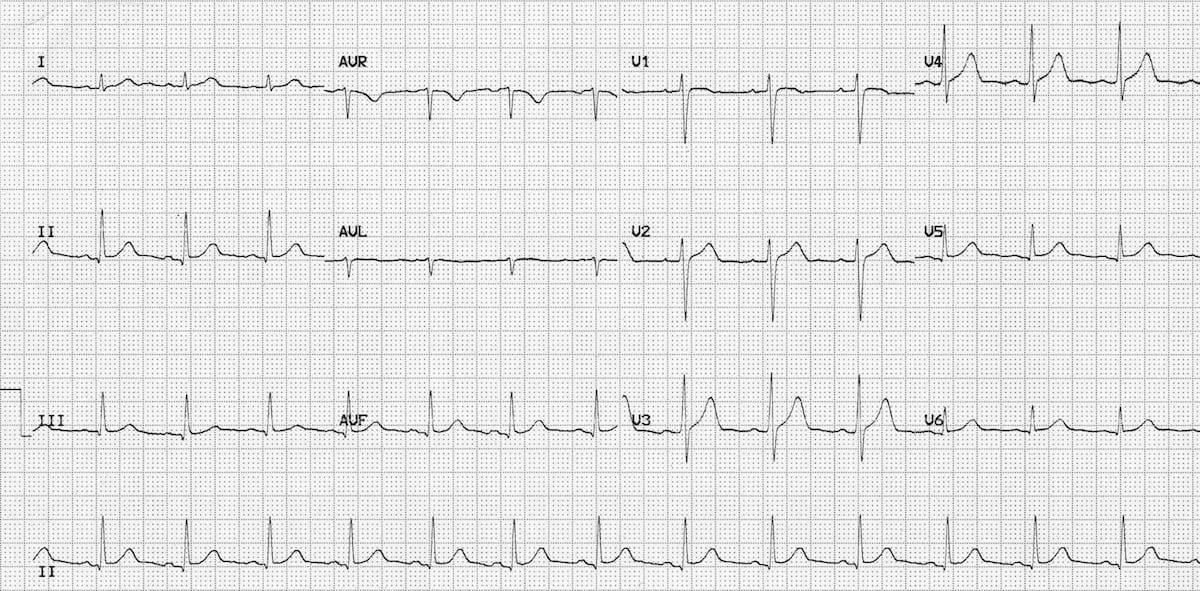 After having reviewed the ECG, what is the next best step to take with this patient?
After having reviewed the ECG, what is the next best step to take with this patient? Your Answer:
Correct Answer: No further assessment is required
Explanation:Assessing Cardiac Risk in Preoperative Patients: Common Misconceptions
There are several misconceptions when it comes to assessing cardiac risk in preoperative patients. One common mistake is assuming that all patients require extensive cardiac testing, even when there are no significant risk factors or symptoms present. For example, if a patient has no significant past medical history and their examination is unremarkable, an echocardiogram is not necessary.
On the other hand, some clinicians may be too cautious and cancel a patient’s procedure based on a perceived cardiac risk that is not supported by evidence. If the patient’s ECG is normal and there are no cardiac risk factors, cancelling the procedure would be unreasonable.
It is important to recognise that not all preoperative patients require extensive cardiac testing. Instead, clinicians should focus on identifying patients with specific cardiac conditions that require closer monitoring and management. By avoiding unnecessary testing and interventions, clinicians can improve patient outcomes and reduce healthcare costs.
-
This question is part of the following fields:
- Surgery
-
-
Question 23
Incorrect
-
A 29-year-old man has been waiting for surgery to repair a right inguinal hernia. He is now admitted with abdominal distension and colicky pain, along with vomiting bile and no bowel movements for two days. He is typically healthy and not on any medication. On examination, he appears dehydrated with a red, tender swelling in the right groin. X-rays confirm a small bowel obstruction, and a nasogastric tube is inserted. What is the most appropriate course of treatment for this patient?
Your Answer:
Correct Answer: Surgery with decompression of the bowel and hernia repair
Explanation:Management of Small Bowel Obstruction
Small bowel obstruction is a condition that requires a certain diagnosis before surgery. However, in cases where the cause of the obstruction is an obstructed groin hernia, a contrast study or ultrasound scan of the groin is unnecessary. The patient should be well resuscitated and undergo surgery to reduce and inspect the bowel for viability. Repair of the hernia should proceed, and inspection of incarcerated bowel is important.
In cases of adhesional obstruction, expectant drip and suck management may be appropriate, as the obstruction may settle with adequate decompression of the bowel. A contrast study may also be helpful in incomplete obstruction, as gastrografin has a therapeutic laxative effect. However, indications for surgery in bowel obstruction are an obstructed hernia and signs of peritonism, which indicate ischaemic bowel.
In summary, the management of small bowel obstruction depends on the cause of the obstruction. In cases of an obstructed groin hernia, surgery is necessary, while expectant management may be appropriate in adhesional obstruction. A contrast study may also be helpful in incomplete obstruction. It is important to consider the indications for surgery, such as signs of peritonism, to prevent further complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 24
Incorrect
-
A 30-year-old female without underlying medical conditions undergoes a tonsillectomy and suddenly experiences a fever spike up to 40°C. Her heart rate increases to 160 beats per minute and her systolic blood pressure is measured at 180 mmHg. Additionally, the patient displays signs of muscle rigidity in her limbs. Prior to the surgery, her pre-anesthetic evaluation was unremarkable, and there is no known family history of neuromuscular disease or complications during surgery or anesthesia. The patient was induced with propofol and suxamethonium.
What is the definitive treatment for this patient in this situation?Your Answer:
Correct Answer: Dantrolene
Explanation:Suxamethonium can cause malignant hyperthermia in susceptible individuals, which is a serious side effect that requires treatment with IV dantrolene. Malignant hyperthermia is a genetic disorder that causes a hypermetabolic crisis, including hypercapnia, tachycardia, muscle rigidity, rhabdomyolysis, hyperthermia, and arrhythmia. It is often associated with volatile inhalational anesthetics and suxamethonium. Dantrolene is the only effective treatment for malignant hyperthermia and should be given intravenously. There is no evidence to support the use of IV hydrocortisone in the treatment of malignant hyperthermia. Flumazenil is an antidote for benzodiazepine overdose, while N-acetylcysteine is an antidote for paracetamol overdose.
Understanding Neuromuscular Blocking Drugs
Neuromuscular blocking drugs are commonly used in surgical procedures as an adjunct to anaesthetic agents. These drugs are responsible for inducing muscle paralysis, which is a necessary prerequisite for mechanical ventilation. There are two types of neuromuscular blocking drugs: depolarizing and non-depolarizing.
Depolarizing neuromuscular blocking drugs bind to nicotinic acetylcholine receptors, resulting in persistent depolarization of the motor end plate. On the other hand, non-depolarizing neuromuscular blocking drugs act as competitive antagonists of nicotinic acetylcholine receptors. Examples of depolarizing neuromuscular blocking drugs include succinylcholine (also known as suxamethonium), while examples of non-depolarizing neuromuscular blocking drugs include tubcurarine, atracurium, vecuronium, and pancuronium.
While these drugs are effective in inducing muscle paralysis, they also come with potential adverse effects. Depolarizing neuromuscular blocking drugs may cause malignant hyperthermia and transient hyperkalaemia, while non-depolarizing neuromuscular blocking drugs may cause hypotension. However, these adverse effects can be reversed using acetylcholinesterase inhibitors such as neostigmine.
It is important to note that suxamethonium is contraindicated for patients with penetrating eye injuries or acute narrow angle glaucoma, as it increases intra-ocular pressure. Additionally, suxamethonium is the muscle relaxant of choice for rapid sequence induction for intubation and may cause fasciculations. Understanding the mechanism of action and potential adverse effects of neuromuscular blocking drugs is crucial in ensuring their safe and effective use in surgical procedures.
-
This question is part of the following fields:
- Surgery
-
-
Question 25
Incorrect
-
A 45-year-old man with a history of alcohol abuse presents to your clinic after being diagnosed with chronic pancreatitis. You inform him that this diagnosis increases his likelihood of developing diabetes mellitus. What tests should you suggest to assess his risk for this condition?
Your Answer:
Correct Answer: Annual HbA1c
Explanation:Type 3c diabetes mellitus is a rare complication of pancreatitis that is more difficult to manage than type 1 or 2 diabetes mellitus due to the accompanying exocrine insufficiency, which leads to malabsorption and malnutrition. The development of diabetes mellitus may take years after the onset of pancreatitis, necessitating lifelong monitoring through annual HbA1c measurements. An ultrasound of the pancreas will not provide any indication of diabetes development. Additionally, it is crucial to counsel the patient on their alcohol misuse, as it may exacerbate their pancreatitis.
Understanding Chronic Pancreatitis
Chronic pancreatitis is a condition characterized by inflammation that can affect both the exocrine and endocrine functions of the pancreas. While alcohol excess is the leading cause of this condition, up to 20% of cases are unexplained. Other causes include genetic factors such as cystic fibrosis and haemochromatosis, as well as ductal obstruction due to tumors, stones, and structural abnormalities like pancreas divisum and annular pancreas.
Symptoms of chronic pancreatitis include pain that worsens 15 to 30 minutes after a meal, steatorrhoea, and diabetes mellitus. Abdominal x-rays can show pancreatic calcification in 30% of cases, while CT scans are more sensitive at detecting calcification with a sensitivity of 80% and specificity of 85%. Functional tests like faecal elastase may be used to assess exocrine function if imaging is inconclusive.
Management of chronic pancreatitis involves pancreatic enzyme supplements, analgesia, and antioxidants, although the evidence base for the latter is limited. It is important to understand the causes, symptoms, and management of chronic pancreatitis to effectively manage this condition.
-
This question is part of the following fields:
- Surgery
-
-
Question 26
Incorrect
-
A 65-year-old woman undergoes a right hemicolectomy for colon cancer and four days later presents with vomiting, a distended abdomen, and absent bowel sounds. Her blood results show a CRP of 124 mg/l and a WBC count of 5.2 * 109/l. Nursing notes reveal no bowel movements since surgery. What is the probable cause of her clinical presentation?
Your Answer:
Correct Answer: Paralytic ileus
Explanation:Simple constipation is unlikely in this patient due to the presence of vomiting and absent bowel sounds, which suggests paralytic ileus, especially so soon after surgery. Additionally, constipation alone would not explain all of the patient’s symptoms and signs. As the patient underwent a right hemicolectomy, the caecum would have been removed, making caecal volvulus an unlikely diagnosis. The raised CRP is a normal response to surgery. While peritonitis is a possibility, it would typically present with severe abdominal pain, tenderness, guarding, and more significantly elevated inflammatory markers and fever. Hirschsprung’s disease, a congenital condition, is highly unlikely to present for the first time in a 67-year-old patient.
Postoperative ileus, also known as paralytic ileus, is a common complication that can occur after bowel surgery, particularly if the bowel has been extensively handled. This condition is characterized by a reduction in bowel peristalsis, which can lead to pseudo-obstruction. Symptoms of postoperative ileus include abdominal distention, bloating, pain, nausea, vomiting, inability to pass flatus, and difficulty tolerating an oral diet. It is important to check for deranged electrolytes, such as potassium, magnesium, and phosphate, as they can contribute to the development of postoperative ileus.
The management of postoperative ileus typically involves starting with nil-by-mouth and gradually progressing to small sips of clear fluids. If vomiting occurs, a nasogastric tube may be necessary. Intravenous fluids are administered to maintain normovolaemia, and additives may be used to correct any electrolyte disturbances. In severe or prolonged cases, total parenteral nutrition may be required. It is important to monitor the patient closely and adjust the treatment plan as necessary to ensure a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 27
Incorrect
-
A 55-year-old woman with ulcerative colitis and primary sclerosing cholangitis visits her GP complaining of colicky abdominal pain and pruritus that has persisted despite taking ursodeoxycholic acid. She also reports unintentional weight loss of 5kg over two months. During the examination, the patient appears mildly jaundiced and a mass is palpable in the right hypochondrium. What screening test can be performed to detect the probable malignancy?
Your Answer:
Correct Answer: CA 19-9
Explanation:Understanding Cholangiocarcinoma
Cholangiocarcinoma, also known as bile duct cancer, is a type of cancer that affects the bile ducts. The main risk factor for this type of cancer is primary sclerosing cholangitis. Symptoms of cholangiocarcinoma include persistent biliary colic, anorexia, jaundice, and weight loss. A palpable mass in the right upper quadrant, known as the Courvoisier sign, may also be present. Additionally, periumbilical lymphadenopathy, known as Sister Mary Joseph nodes, and left supraclavicular adenopathy, known as Virchow node, may be seen. CA 19-9 levels are often used to detect cholangiocarcinoma in patients with primary sclerosing cholangitis. It is important to be aware of these symptoms and risk factors in order to detect and treat cholangiocarcinoma early.
-
This question is part of the following fields:
- Surgery
-
-
Question 28
Incorrect
-
A patient in their 60s with severe intermittent claudication undergoes an axillo-bifemoral bypass. Two days after the operation, they develop pain in the leg. Examination reveals a warm, erythaematous swelling in the groin.
What complication has occurred?Your Answer:
Correct Answer: The graft has become infected
Explanation:Possible Complications of a Graft Procedure
Graft procedures are commonly performed to improve blood flow in patients with peripheral arterial disease. However, like any surgical intervention, there are potential complications that may arise. One possible complication is an infected graft, which can cause swelling and abscess formation. Another possibility is graft occlusion, which may occur if there is a surgical error and can lead to the recurrence of claudication symptoms. An anastomotic aneurysm is another rare but serious complication that may cause pulsatile swelling. Embolism is more likely to occur in patients with aneurysmal disease and can present with acute limb ischaemia or petechiae. Finally, an anastomotic leak is an extremely rare complication that may cause sudden pain and swelling at the site of the graft. It is important for patients to be aware of these potential complications and to seek medical attention if they experience any concerning symptoms after a graft procedure.
-
This question is part of the following fields:
- Surgery
-
-
Question 29
Incorrect
-
A 55-year-old woman comes to the clinic with a complaint of bloody discharge from her left nipple. She is also a perimenopausal woman who has two grown children that were born after normal labour and delivery and breastfed. She is not currently taking hormone replacement therapy. Upon physical examination, there are no signs of lumps, asymmetry, or dimpling of the skin or nipple. When pressure is applied to the nipple, a small amount of bloody fluid is expressed. What is the probable cause of her presenting symptom?
Your Answer:
Correct Answer: Intraductal papilloma
Explanation:The most likely cause of blood-stained nipple discharge is intraductal papilloma, a benign tumor that grows within the lactiferous duct. This condition does not usually present with a palpable lump, but larger papillomas may cause a mass. Unlike intraductal papilloma, ductal carcinoma in situ is a type of non-invasive breast cancer that may or may not cause bloody nipple discharge. However, intraductal papilloma is a more common cause of this symptom. Mammary duct ectasia, on the other hand, is a benign breast condition that causes thick, green-tinged discharge, unlike the blood-stained discharge seen in this case. Mastitis, an inflammation of the breast tissue, can also cause bloody nipple discharge, but it is more commonly associated with pain, heat, erythema, fever, and sometimes a lump. This condition is also more prevalent in breastfeeding or lactating women, which is not the case for this patient.
Understanding Nipple Discharge: Causes and Assessment
Nipple discharge is a common concern among women, and it can be caused by various factors. Physiological discharge occurs during breastfeeding, while galactorrhea may be triggered by emotional events or certain medications. Hyperprolactinemia, which is often associated with pituitary tumors, can also cause nipple discharge. Mammary duct ectasia, which is characterized by the dilation of breast ducts, is common among menopausal women and smokers. On the other hand, nipple discharge may also be a sign of more serious conditions such as carcinoma or intraductal papilloma.
To assess patients with nipple discharge, a breast examination is necessary to determine the presence of a mass lesion. If a mass lesion is suspected, triple assessment is recommended. Reporting of investigations follows a system that uses a prefix denoting the type of investigation and a numerical code indicating the abnormality found. For non-malignant nipple discharge, endocrine disease should be excluded, and smoking cessation advice may be given for duct ectasia. In severe cases of duct ectasia, total duct excision may be necessary.
Understanding the causes and assessment of nipple discharge is crucial in providing appropriate management and treatment. It is important to seek medical attention if nipple discharge persists or is accompanied by other symptoms such as pain or a lump in the breast.
-
This question is part of the following fields:
- Surgery
-
-
Question 30
Incorrect
-
A 35-year-old woman who is a heavy smoker presents with recurring infections in her right breast. During examination, an indurated area is found at the lateral aspect of the nipple areolar complex. Imaging reveals no mass lesions. What is the probable diagnosis?
Your Answer:
Correct Answer: Periductal mastitis
Explanation:Recurrent infections are a common symptom of periductal mastitis in smokers, which can be treated with co-amoxiclav. Additionally, Mondor’s disease of the breast is characterized by a localized thrombophlebitis of a breast vein.
Understanding Mastitis: Inflammation of the Breast Tissue
Mastitis is a condition that refers to the inflammation of the breast tissue, which is commonly associated with breastfeeding. It affects around 1 in 10 women and is characterized by a painful, tender, and red hot breast. Other symptoms may include fever and general malaise.
The first-line management of mastitis is to continue breastfeeding, as simple measures such as analgesia and warm compresses can help alleviate the symptoms. However, if the patient is systemically unwell, has a nipple fissure, or if symptoms do not improve after 12-24 hours of effective milk removal, treatment with antibiotics may be necessary. The first-line antibiotic for mastitis is oral flucloxacillin, which should be taken for 10-14 days. This reflects the fact that the most common organism causing infective mastitis is Staphylococcus aureus.
It is important to note that breastfeeding or expressing should continue during antibiotic treatment. If left untreated, mastitis may develop into a breast abscess, which generally requires incision and drainage. Therefore, it is crucial to seek medical attention if symptoms persist or worsen. Understanding mastitis and its management can help ensure the health and well-being of both the mother and the baby.
-
This question is part of the following fields:
- Surgery
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)