-
Question 1
Incorrect
-
Question 2
Correct
-
Which of the following is suggestive of ovulation:
Your Answer: Regular cycle with dysmenorrhea
Explanation:Ovulation in the menstrual cycle usually occurs over 4 days. There is an increase in basal body temperature at the time of ovulation due to the effect of progesterone.
A high Day 21 progesterone level indicates ovulation and the release of an egg.
Dysmenorrhea is described as painful menstruation. The symptoms start at the time of ovulation and persist till menstruation.
-
This question is part of the following fields:
- Physiology
-
-
Question 3
Correct
-
Regarding cardiac output in pregnancy which of the following statements is TRUE?
Your Answer: Cardiac output increases by approximately 40-50% during pregnancy
Explanation:In a non pregnant adult female the cardiac output is 4.5L/min, by the 20 week of pregnancy the cardiac output increases by 40% to 6.3L/min. During early stages of labour it increases further still by 17% to 7.3L/min.
-
This question is part of the following fields:
- Physiology
-
-
Question 4
Correct
-
Which one of the following features indicates complete placental separation after delivery?
Your Answer: All of the options given
Explanation:At the time of delivery, the most important signs of complete placental separation are lengthening of the umbilical cord, per vaginal bleeding and change in shape of uterus from discoid to globular shape. The uterus contracts in size and rises upward.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 5
Incorrect
-
Adult Polycystic Kidney Disease (PKD) typically follows which pattern of inheritance
Your Answer: Autosomal Recessive
Correct Answer: Autosomal Dominant
Explanation:Polycystic kidney disease (PKD) can either be autosomal dominant or recessive. The autosomal dominant variant is more common in adult PKD however, the recessive pattern is more common in infantile PKD.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 6
Correct
-
A 31 year old is being seen in EPU and you are asked to review her ultrasound. There is a solid collection of echoes with numerous small (3-10 mm) anechoic spaces. What is the likely diagnosis?
Your Answer: Molar Pregnancy
Explanation:This is typical appearance of molar pregnancy. This used to be referred to as ‘snowstorm sign’ as with older poorer resolution ultrasound the anechoic species looked like a snowstorm.
-
This question is part of the following fields:
- Data Interpretation
-
-
Question 7
Correct
-
Renal cell carcinoma is associated with which type of metastasis?
Your Answer: Haematogenous
Explanation:Most carcinomas spread primarily via lymphatic invasion. Renal cell is the exception spreading via the bloodstream.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 8
Incorrect
-
A 29 year old female presented at her 38th week of gestation to the ER with severe hypertension (210/100) and proteinuria (+++). Soon after admission, she developed generalized tonic clonic fits. What is the first line of management in this case?
Your Answer: Immediate delivery
Correct Answer: Magnesium sulphate IV
Explanation:Magnesium Sulphate is the drug of choice in eclamptic patients. A loading dose of 4g magnesium sulphate in 100mL 0.9% saline IVI over 5min followed by maintenance IVI of 1g/h for 24h. Signs of toxicity include respiratory depression and jerky tendon reflexes. In recurrent fits additional 2g can be given. Magnesium should be stopped when the respiratory rate is <14/min, absent tendon reflexes, or urine output is <20mL/h.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 9
Correct
-
With sneezing, a 45-year-old mother of two reported leaking a small bit of urine. It started to happen with exercising recently. She denies having experienced recent life pressures. Which of the following best characterizes the incontinence she's dealing with?
Your Answer: Stress incontinence
Explanation:Overflow incontinence typically presents with continuous urinary leakage or dribbling in the setting of incomplete bladder emptying. Associated symptoms can include weak or intermittent urinary stream, hesitancy, frequency, and nocturia. When the bladder is very full, stress leakage can occur or low-amplitude bladder contractions can be triggered resulting in symptoms similar to stress or urgency incontinence.
Women with urgency incontinence experience the urge to void immediately preceding or accompanied by involuntary leakage of urine
Individuals with stress incontinence have involuntary leakage of urine that occurs with increases in intraabdominal pressure (e.g., with exertion, sneezing, coughing, laughing) in the absence of a bladder contraction.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 10
Correct
-
A 48-year-old woman presented to you with a breast mass. On examination, it is hard, irregular and ill defined. The surface of the breast is slightly bruised however, there is no discharge. The most probable diagnosis is?
Your Answer: Fat necrosis
Explanation:Fat necrosis is often a result of a trauma or surgery. In fat necrosis the enzyme lipase releases fatty acids from triglycerides. The fatty acids combine with calcium to form soaps. These soaps appear as white chalky deposits which are firm lumps with no associated discharge. The given case has a bruise which indicates prior trauma.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 11
Correct
-
A 34 year old patient is being investigated in the infertility clinic and is offered Hysterosalpingography (HSG). She has 28 day cycles. Which of the following statements regarding HSG is correct?
Your Answer: Typically performed using iodine based water soluble contrast
Explanation:Hysterosalpingography is used to assess the patency of the fallopian tubes. It is performed by injection of a radio-opaque iodine based contrast. This test is contraindicated in pelvic inflammatory disease and during pregnancy. Should be performed in Follicular phase of menstrual cycle after cessation of menstrual bleeding and prior to ovulation (days 6-12).
-
This question is part of the following fields:
- Biophysics
-
-
Question 12
Correct
-
Endometrial ablation is a medical technique that removes or destroys the endometrial lining in women who have severe monthly flow. Endometrial ablation is not contraindicated by which of the following?
Your Answer: Completed family
Explanation:Endometrial ablation is primarily intended to treat premenopausal women with heavy menstrual bleeding (HMB) who do not desire future fertility. Women who choose endometrial ablation often have failed or declined medical management.
Absolute contraindications to endometrial ablation include pregnancy, known or suspected endometrial hyperplasia or cancer, desire for future fertility, active pelvic infection, IUD currently in situ, and being post-menopausal. In general, endometrial ablation should be avoided in patients with congenital uterine anomalies, severe myometrial thinning, and uterine cavity lengths that exceed the capacity of the ablative technique (usually greater than 10-12 cm).
-
This question is part of the following fields:
- Gynaecology
-
-
Question 13
Incorrect
-
A 23-year-old woman presents to the local hospital clinic for her first antenatal visit. She is primigravid at 39 weeks of gestation (exact dates uncertain). She has just arrived from overseas, and no antenatal care had been available in her origin country. On examination, BP is 120/80 mmHg. The fundal height is 30cm above the pubic symphysis. Fetal heart sounds are present at a rate of 144/min. Pelvic examination indicates a long, closed cervix. The baby is noted to be in cephalic presentation. What is the appropriate choice for initial management of this woman?
Your Answer: Amniocentesis.
Correct Answer: Ultrasound examination.
Explanation:In this case, the fundus height appears to be smaller than the suggested dates of gestation. However, this is uncertain as the exact gestation dates are not known. Head-sparing intrauterine growth restriction needs to be excluded or managed appropriately if detected.
The best initial management step would be to perform an ultrasound examination (correct answer). This would enable complete assessment of the foetus and all the measurable parameters can be determined. This would aid in identifying any discrepancy in size of the abdomen, limbs and head, and the liquor volume (amniotic fluid index) could be evaluated.
If asymmetrical growth restriction was detected via ultrasound examination, further evaluations such as cardiotocography (CTG) and umbilical arterial wave form analysis by Doppler could be initiated.
Additionally, foetal movement counting could then be commenced and evaluation of foetal lung maturity by amniocentesis could be considered.
If the ultrasound was normal (no evidence of asymmetrical growth restriction, normal amniotic fluid), repeat ultrasound should be performed after two weeks to evaluate the foetal growth.
If normal growth is observed on the repeat ultrasound, the estimated due date can be calculated (assuming normal foetal growth around the 50th percentile for the population).
-
This question is part of the following fields:
- Gynaecology
-
-
Question 14
Correct
-
A patient attends the maternity unit as her waters have broken but she hasn't had contractions. She is 39+6 weeks gestation. Speculum examination confirms prelabour rupture of membranes. What is the likelihood of spontaneous labour starting within 24 hours?
Your Answer: 60%
Explanation:In pregnancy, term refers to the gestational period from 37 0 to 41 6 weeks. Preterm births occur between 24 0 and 36 6 weeks. 60% of the women will go into labour with in 24 hours in PPROM. After 24 hours have past without any contraction and the gestation age is more than 34 week than prostaglandins can be used to augment labour.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 15
Correct
-
A patient undergoes oophorectomy and the ovarian veins are ligated. Which vein does the left ovary drain into?
Your Answer: Left renal
Explanation:When it comes to questions on venous drainage the ovarian vein is likely to be a common question given its varied drainage depending on laterality. The right ovarian vein travels through the suspensory ligament of the ovary and generally joins the inferior vena cava whereas the left ovarian vein drains into the left renal vein.
-
This question is part of the following fields:
- Anatomy
-
-
Question 16
Incorrect
-
A 28-year-old lady is complaining of mucopurulent vaginal discharge. On examination, copious amounts of thick mucoid material is found to be draining out of a large cervical erosion. She has had regular pap smears since 16 years of age, which have all been normal. Her last smear was done 4 months prior. What is the best next step in her management?
Your Answer: Colposcopic examination of the cervix.
Correct Answer: Cauterisation of the cervix.
Explanation:The best next step in management would be to remove the cervical ectropion using cautery. This would usually be performed under anaesthesia. It can take up to a month to heal following the procedure. Vaginal pessaries and antibiotics are typically not effective.
Indications for a cone biopsy include an abnormal pap smear, lesion suspected to be a CIN on colposcopic examination that cannot be fully visualised as well if there is a histological discrepancy between the smear and biopsy. Colposcopic examination is also unnecessary at this stage since she has not complained of any abnormal per vaginal bleed nor is her last pap smear abnormal.
Since the discharge is now affecting the patient’s life, treatment should be given so reassuring her that no treatment is needed is not appropriate.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 17
Correct
-
A women in her 21-weeks of pregnancy, complaints of palpitations, sweating of palms, and increased nervousness. Along with TSH what other investigations should be done for this patient?
Your Answer: Free T4
Explanation:Patient mentioned in the case has developed thyrotoxicosis during pregnancy. TSH level should be tested, and if the result shows any suppressed or elevated TSH level, then it is mandatory to check for free T4 level.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 18
Correct
-
Which of the following hormones are required for alveolar morphogenesis during pregnancy?
Your Answer: Progesterone, Prolactin and hPL
Explanation:The changes seen in breast tissue with the menstrual cycle are accentuated during pregnancy. Deposition of fat around glandular tissue occurs, and the number of glandular ducts is increased by oestrogen, while progesterone and human placental lactogen (hPL) increase the number of gland alveoli. Prolactin is essential for the stimulation of milk secretion and during pregnancy prepares the alveoli for milk production. Although prolactin concentration increases throughout pregnancy, it does not then result in lactation since it is antagonized at an alveolar receptor level by oestrogen.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 19
Correct
-
A 27 year old women presents with a history of vaginal spotting and cramping abdominal pain. She has an 8 week history of amenorrhoea. On examination urine pregnancy test is positive and the cervix is closed. What is the likely diagnosis?
Your Answer: Threatened Miscarriage
Explanation:Miscarriage is a pregnancy that ends spontaneously before the foetus reaches the age of viability i.e. before 24 weeks of gestation. In a threatened miscarriage the USG findings are of a foetus present in the uterus and on speculum examination the cervical OS is closed, in an inevitable miscarriage the cervical OS is opened. In an incomplete miscarriage the uterus contains the retained products of conception and the cervical OS is open. complete miscarriage contains no retained products of conception and the cervix is closed as the bleeding as resolved.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 20
Incorrect
-
A 30-year-old primigravida woman presented to the clinic for her first antenatal check-up. Upon interview, it was noted that she was taking folic acid along with some other nutritional supplements as medication. All of the following are considered correct regarding neural tube defects and folate before and during pregnancy, except:
Your Answer: Women taking carbamazepine should take high-dose folate supplement
Correct Answer: Prevalence of neural tube defects among non-indigenous population is almost double than that in Aboriginal and Torres Strait Islander babies
Explanation:Neural tube defects (NTDs) are common complex congenital malformations resulting from failure of the neural tube closure during embryogenesis. It is established that folic acid supplementation decreases the prevalence of NTDs, which has led to national public health policies regarding folic acid.
Neural tube defects (NTD) were 43% more common in Indigenous than in non-Indigenous infants in Western Australia in the 1980s, and there has been a fall in NTD overall in Western Australia since promotion of folate and voluntary fortification of food has occurred.
Women should take 5 mg/d of folic acid for the 2 months before conception and during the first trimester.
Women planning pregnancy might be exposed to medications with known antifolate activities affecting different parts of the folic acid metabolic cascade. A relatively large number of epidemiologic studies have shown an increased risk of NTDs among babies exposed in early gestation to antiepileptic drugs (carbamazepine, valproate, barbiturates), sulphonamides, or methotrexate. Hence, whenever women use these medications, or have used them near conception, they should take 5 mg/d of folic acid until the end of the first trimester of pregnancy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 21
Correct
-
What is the contraception of choice for epileptics on enzyme inducing antiepileptic drugs?
Your Answer: Levonorgestrel-releasing intrauterine contraceptive device.
Explanation:Clinical decision making which contraceptive regimen is optimal for an individual woman with epilepsy is one of the most challenging tasks when taking care of women with epilepsy. The bidirectional interactive potential of antiepileptic drugs (AEDs) and hormonal contraceptives needs to be taken into account. Enzyme inducing (EI)-AEDs may reduce the contraceptive efficacy of hormonal contraceptives.
If combined oral contraceptives (COCs) are used in combination with EI-AEDs, it is recommended to choose a COC containing a high progestin dose, well above the dose needed to inhibit ovulation, and to take the COC pill continuously (“long cycle therapy”). But even with the continuous intake of a COC containing a higher progestin dose contraceptive safety cannot be guaranteed, thus additional contraceptive protection may be recommended.
Progestin-only pills (POPs) are likely to be ineffective, if used in combination with EI-AEDs.
Subdermal progestogen implants are not recommended in patients on EI-AEDs, because of published high failure rates.
Depot medroxyprogesterone-acetate (MPA) injections appear to be effective, however they may not be first choice due to serious side effects (delayed return to fertility, impaired bone health).
The use of intrauterine devices is an alternative method of contraception in the majority of women, with the advantage of no relevant drug–drug interactions. The levonorgestrel intrauterine system (IUS) appears to be effective, even in women taking EI-AEDs. Likelihood of serious side effects is low in the IUS users.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 22
Correct
-
Which ONE among the following factors does not increase the risk for developing postpartum endometritis?
Your Answer: Advanced maternal age
Explanation:The most common clinical findings in a postpartum women with endometritis are postpartum fever, with tachycardia relative to the rise in temperature, midline lower abdominal pain and uterine tenderness from the 2nd to 10th day of postpartum.
Most common risk factors for the development of postpartum endometritis are:
– Cesarean deliveries are considered as the most important risk factor for postpartum endometritis, especially those performed after the onset of labour.
– Young maternal age.
– Multiple digital cervical examinations.
– Prolonged rupture of membranes.
– Retention of placental products.
– Prolonged labour.
– Chorioamnionitis.
Advanced maternal age is not considered as a risk factor for development of postpartum endometritis. -
This question is part of the following fields:
- Obstetrics
-
-
Question 23
Correct
-
During pregnancy, maternal oestrogen levels increase markedly. Most of this oestrogen is produced by the:
Your Answer: Placenta
Explanation:The placenta does not have all the necessary enzymes to make oestrogens from cholesterol, or even progesterone. Human trophoblast lack 17-hydroxylase and therefore cannot convert C21-steroids to C19-steroids, the immediate precursors of oestrogen. To bypass this deficit, dehydroisoandrosterone sulphate (DHA) from the fetal adrenal is converted to estradiol-17ί by trophoblasts. In its key location as a way station between mother and foetus, placenta can use precursors from either mother or foetus to circumvent its own deficiencies in enzyme activities.
-
This question is part of the following fields:
- Physiology
-
-
Question 24
Correct
-
Multiple Gestation is frequently associated with all of the following EXCEPT:
Your Answer: Post-maturity
Explanation:Multiple pregnancy is considered a high risk for obstetric complications such as spontaneous abortion, hypertensive disorders, placenta previa, and fetal malformations. Specifically, the incidence of hypertensive disorders, a common source of maternal morbidity, is 15% to 35% in twin pregnancies, which is two to five times higher than in singleton pregnancies. Additionally, the aetiology of preterm birth is not completely understood, but the association between multiple pregnancy and preterm birth is well known. A secondary analysis of the WHO Global Survey dataset indicated that 35.2% of multiple births were preterm (< 37 weeks gestation); of all multiple births, 6.1% of births were before 32 weeks gestation, 5.8% were during weeks 32 and 33, and 23.2% were during weeks 34 through 37
-
This question is part of the following fields:
- Obstetrics
-
-
Question 25
Correct
-
A 24 week pregnant patient complains of itching over the past 6 weeks particularly to the hands and feet which is worse at night. She has taken cetirizine but this hasn't settled her symptoms. Examination is unremarkable with no rash. What is the likely diagnosis?
Your Answer: Intrahepatic Cholestasis of Pregnancy
Explanation:The history is typical of Intrahepatic Cholestasis of Pregnancy, also known as obstetric cholestasis and prurigo gravidarum. It is characterised by itching without rash and abnormal LFTs beyond normal pregnancy ranges. Itching affects around 23% of pregnancies and can occur before biochemical changes.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 26
Incorrect
-
According to the RCOG Green-top guidelines on prevention and management of post-partum haemorrhage (PPH) which of the following statements is true?
Your Answer: Prophylactic oxytocics reduce the risk of PPH by about 30%
Correct Answer: For women delivering by caesarean section, Oxytocin 5 iu by slow IV injection should be used
Explanation:Misoprostol is not as effective as oxytocin but may be used if Oxytocin is not available e.g. home birth Recommended doses of Oxytocin For vaginal deliveries: 5 iu or 10 iu by intramuscular injection. For C-section: 5 iu by IV injection
-
This question is part of the following fields:
- Clinical Management
-
-
Question 27
Correct
-
Which one of the following methods helps determine the fetal position and presentation?
Your Answer: Leopold's manoeuvre
Explanation:Fetal position and presentation is best evaluated by Leopold’s manoeuvre. It will determine which part of the foetus is in the uterine fundus.
Cullen’s sign is found in ruptured ectopic pregnancy characterised by bruising and oedema of the periumbilical region.
Mauriceau-Smelli-Veit manoeuvre is done during a breech delivery. -
This question is part of the following fields:
- Obstetrics
-
-
Question 28
Correct
-
Looking at the picture below what is the diagnosis?
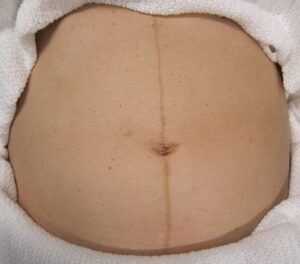
Your Answer: Linea Nigra
Explanation:This is Linea Nigra. It occurs in 3/4 of pregnancies and is due to increased melanocyte-stimulating hormone production by the placenta. This also causes melasma and darkening of the nipples.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 29
Correct
-
Question 30
Correct
-
A 21-year old female, gravida 1 para 0, term pregnancy, comes in due to labour for eight hours. Two hours prior to onset of contractions, her membranes have allegedly ruptured. Fetal heart rate is at 144/min. Contractions are of good quality, noted every 2-3 minutes, with a duration of 45 seconds. On examination, her cervix is fully dilated and the patient has been pushing all throughout. Vertex is palpated in the occipito-anterior (OA) position and has descended to station 2 cm below the ischial spines in the previous hour. Which of the following most likely depicts the current condition of the patient?
Your Answer: Normal progress.
Explanation:The patient’s condition can be described as a normal progress of labour. The scenario shows a normal descent of the head in the pelvic cavity, with a favourable position, and occurring within an hour of the second stage of labour. A normal second stage of labour in a nulliparous individual occurs at a maximum of two hours, which is consistent with this patient. Hence, there is no delay in the second stage.
There is evident progress of labour in this patient, hence, obstructed labour or cephalopelvic disproportion is ruled out.
No signs of maternal distress such as tachycardia or pyrexia is described in this patient.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 31
Correct
-
A 35-year-old woman presented to the medical clinic for her first prenatal visit. Upon history-taking, it was noted that this was her first pregnancy and based on her last menstrual period, she is pregnant for 11 weeks already. There was also no mention of a history of medical problems. Upon further observation, the uterus was palpable midway between her pubic symphysis and the umbilicus. There was also no audible fetal heart tones using the Doppler stethoscope. Which of the following is considered the best management as the next step given the case above?
Your Answer: Schedule an ultrasound as soon as possible to determine the gestational age and viability of the foetus.
Explanation:In pregnancy, the uterus increases in size to accommodate the developing foetus. At 16 weeks gestation, the fundus of the uterus must be palpated at the midpoint between the umbilicus and the pubic symphysis but the patient’s uterus was already palpable at just 11 weeks.
If less than seven weeks pregnant, it’s unlikely to find a heartbeat by ultrasound. Using transvaginal ultrasound, a developing baby’s heartbeat should be clearly visible by the time a woman is seven weeks pregnant. Abdominal ultrasound is considerably less sensitive, so it can take longer for the heartbeat to become visible. If past seven weeks pregnant, seeing no heartbeat may be a sign of miscarriage.
Fetal viability is confirmed by the presence of an embryo that has cardiac activity. Cardiac activity is often present when the embryo itself measures 2 mm or greater during the 6th week of gestation. If cardiac activity is not evident, other sonographic features of early pregnancy can predict viability.
It is recommended that all pregnant women undergo a routine ultrasound at 10 to 13 weeks of gestation to determine an accurate gestational age. Getting an accurate gestational age is highly important and pertinent for the optimal assessment of fetal growth later in pregnancy. Ultrasound is the most reliable method for establishing a true gestational age by measurement of crown-rump length, which can be measured either transabdominally or transvaginally.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 32
Correct
-
A 34-year-old woman, known to have had a history of mild pulmonary hypertension, was admitted to the labour ward. She is at 36 weeks of pregnancy and is keen to have her baby delivered via caesarean section. Which of the following is the most appropriate advice to give to the patient given her situation?
Your Answer: Caesarean section
Explanation:Pulmonary hypertension (PH) is an increase of blood pressure in the pulmonary artery, pulmonary vein, or pulmonary capillaries, leading to shortness of breath, dizziness, fainting, and other symptoms, all of which are exacerbated by exertion. PH in pregnancy carries a 25–56% maternal mortality rate with a mixture of intrapartum and postpartum deaths.
Current recommendations for management of PH in pregnancy include termination of pregnancy if diagnosed early, or utilizing a controlled interventional approach with early nebulized prostanoid therapy and early elective caesarean section under regional anaesthesia. Other recommended therapies for peripartum management of PH include sildenafil and nitric oxide.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 33
Correct
-
A 44-year-old lady came to the clinic with a five-year history of urine incontinence. With a BMI of 34, she is fat. Her last child, weighing 4.2 kg, was born six years ago. She has been using various over-the-counter medicines to treat constipation and gastric reflux for the past three years. She is a non-smoker with normal blood pressure. Which of the following is not a risk factor for female urinary incontinence development?
Your Answer: Gastro-oesophageal reflux disease
Explanation:Stress UI (SUI) is more common among puerperal women, followed by mixed UI (MUI) and urge UI (UUI). Generally, episodes of urine leakage are infrequent and the amount of urine leakage is small.
Maternal age greater than 35 years, UI during pregnancy, elevated body mass index (BMI), multiparity, and normal birth are considered risk factors for postpartum UI. A 10-year cohort study developed with the goal of assessing the effect of the first normal birth on urinary symptoms showed that it was associated with an increase in SUI, in addition to UUI, regardless of maternal age or number of births.
Other factors such as: colour or race, episiotomy, perineal tears, newborn’s head circumference, newborn’s weight, gestational age at birth, smoking, and constipation require further studies in order to prove their association with postpartum UI.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 34
Correct
-
A baby with shoulder dystocia suffers a brachial plexus injury. You diagnose Erb-Duchenne palsy. Which nerve roots are typically affected?
Your Answer: C5 and C6
Explanation:Erb’s or Erb-Duchenne palsy is a type of brachial plexus injury. The brachial plexus comprises C5 to T1 nerve roots. In Erb’s palsy C5 and C6 are the roots primarily affected. Shoulder Dystocia is the most common cause of Erb’s palsy.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 35
Correct
-
Fetal blood is returned to the umbilical arteries & the placenta via the:
Your Answer: Hypogastric arteries
Explanation:In the foetus, the hypogastric artery ascends along the side of the bladder, and runs upward on the back of the anterior wall of the abdomen to the umbilicus, converging toward its fellow of the opposite side. Having passed through the umbilical opening, the two arteries, now termed umbilical, enter the umbilical cord, where they are coiled around the umbilical vein, and ultimately ramify in the placenta.
-
This question is part of the following fields:
- Physiology
-
-
Question 36
Correct
-
The transvaginal ultrasound of a 37 year old woman reveals a left ovarian mass. The mass is a unilocular cyst with diffuse homogenous ground glass echoes as a result of hemorrhagic debris. Which of the following is the most likely diagnosis?
Your Answer: Endometrioma
Explanation:An endometrioma, also known as a chocolate cyst is a benign ovarian cyst that occurs as a result of the trapping of endometriosis tissue inside the ovary. The findings on transvaginal ultrasound are often a unilocular cyst, with ground glass echogenicity due to haemorrhage. Other benign masses that can be evaluated using transvaginal ultrasound are functional cysts, serous and mucinous cystadenomas and mature teratomas.
-
This question is part of the following fields:
- Data Interpretation
-
-
Question 37
Correct
-
In a non-ovulating follicle, follicular growth is followed by:
Your Answer: Atresia
Explanation:During the ovulatory cycle, only one follicle will ovulate. The remaining non-ovulating follicles undergo disintegration. This process is known as atresia.
-
This question is part of the following fields:
- Embryology
-
-
Question 38
Correct
-
Regarding the renal tract during pregnancy, the following are true, EXCEPT:
Your Answer: The bladder tone increases
Explanation:Incontinence in women is typically related to dysfunction of the bladder or pelvic floor muscles, with such dysfunction often arising during pregnancy or childbirth, or at the time of menopause.
A pregnant woman may experience an increase in the size of the kidneys and ureter due to the increased blood volume and vasculature.
Later in pregnancy, the woman might develop physiological hydronephrosis and hydroureteronephrosis, which are normal.
There is an increase in glomerular filtration rate associated with an increase in creatinine clearance, protein, albumin excretion, and urinary glucose excretion.
There is also an increase in sodium retention from the renal tube so oedema and water retention is a common sign in pregnant women -
This question is part of the following fields:
- Physiology
-
-
Question 39
Correct
-
Bishop scoring is used for:
Your Answer: The success rate of induction of the labour
Explanation:The Bishop score is a system used by medical professionals to decide how likely it is that you will go into labour soon. They use it to determine whether they should recommend induction, and how likely it is that an induction will result in a vaginal birth.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 40
Correct
-
What is the maximum normal diameter of the yolk sac on transvaginal ultrasound?
Your Answer: 6mm
Explanation:The yolk sac increases in size up until the 10th week reaching a maximum diameter of 6mm in normal pregnancy. After the 10th week the yolk sac will gradually disappear. It is usually sonographically undetectable by 20 weeks. A yolk sac greater than 6mm diameter is suspicious of failed pregnancy.
-
This question is part of the following fields:
- Biophysics
-
-
Question 41
Incorrect
-
Regarding pelvic inflammatory disease, which of the following is the tubal factor infertility rate?
Your Answer: 25%
Correct Answer: 12.50%
Explanation:Pelvic inflammatory disease (PID) is a known risk factor in causing tubal infertility due to its role in tubal damage. The tubal infertility rate after one episode of PID is thought to be about 12.5%. After two episodes the risk increases to 25%, and 50% after three episodes. The usual causative agents are chlamydia and gonorrhoea.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 42
Incorrect
-
Which of the following Oestrogens (Oestrogens) becomes the predominant circulating oestrogen during pregnancy?
Your Answer: Oestradiol
Correct Answer: Estriol
Explanation:Oestradiol is the predominant form of oestrogen during the reproductive life of a female. The estrogenic potency of oestradiol is 12 times more than estrone and 80 times that of estriol.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 43
Correct
-
A 23-year-old woman at 36 weeks of gestation visits your clinic for follow up. On pelvic ultrasound you noted a decrease in amniotic fluid, and all her previous scans were normal. When asked she recollected on experiencing an episode of urinary incontinence yesterday, were she had wet her undergarment with a sudden gush of clear fluid. Considering the presentation, which of the following is MOST likely the cause of oligohydramnios in this patient?
Your Answer: Premature preterm rupture of membrane
Explanation:This patient presenting with oligohydramnios in her third trimester and had reported an episode of sudden gush of fluid secondary to ruptured membrane which she had mistaken to be “urinary incontinence”. Hence, the most likely cause of oligohydramnios in this patient will be premature preterm rupture of membrane (PPROM).
An amniotic fluid volume which is less than expected for gestational age is called as Oligohydramnios and is typically diagnosed by ultrasound examination. This condition can be qualitatively described as reduced amniotic fluid volume and quantitatively as amniotic fluid index ≤5 cm or a single deepest pocket <2 cm. Oligohydramnios either can be idiopathic or may have a maternal, fetal or placental cause. Fetal prognosis in this case depends on several factors like the underlying cause, the severity of loss ie. reduced versus no amniotic fluid state and the gestational age at which oligohydramnios occurred. As an adequate volume of amniotic fluid is critical for the normal fetal movements, for fetal lung development and for cushioning the fetus and umbilical cord from uterine compression, so pregnancies complicated with oligohydramnios are at higher risk for fetal deformation, pulmonary hypoplasia and umbilical cord compression.
Oligohydramnios is also associated with an increased risk for fetal or neonatal death, which can either be related to the underlying cause of reduction in amniotic fluid volume or due to the sequelae caused due to reduced amniotic fluid volume. The amniotic fluid volume reflects the balance between fluid production and movement of fluid out of the amniotic sac and the most common mechanisms behind oligohydramnios are fetal oliguria/anuria or fluid loss due to rupture of membranes; also reduction in the amount of lung fluid or increased swallowing do not play major roles in this. Idiopathic cases as in idiopathic oligohydramnios, may be due to alterations in the expression of water pores like aquaporin 1 and aquaporin 3, present in fetal membranes and placenta.Causes of oligohydramnios
a) Maternal causes includes:
– Medical or obstetric conditions associated with uteroplacental insufficiency like preeclampsia, chronic hypertension, collagen vascular disease, nephropathy, thrombophilia.
– Intake of medications like angiotensin converting enzyme inhibitors, prostaglandin synthetase inhibitors, trastuzumab.
b) Placental causes are:
– Abruption of placenta
– Twin polyhydramnios-oligohydramnios sequence which is the Twin to twin transfusion
– Placental thrombosis or infarction
c) Fetal cases leading to oligohydramnios are:
– Chromosomal abnormalities
– Congenital abnormalities which are associated with impaired urine production
– Growth restriction
– Demise
– Post-term pregnancy
– Ruptured fetal membranes
– Infections
– Idiopathic causesDuring First trimester: Etiology of oligohydramnios during the first trimester is often unclear. As the gestational sac fluid is primarily derived from the fetal surface of the placenta via transamniotic flow from the maternal compartment and secretions from the surface of the body of the embryo reduced amniotic fluid prior to 10 weeks of gestation is rare.
During Second trimester: Fetal urine begins to enter the amniotic sac and fetus begins to swallow amniotic fluid by the beginning of second trimester, therefore, during this period any disorders related to the renal/urinary system of the fetus begins to play a prominent role in the etiology of oligohydramnios. Some of such anomalies include intrinsic renal disorders like cystic renal disease and obstructive lesions of the lower urinary tract like posterior urethral valves or urethral atresia. Other common causes of oligohydramnios in the second trimester are maternal and placental factors and traumatic or nontraumatic rupture of the fetal membranes.
During Third trimester: Oligohydramnios which is first diagnosed in the third trimester is often associated with PPROM or with conditions such as preeclampsia or other maternal vascular diseases leading to uteroplacental insufficiency. Oligohydramnios frequently accompanies fetal growth restriction as a result of uteroplacental insufficiency.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 44
Correct
-
Which of the following has been shown to improve pruritus and liver function in patients with obstetric cholestasis?
Your Answer: Ursodeoxycholic acid
Explanation:Intrahepatic cholestasis characterized by reversible cholestasis typically occurring in the second or third trimester of pregnancy, elevated serum aminotransferases and bile acid level and resolution of symptoms by 2 to 3 weeks after delivery. Ursodeoxycholic acid has shown to reduce the symptoms of this condition.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 45
Correct
-
A 26-year-old pregnant woman in her third trimester, was admitted with headache, abdominal pain and visual disturbances. Shortly after, she had a fit. What is the most appropriate management?
Your Answer: 4g MgSO4 in 100ml 0.9% Normal saline in 5 min.
Explanation:The woman is most probably suffering from eclampsia.
Magnesium sulphate (MgSO4) is the agent most commonly used for treatment of eclampsia and prophylaxis of eclampsia in patients with severe pre-eclampsia. It is usually given by either intramuscular or intravenous routes. The intramuscular regimen is most commonly a 4 g intravenous loading dose, immediately followed by 10 g intramuscularly and then by 5 g intramuscularly every 4 hours. The intravenous regimen is given as a 4 g dose, followed by a maintenance infusion of 1 to 2 g/h by controlled infusion pump. -
This question is part of the following fields:
- Obstetrics
-
-
Question 46
Correct
-
From which of the following spinal segments do both the internal and external anal sphincters receive their innervation?
Your Answer: S4
Explanation:The anal sphincters are responsible for closing the anal canal to the passage of faeces and flatus. The smooth muscle of the involuntary internal sphincter sustains contraction to prevent the leakage of faeces between bowel movements and is innervated by the pelvic splanchnic nerves, which are a branch of the spinal segment 4. The external sphincter is made up of skeletal muscle and can therefore contract and relax voluntarily. Its innervation comes from the inferior rectal branch of the pudendal nerve, and the perineal branch of S4 nerve roots.
-
This question is part of the following fields:
- Anatomy
-
-
Question 47
Incorrect
-
Prenatal screening is recommended if ultrasound scan at 16 weeks confirms that the foetus is male and the mother has had an affected son previously. Choose the single most likely condition from the following list of options. 7
Your Answer: Spinal muscular atrophy
Correct Answer: Duchene muscular dystrophy
Explanation:The condition should be an X-linked recessive condition, as it affects only male offspring. Duchene muscular dystrophy is an X-linked recessive condition. Cystic fibrosis is an autosomal recessive disorder. Spina bifida is a multifactorial condition. Down syndrome is caused by trisomy of chromosome 21. Spinal muscular atrophies are inherited in an autosomal-recessive pattern.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 48
Incorrect
-
The chance of multiple pregnancy increases:
Your Answer: With bromocriptine use for infertility treatment
Correct Answer: With advancing maternal age
Explanation:Dizygotic twin pregnancies are known to increase with age of the mother. Naturally conceived twins are thought to occur in a 0.3% rate in women under 25 years, 1.4% between 25 and 34, 3% between 34 and 39, and 4.1% in women in their 40s or over. We also know that at least 50% of all twin pregnancies are conceived through ART and that this proportion is probably higher for women in their 40s.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 49
Incorrect
-
Which of the following microorganisms is considered the most frequently associated with septic shock in obstetrics and gynecology?
Your Answer: Staphylococcus aureus
Correct Answer: Escherichia coli
Explanation:Organisms frequently associated with obstetric sepsis include: beta haemolytic streptococci, Gram-negative rods such as Escherichia coli, Streptococcus pneumoniae and influenza A and B.
E. coli is the most common sepsis pathogen in pregnancy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 50
Correct
-
A 77 year old woman undergoes staging investigations for endometrial carcinoma. This shows invasion of the inguinal lymph nodes. What is this patients 5-year survival?
Your Answer: 15%
Explanation:Lymph node involvement means that the carcinoma is stage 4. The 5 year survival of stage 4 endometrial carcinoma is 16%.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 51
Correct
-
Regarding the rectus sheath which of the following statements are true?
Your Answer: Above the arcuate line the internal oblique divides into two lamellae
Explanation:The rectus sheath is formed by the aponeurosis of the internal and external oblique muscles and the transversus abdominus muscle. The internal oblique divides into two lamellae and encloses the rectus muscle. Anteriorly it fuses with the aponeurosis of the external oblique and posteriorly with that of the transverus abdominus. Below the arcuate line the aponeurosis of all the flat muscles lies anteriorly and posteriorly it is only enclosed by the transveralis fascia.
-
This question is part of the following fields:
- Anatomy
-
-
Question 52
Correct
-
Question 53
Incorrect
-
All of the following features are associated with congenital uterine malformations except:
Your Answer: Spontaneous abortions
Correct Answer: Pregnancy induced hypertension
Explanation:Congenital uterine abnormalities are associated with an increased risk of spontaneous abortions, preterm delivery of the foetus, fetal growth retardation and malpresentation.
-
This question is part of the following fields:
- Embryology
-
-
Question 54
Correct
-
Which of the following factors causes the greatest increase in risk of developing bladder cancer?
Your Answer: Smoking
Explanation:Transitional cell carcinoma of the bladder is most commonly caused by cigarette smoke. Other risk factors include naphthylamine, azodyes and long term cyclophosphamide use.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 55
Incorrect
-
Question 56
Incorrect
-
Which of the following drugs is associated with reduced milk production whilst breastfeeding?
Your Answer: Fluoxetine
Correct Answer: Cabergoline
Explanation:Domperidone and metoclopramide are D2 dopamine receptor antagonists. They are primarily used to promote gastric motility. They are also known as galactagogues and they promote the production of milk. Cabergoline and bromocriptine are prolactin inhibitors and they reduce milk production.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 57
Correct
-
A young woman came to your clinic seeking help. She has been married for two years and has yet to conceive. The following are the findings of blood tests: Luteinizing hormone levels are low. Low levels of follicle stimulating hormone. Thyroid stimulating hormone (TSH) levels are low. Prolactin-high. What is the most effective way to deal with infertility?
Your Answer: Bromocriptine
Explanation:The most common treatment approach is with the dopamine receptor agonists, bromocriptine, and cabergoline. Bromocriptine normalizes prolactin and decreases tumour size in 80%–90% of patients with microadenomas. Bromocriptine should be given to this patient who has developed hyperprolactinemia anovulation.
Women with hyperprolactinaemic anovulation are treated with dopamine agonists such as bromocriptine.
This patient has also developed symptoms of a low-functioning pituitary gland tumour, which bromocriptine will assist to shrink. Before starting bromocriptine, a head MRI scan should be considered to confirm the suspected diagnosis.Clomiphene is an oestrogen receptor modulator that is selective. It works by competing with oestrogen receptors in the hypothalamus. This disrupts normal negative feedback mechanisms, causing the release of pituitary gonadotropins, particularly LH, to rise, triggering ovulation.
When the levels of gonadotropins and oestrogen are normal but the women still have ovulatory dysfunction, it is successful in inducing ovulation. In hypogonadotropic hypogonadism and hypogonadotropic hypogonadism patients, clomiphene is frequently ineffective. -
This question is part of the following fields:
- Gynaecology
-
-
Question 58
Correct
-
A 35-year-old female patient, gravida 1 para 1, visits the clinic to have her contraception method evaluated. The patient has had unpredictable bleeding for the past 8 months since receiving a subdermal progestin implant and begs that it be removed. She used to use combined oral contraceptives and would like to go back to it. The patient has primary hypertension, which she was diagnosed with last year and is effectively controlled on hydrochlorothiazide. She does not take any other medications or have any allergies. Her father and brother both suffer from type 2 diabetes. The patient does not smoke, drink, or use illegal drugs. Her BMI is 24 kg/m2. Blood pressure is 130/75. Physical examinations are all normal. Which of the following is increased by using combination oral contraceptives?
Your Answer: Worsening hypertension
Explanation:Overt hypertension, developing in about 5% of Pill users, and increases in blood pressure (but within normal limits) in many more is believed to be the result of changes in the renin-angiotensin-aldosterone system, particularly a consistent and marked increase in the plasma renin substrate concentrations. The mechanisms for the hypertensive response are unclear since normal women may demonstrate marked changes in the renin system. A failure of the kidneys to fully suppress renal renin secretion could thus be an important predisposing factor. These observations provide guidelines for the prescription of oral contraceptives. A baseline blood pressure measurement should be obtained, and blood pressure and weight should be followed at 2- or 3-month intervals during treatment. Oral contraceptive therapy should be contraindicated for individuals with a history of hypertension, renal disease, toxaemia, or fluid retention. A positive family history of hypertension, women for whom long-term therapy is indicated, and groups such as blacks, especially prone to hypertensive phenomena, are all relative contraindications for the Pill.
COCs do not increase the risk of developing breast and endometrial cancer, Type 2 DM or breast fibroadenoma.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 59
Correct
-
Regarding twin pregnancies all of the following are correct EXCEPT:
Your Answer: Identical or monozygotic twins arise from fertilization of two ovum
Explanation:Monozygotic (MZ) twins originate when a single egg is fertilized to form one zygote, which then divides into two embryos. Although they share the same genotype they are not phenotypically identical.
-
This question is part of the following fields:
- Genetics
-
-
Question 60
Incorrect
-
Which of the following causes an increase in Sex Hormone Binding Globulin (SHBG)?
Your Answer: PCOS
Correct Answer: Liver cirrhosis
Explanation:Liver cirrhosis is known to lead to decreased levels of SHBG. Other causes of high SHBG are:
Oestrogens e.g. oral contraceptives
Pregnancy
Hyperthyroidism
Liver cirrhosis
Anorexia nervosa
Drugs e.g. anticonvulsants -
This question is part of the following fields:
- Endocrinology
-
-
Question 61
Incorrect
-
Intrapartum antibiotics prophylaxis is required in which of the following conditions?
Your Answer: Emergency Caesarean Section
Correct Answer: A previous infant with Group B streptococcus disease regardless of present culture
Explanation:Group B Streptococcus (GBS) or Streptococcus agalactiae is a Gram-positive bacteria which colonizes the gastrointestinal and genitourinary tract. In the United States of America, GBS is known to be the most common infectious cause of morbidity and mortality in neonates. GBS is known to cause both early onset and late onset infections in neonates, but current interventions are only effective in the prevention of early-onset disease.
The main risk factor for early-onset GBS infection is colonization of the maternal genital tract with Group B Streptococcus during labour. GBS is a normal flora of the gastrointestinal (GI) tract, which is thought to be the main source for maternal colonization.
The principal route of neonatal early onset GBS infection is vertical transmission from colonized mothers during passage through the vagina during labour and delivery.
Intravenous penicillin G is the treatment of choice for intrapartum antibiotic prophylaxis against Group B Streptococcus.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 62
Correct
-
Question 63
Correct
-
The arcuate line forms part of the border of the pelvic brim. Where is it located?
Your Answer: Ilium
Explanation:Arcuate means ‘bow shaped’ and there are different arcuate lines in anatomical terms. Regarding the pelvic brim this is composed of the arcuate line of the ilium, pectineal line and prominences of sacrum and pubic symphysis (as demonstrated in the images below). As can be seen the arcuate line is a smooth rounded border on the internal surface of the ilium inferior to the iliac fossa and Iliacus. Image sourced from Wikipedia Note: The pelvic outlet is also called the inferior aperture. The pelvic brim is the superior aperture
-
This question is part of the following fields:
- Anatomy
-
-
Question 64
Correct
-
A 28-year-old white female consults you with a complaint of irregular heavy menstrual periods. Her general physical examination, pelvic examination, and HPV test are normal and she has a negative pregnancy test. A CBC and chemistry profile are also normal. The next step in her workup should be:
Your Answer: Cyclic administration of progesterone for 3 months
Explanation:Abnormal uterine bleeding is a relatively common disorder which may be due to functional disorders of the hypothalamus, pituitary, or ovary, as well as uterine lesions. However, the patient who is younger than 30 years of age will rarely be found to have a structural uterine defect. Once pregnancy, hematologic disease, and renal impairment are excluded, administration of intramuscular or oral progesterone will usually produce definitive flow and control the bleeding. No further evaluation should be necessary unless the bleeding recurs.
Endometrial aspiration, dilatation and curettage, and other diagnostic procedures are appropriate for recurrent problem or for older women. Oestrogen would only increase the problem, which is usually due to anovulation with prolonged oestrogen secretion, producing a hypertrophic endometrium.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 65
Correct
-
Among the following which will not be elevated in the third trimester of pregnancy?
Your Answer: Serum free T4
Explanation:Normally, there will be a slight raise in prolactin level throughout pregnancy even despite estrogen stimulating and progesterone inhibiting prolactin secretion.
Serum alkaline phosphatase levels will be increased in pregnancy due to placental ALP.
During the first trimester of pregnancy there is a physiological mechanism by hCG causing cross-stimulation of the TSH receptors and as a result of this the concentration of thyroid stimulating hormone (TSH) normally decreases. During second trimester TSH concentration will again return back to its pre-pregnancy levels and then rises slightly by the third trimester. However, most of the changes still occur within the normal non-pregnant range, and the serum free T3 and T4 concentrations remain unchanged throughout pregnancy. But the total concentrations, which include both free and protein-bound fractions, elevates significantly due to an increase in the circulating binding globulins.
Iron binding capacity reflects transferrin, a protein used for iron transportation, which is a globulin found in the beta band on electrophoresis. To counteract the reduction of plasma iron during pregnancy both transferrin and iron binding capacity are elevated during this period.
When compared to the non-pregnant level, cortisol levels are been elevated up to three times than normal.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 66
Incorrect
-
Which of the following fasting plasma glucose (FPG) values for OGTT (Oral glucose tolerance test) is diagnostic of gestational diabetes according to the WHO criteria?
Your Answer: FPG 7.1mmol/L; 2 hour 11.1mmol/L
Correct Answer: FPG 6.1mmol/L; 2 hour 7.8mmol/L
Explanation:There are several criteria that aid in the diagnosis of gestational diabetes in pregnancy including NICE, WHO and modified WHO:
GDM Diagnostic Criteria:
NICE: Immediate FBG >5.6, 2 hour glucose >7.8
WHO: Immediate FBG >6.1, 2 hour glucose >7.8
Modified WHO: Immediate FBG >7.1, 2 hour glucose >7.8Random glucose and OGTT 2 hour readings of >11.1 are diagnostic of diabetes in non-pregnant states but are not part of the gestational diabetes criteria.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 67
Correct
-
During normal pregnancy, a weight gain is anticipated. The average weight gain is approximately:
Your Answer: 10-15 kg
Explanation:Institute of Medicine Weight Gain Recommendations for Pregnancy: Recommends a gestational weight gain of 16.8–24.5 kg (37–54 lb) for women of normal weight, 14.1–22.7 kg (31–50 lb) for overweight women, and 11.3–19.1 kg (25–42 lb) for obese women.
-
This question is part of the following fields:
- Physiology
-
-
Question 68
Correct
-
A pregnant patient with a chest infection is worried about the radiation risk of a chest X Ray. How many days of natural background radiation is equivalent to a chest X Ray?
Your Answer: 2.5
Explanation:X-rays carry low levels of risk during pregnancy and are not a significant cause for concern if the total exposure to ionising radiation is less than 5 rads throughout the pregnancy; a chest X-ray is about 0.00007 rads. The amount of radiation generated from a chest X-ray is equivalent to 2.4 days of natural background radiation. Non-urgent radiological tests should, however, be avoided between 10-17 weeks gestation as there is a higher risk of central nervous system teratogenesis during this time.
-
This question is part of the following fields:
- Biophysics
-
-
Question 69
Incorrect
-
You are called to assist in an initially midwife led delivery. Upon delivering a female baby you notice the baby has partial fusion of the labioscrotal folds. You suspect congenital adrenal hyperplasia. Which of the following genes is most likely to be mutated?
Your Answer: BRCA1
Correct Answer: CYP21A
Explanation:CAH leads to virilization of the female foetus. It occurs to an enzyme deficiency (21-hydroxylase). This results in a reduced levels of corticosteroids from being circulated resulting in hyperplasia of the adrenal glands and increased progesterone production. The CYP21A gene has been implicated in causes this deficiency.
-
This question is part of the following fields:
- Genetics
-
-
Question 70
Correct
-
Which of the following tests is used to detect antibodies or complement bound to red blood cell antigens in vivo?
Your Answer: Direct Coombs
Explanation:When the red cells are coated with immune IgG antibody, the cells do not agglutinate but when anti-IgG antiserum is added to these sensitized cells visible agglutination occurs. This is known as a positive direct coombs test.
-
This question is part of the following fields:
- Physiology
-
-
Question 71
Correct
-
Endometrial tissue found within the myometrium is classed as
Your Answer: Adenomyosis
Explanation:Endometrial tissue found within the myometrium is Adenomyosis. If endometrial tissue is found at a distant site to the uterus it is termed endometriosis. Fibroids are smooth muscle tumours (Leiomyoma’s) sometimes called myoma’s.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 72
Correct
-
A 34-year-old woman, gravida 1 para 1, presented to the emergency department complaining of left breast pain six weeks after a spontaneous, uncomplicated term vaginal delivery. She reported having noticed the pain and redness on her left breast a week ago. From her unaffected breast, she continued to breastfeed her infant. Upon history taking, it was noted that she has no chronic medical conditions and for medication, she only takes a daily multivitamin. Her temperature was taken and the result was 38.3 deg C (101 deg F). Further observation was done and the presence of an erythematous area surrounding a well-circumscribed, 4-cm area of fluctuance extending from the areola to the lateral edge of the left breast was noted. There was also the presence of axillary lymphadenopathy. Which of the following is the next step to best manage the condition of the patient?
Your Answer: Needle aspiration and antibiotics
Explanation:Breast infections can be associated with superficial skin or an underlying lesion. Breast abscesses are more common in lactating women but do occur in nonlactating women as well.
The breast contains breast lobules, each of which drains to a lactiferous duct, which in turn empties to the surface of the nipple. There are lactiferous sinuses which are reservoirs for milk during lactation. The lactiferous ducts undergo epidermalization where keratin production may cause the duct to become obstructed, and in turn, can result in abscess formation. Abscesses associated with lactation usually begin with abrasion or tissue at the nipple, providing an entry point for bacteria. The infection often presents in the second postpartum week and is often precipitated in the presence of milk stasis. The most common organism known to cause a breast abscess is S. aureus, but in some cases, Streptococci, and Staphylococcus epidermidis may also be involved.
The patient will usually provide a history of breast pain, erythema, warmth, and possibly oedema. Patients may provide lactation history. It is important to ask about any history of prior breast infections and the previous treatment. Patients may also complain of fever, nausea, vomiting, purulent drainage from the nipple, or the site of erythema. It is also important to ask about the patient’s medical history, including diabetes. The majority of postpartum mastitis are seen within 6 weeks of while breast-feeding
The patient will have erythema, induration, warmth, and tenderness to palpation at the site in question on the exam. It may feel like there is a palpable mass or area of fluctuance. There may be purulent discharge at the nipple or site of fluctuance. The patient may also have reactive axillary adenopathy. The patient may have a fever or tachycardia on the exam, although these are less common.
Incision and drainage are the standard of care for breast abscesses. If the patient is seen in a primary care setting by a provider that is not comfortable in performing these procedures, the patient may be started on antibiotics and referred to a general surgeon for definitive treatment. Needle aspiration may be attempted for abscesses smaller than 3 cm or in lactational abscesses. A course of antibiotics may be given before or following drainage of breast abscesses.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 73
Correct
-
Which is not part of post natal urinary incontinence management?
Your Answer: Good control of blood pressure
Explanation:Thee good news in regard to incontinence after childbirth is that there are many treatment options. Some common treatment options are listed below.
Food and drinks such as coffee, citrus, spicy foods and soda can all irritate the bladder. Cutting back on or eliminating these foods may help improve incontinence symptoms. Keeping weight within a healthy BMI range, and/or focusing on losing pregnancy weight, can also help with bladder control.
Kegels strengthen the pelvic floor, giving more control over urinary urges. Pelvic floor physical therapy can also help build muscle memory and strength. The abdominal muscles, hip muscles and pelvic floor muscles work together when a woman performs strengthening exercises like Kegels. Physical therapists identify areas of weakness in those muscle groups to help a woman build a strong core and pelvic floor.
The bladder is a muscle that should be regularly strengthened. Scheduling urination times and then gradually increasing the amount of time in between urination can increase bladder strength.
Percutaneous tibial nerve stimulation is a nonsurgical treatment for overactive bladder and a form of neuromodulation therapy. During PTNS treatments, a doctor places a slim needle in the ankle where the tibial nerve is located. The needle delivers electrical impulses to the tibial nerve, which sends signals to the sacral nerves in the spine that control bladder and pelvic floor function. Over time, these pulses block nerve signals that are not working properly to lessen urinary incontinence symptoms.
Evaluating lifestyle factors. Excessive coughing due to smoking or being overweight can put unnecessary strain on the pelvic floor muscles. Certain drugs such as antidepressants and antihistamines can also have an impact on urinary incontinence.
Pessary. A pessary is a device inserted into the vagina to provide support for vaginal tissues, in turn, aiding in bladder incontinence.Surgical treatment options can help support the pelvic floor and may be recommended for women who have completed childbearing and have not had success with conservative therapy.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 74
Correct
-
Regarding congenital CMV infection, what percentage of infants are symptomatic?
Your Answer: 10-15%
Explanation:Congenital cytomegalovirus infections are the most common cause of sensorineural hearing loss in babies. Cytomegalovirus infection during the perinatal period can be transferred to the foetus especially if the primary infection is during pregnancy. In babies born with congenital CMV about 10-15% are symptomatic, while 10-15% of those who are asymptomatic will develop symptoms in life. Some of the features of CMV infection include sensorineural hearing loss, visual impairment, cerebral palsy, microcephaly and seizures. Other causes of infective congenital sensorineural hearing loss include: Rubella, HIV, Herpes Simplex Virus, Measles, Varicella Zoster virus, Mumps and West Nile Virus.
-
This question is part of the following fields:
- Microbiology
-
-
Question 75
Correct
-
Regarding anti-epileptic use in the 1st trimester of pregnancy, which of the following is closely associated with the development of congenital malformations?
Your Answer: Sodium valproate
Explanation:Sodium Valproate is known to be the most teratogenic when used in the first trimester of pregnancy. This antiepileptic increases the risk of congenital malformations including a 10-20 fold risk of neurodevelopmental defects. Though the use of antiepileptics should generally be avoided during pregnancy, carbamazepine, or newer drugs such as Lamotrigine are thought to carry less of a risk of teratogenicity.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 76
Correct
-
A 61-year-old woman presents to OBGYN clinic with a complaint of irregular bleeding per vagina for the last 3 months. Her past medical history is not significant and she went through menopause around a decade ago. A cervical screening test is performed and comes back normal. PCR for chlamydia is also negative. Endometrial thickness of around 8mm is seen on transvaginal ultrasound. What would be the next step of management?
Your Answer: Referral to the gynaecologist for endometrial biopsy
Explanation:This patient had postmenopausal vaginal haemorrhage and an 8mm endometrial thickness. Endometrial thickness of 4mm or more in a postmenopausal woman with vaginal bleeding necessitates an endometrial biopsy to rule out endometrial cancer, and this patient should be referred to a gynaecologist for this procedure.
All of the other choices are incorrect. -
This question is part of the following fields:
- Gynaecology
-
-
Question 77
Correct
-
A 22-year-old female is at her second trimester of pregnancy and she presented to the medical clinic to receive human papillomavirus vaccination. Which of the following is considered the best step to do?
Your Answer: Postpone vaccination until after delivery
Explanation:Genital HPV is a common virus that is passed from one person to another through direct skin-to-skin contact during sexual activity. Most HPV types cause no symptoms and go away on their own, but some types can cause cervical cancer in women and other less common cancers — like cancers of the anus, penis, vagina, and vulva and oropharynx. Other types of HPV can cause warts in the genital areas of men and women, called genital warts.
HPV vaccination is recommended for 11 and 12 year-old girls. It is also recommended for girls and women age 13 through 26 years of age who have not yet been vaccinated or completed the vaccine series; HPV vaccine can also be given to girls beginning at age 9 years. CDC recommends 11 to 12 year olds get two doses of HPV vaccine to protect against cancers caused by HPV.
The vaccine is not recommended for pregnant women. Studies show that the HPV vaccine does not cause problems for babies born to women who were vaccinated while pregnant, but more research is still needed. A pregnant woman should not get any doses of the HPV vaccine until her pregnancy is completed.
Getting the HPV vaccine when pregnant is not a reason to consider ending a pregnancy. If a woman realizes that she got one or more shots of an HPV vaccine while pregnant, she should wait until after her pregnancy to finish any remaining HPV vaccine doses.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 78
Correct
-
Placental production of hPL, hCG, Oestrogen and Progesterone are examples of which type of mechanism
Your Answer: Endocrine
Explanation:Hormones that are secreted into the circulation at one site but have effects on distal target organs are endocrine as is the case with the hormones above. Autocrine and Intracrine messengers act within the same cell. Exocrine glands secrete their products into ducts. Apocrine is a histological term used to describe some types of exocrine gland.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 79
Correct
-
A 23-year-old woman, G1PO comes to your clinic at 12 week of pregnancy. She is complaining of mild vaginal bleeding for the past 12 hours, along with bouts of mild cramping lower abdominal pain. On vaginal examination, the cervical os is closed with mild discharge containing blood clots and an ultrasonography confirms the presence of a live fetus with normal heart rate. Which among of the following is the most likely diagnosis?
Your Answer: Threatened abortion
Explanation:Uterine bleeding in the presence of a closed cervix along with sonographic visualization of an intrauterine pregnancy with detectable fetal cardiac activity are diagnostic of threatened abortion.
Abortion does not always follow a uterine bleeding in early pregnancy, sometimes not even after repeated episodes or large amounts of bleeding, that is why the term “threatened” is used in this case. In about 90 to 96% cases, the pregnancy continues after vaginal bleeding if occured in the presence of a closed os and a detectable fetal heart rate. Also as the gestational age advances its less likely the condition will end in miscarriage.
In cases of inevitable abortion, there will be dilatation of cervix along with progressive uterine bleeding and painful uterine contractions. The gestational tissue can be either felt or seen through the cervical os and the passage of this tissue occurs within a short time.
In case were the membranes have ruptured, partly expelling the products of conception with a significant amounts of placental tissue left in the uterus is called as incomplete abortion. During the late first and early second trimesters this will be the most common presentation of an abortion. Examination findings of this includes an open cervical os with gestational tissues observed in the cervix and a uterine size smaller than expected for gestational age and a partially contracted uterus. The amount of bleeding will vary but can be severe enough to cause hypovolemic shock, with painful contractions and an ultrasound revealing tissues in the uterus.
An in utero death of the embryo or fetus prior to 20 weeks of gestation is called as a missed abortion. In this case the women may notice that the symptoms associated with early pregnancy like nausea, breast tenderness, etc have disappeared and they don’t ‘feel pregnant’ anymore. Vaginal bleeding may occur but the cervix remains closed and the ultrasound done reveals an intrauterine gestational sac with or without an embryonic/fetal pole, but no embryonic/fetal cardiac activity will be noticed.
In case of complete abortion, miscarriage occurs before the 12th week and the entire contents of conception will be expelled out of uterus. If this case, the physical examination will show a small and well contracted uterus with an open or closed cervix. There is scant vaginal bleeding with only mild cramping and ultrasound will reveal an empty uterus without any extra-uterine pregnancy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 80
Correct
-
Which of the following nerves passes through the inguinal canal?
Your Answer: Ilioinguinal nerve
Explanation:The contents of the inguinal canal is the ilioinguinal nerves, the round ligament of uterus in the females and the spermatic cord with its contents in males.
-
This question is part of the following fields:
- Anatomy
-
-
Question 81
Correct
-
A 55 year old patient with a who has tried unsuccessful conservative measures for her overactive bladder, would like to consider Oxybutynin. She wants to know how common dry mouth is as a side effect, as her sister suffered from it on while on the same drug.
Your Answer: approximately 1 in 10 patients
Explanation:Urinary incontinence can be divided into two main aetiologies, stress incontinence, or overactive bladder. Conservative management include lifestyle interventions, controlling fluid intake, or bladder exercises. If conservative management is no longer efficient, then medications may be indicated. Oxybutynin is an anticholinergic drug used in the treatment of urinary incontinence. As with other anticholinergic drugs, side effects include dry mouth, dry eyes, blurry vision and constipation. About 1 in 10 patients taking Oxybutynin will experience some of these side effects.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 82
Incorrect
-
Which of the following drugs is most associated with coronary artery spasm?
Your Answer: Verapamil
Correct Answer: Ergometrine
Explanation:Ergot alkaloids e.g. Ergometrine, produce marked and prolonged alpha receptor mediated vasoconstriction. Its overdose can cause ischemia and gangrene of the limbs and bowel. It also causes coronary artery spasm and has been used by cardiologist as a provocation test.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 83
Incorrect
-
What is the target INR in a patient who has just been started on warfarin therapy due to a pulmonary embolism?
Your Answer: 3.0-4.0
Correct Answer: 2.0-3.0
Explanation:Warfarin can be useful for management of thromboembolism. The target INR range for this medication is between 2.0-3.0 in patients with venous thromboembolism, pulmonary embolism etc. The INR range may increase to 3.0-4.0 in patients with mechanical valves. However, warfarin is not recommended in pregnancy, and Low Molecular Weight Heparin should be used for thromboprophylaxis instead.
-
This question is part of the following fields:
- Pharmacology
-
-
Question 84
Correct
-
A 24 year old patient presents as 24 weeks pregnant with vaginal discharge. Swabs show Chlamydia Trachomatis detected. Which of the following is the most appropriate treatment regime?
Your Answer: Erythromycin 500 mg twice a day for 14 days
Explanation:The treatment of Chlamydia includes avoidance of intercourse, use of condoms and antibiotic treatment. Erythromycin 500mg orally QID for 7 days or Amoxicillin 500mg TDS for 7 days or Ofloxacin 200mg orally BD for 7 days.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 85
Incorrect
-
Among the below mentioned conditions which is not a contraindication to tocolysis?
Your Answer: Suspected fetal compromise determined by cardiotocography
Correct Answer: Maternal hypothyroidism
Explanation:Contraindications to tocolysis in preterm labor are as follows:
– Gestational age > 34 weeks or <24 weeks
– Labor is too advanced with an advanced cervical dilation of >4 cm
– Abnormal CTG suggesting a non-reassuring fetal status
– Lethal fetal anomalies
– Intrauterine fetal demise
– Suspected fetal compromise
– Significant antepartum hemorrhage, such as placental abruption/ active vaginal bleeding with hemodynamic instability
– Any suspected intrauterine infections like chorioamnionitis
– Maternal hypotension
– Pregnancy-induced hypertension/ eclampsia/ pre-eclampsia
– Placenta previa
– Placental insufficiency
– Intrauterine growth retardation
– Maternal allergy to specific tocolytic agents or cases where tocolytics are contraindicated due to specific comorbidities like in case of cardiac disease, were beta agonists cannot be administered.As there are nonpulmonary morbidities associated with preterm birth, fetal pulmonary maturity, known or suspected, is not an absolute contraindication for tocolysis. These fetuses could potentially benefit from prolongation of pregnancy and from the nonpulmonary benefits of glucocorticoid therapy.
When cervical dilation is greater than 3 cm inhibition of preterm labor is less likely to be successful. In such cases Tocolysis can be considered when the goal is to administer antenatal corticosteroids or to safely transport the mother to a tertiary care center.
Maternal hypothyroidism which is usually treated with thyroxine is not a contraindication to suppression of labor.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 86
Correct
-
Turner's syndrome is characterised by :
Your Answer: Streak ovaries
Explanation:Turner syndrome, a condition that affects only females, results when one of the X chromosomes (sex chromosomes) is missing or partially missing. Turner syndrome can cause a variety of medical and developmental problems, including short height, failure of the ovaries to develop and heart defects. Streak ovaries are a form of ovarian dysgenesis and are associated with Turner syndrome. Occasionally they may be functional and secondary sexual characteristics may develop.
-
This question is part of the following fields:
- Embryology
-
-
Question 87
Correct
-
A 52-year-old lady comes to your office with vaginal bleeding 7 hours after sexual intercourse. She hasn't had a menstrual period in over a year. A year ago, she had a normal pap smear. She has no other symptoms and appears to be in good condition. Which of the following is the most likely underlying cause of this woman's postcoital bleeding?
Your Answer: Vaginal atrophy
Explanation:Vaginal atrophy (thinning of vaginal tissue): Oestrogen helps to keep this tissue healthy. After menopause, low oestrogen levels can cause your vaginal walls to become thin, dry, and inflamed. That often leads to bleeding after sex.
Vaginal atrophy is the most common cause of post menopausal vaginal bleeding.
With a normal pap smear a year ago, this patient is unlikely to develop cervical cancer.
Cervical ectropions are not common in post-menopausal women.
Endometrial cancer and cervical polyps are possible causes of postcoital bleeding, however, they are not as common as vaginal atrophy.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 88
Correct
-
Which of the following increases during pregnancy?
Your Answer: Tidal Volume
Explanation:Ventilation begins to increase significantly at around 8 weeks of gestation, most likely in response to progesterone-related sensitization of the respiratory centre to carbon dioxide and the increased metabolic rate. Significant alterations occur in the mechanical aspects of ventilation during pregnancy. Minute ventilation (or the amount of air moved in and out of the lungs in 1 minute) is the product of tidal volume and respiratory rate and increases by approximately 30–50 per cent with pregnancy. The increase is primarily a result of tidal volume, which increases by 40 per cent (from 500 to 700 mL), because the respiratory rate remains unchanged. The increase in minute ventilation is perceived by the pregnant woman as shortness of breath, which affects 60–70 per cent of women. This physiological dyspnoea is usually mild and affects 50 per cent of women before 20 weeks gestation, but resolves immediately postpartum.
-
This question is part of the following fields:
- Physiology
-
-
Question 89
Correct
-
Which HPV subtypes are chiefly associated with causing cancer?
Your Answer: 16 and 18
Explanation:HPV 16 and 18 are responsible for 70% of cases of HPV related cancers. They are considered the most important high risk genotypes of HPV. As well as cervical cancer they are associated with cancers of the oropharynx and anogenital region.
There are over 100 genotypes of HPV including several other high risk HPV types. Gardasil® is a quadrivalent vaccine against HPV Types 6, 11, 16, and 18
HPV genotypes 6 and 11 are low risk and cause anogenital warts.
Typically 70% of HPV infections are cleared within 1 year and 90% are cleared within 2 years
-
This question is part of the following fields:
- Microbiology
-
-
Question 90
Correct
-
A 24 year old woman presents to the clinic with foul smelling vaginal discharge. Which facultative anaerobic bacteria is most likely to be the cause?
Your Answer: Gardnerella vaginalis
Explanation:Bacterial vaginosis is a common infection of the vagina caused by the overgrowth of atypical bacteria, most commonly Gardnerella vaginalis, a gram indeterminate bacteria, which is also a facultative anaerobe. Patients often complain of foul-smelling fishy discharge and dysuria. In diagnosing BV, a swab is taken for microscopy, often revealing clue cells. Of the other organisms listed in the options, Neisseria is an obligate anaerobe, while Chlamydia trachomatis is an obligate intracellular aerobe. Treponema Pallidum is an aerophilic bacteria and Mycoplasma hominis is a pleomorphic parasitic bacterium.
-
This question is part of the following fields:
- Microbiology
-
-
Question 91
Correct
-
A 29-year-old woman presents to the emergency department of your hospital complaining of fever, she had given birth to a healthy male baby four days ago. During vaginal delivery, she sustained small vaginal laceration, suture repair was not done as the lesion were small. Presently she is breastfeeding her baby. Physical examination shows no uterine tenderness and the rest of the examinations were unremarkable. Which of the following can be the most likely cause of this Patient's fever?
Your Answer: Infection of the unrepaired vaginal laceration
Explanation:As the time of onset of fever is the 4th day of postpartum and absence of uterine tenderness on exam makes infection of vaginal laceration the most likely cause of this presentation.
Exquisite uterine tenderness will be experienced in case of endometritis and symptoms are expected to start much earlier like by 2-3 days of postpartum.
UTI is often expected on days one or two of postpartum, also there are no urinary symptoms suggestive of UTI
Breast engorgement usually develops by 7th -2st day of postpartum and in the given case it’s too soon for it to occur.
As it is expected during the first 2 hours postpartum, Atelectasis is unlikely to be the cause of symptoms in the given case.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 92
Correct
-
A 41-year-old G2P1 woman who is at 30 weeks gestational age presented to the medical clinic for a routine OB visit. Upon history taking, it was noted that her first pregnancy was uncomplicated and was delivered 10 years ago. At 40 weeks then, she had a normal vaginal delivery and the baby weighed 3.17kg. In her current pregnancy, she has no complications and no significant medical history. She is a non-smoker and has gained about 11.3 kg to date. She also declined any testing for Down syndrome even if she is of advanced maternal age. Upon further examination and observation, the following are her results: Blood pressure range has been 100 to 120/60 to 70. Fundal height measures only 25 cm. Which of the following is most likely the reason for the patient’s decreased fundal height?
Your Answer: Fetal growth restriction
Explanation:A fundal height measurement is typically done to determine if a baby is small for its gestational age. The measurement is generally defined as the distance in centimetres from the pubic bone to the top of the uterus. The expectation is that after week 24 of pregnancy the fundal height for a normally growing baby will match the number of weeks of pregnancy — plus or minus 2 centimetres.
A fundal height that measures smaller or larger than expected — or increases more or less quickly than expected — could indicate:
– Slow fetal growth (intrauterine growth restriction)
– A multiple pregnancy
– A significantly larger than average baby (fetal macrosomia)
– Too little amniotic fluid (oligohydramnios)
– Too much amniotic fluid (polyhydramnios). -
This question is part of the following fields:
- Obstetrics
-
-
Question 93
Correct
-
Which organism is the most common cause of puerperal sepsis?
Your Answer: Group A Streptococcus
Explanation:Puerperal sepsis is defined as sepsis occurring after birth until 6 weeks postnatal. The most common cause of puerperal sepsis is Group A streptococcus. Until 1937, puerperal sepsis was the major cause of maternal mortality. The discovery of sulphonamides in 1935 and the simultaneous reduction in the virulence of the haemolytic streptococcus resulted in a dramatic fall in maternal mortality.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 94
Incorrect
-
A 25-year-old woman presented to the medical clinic due to fever and dysuria which has been going on for the past 3 days. The presence a pruritic, erythematous vulvar rash that is particularly painful during urination was also noted on the patient. Upon history taking, she mentioned that she is sexually active with one partner, and they use condoms inconsistently. Physical examination was done and the following are her results: Temperature is 38.7 deg C, Blood pressure is 120/80mmHg, Pulse is 84/min. Abdominal examination was done and revealed that there is suprapubic fullness. Upon pelvic examination, the presence of several tender ulcerated lesions with circular borders on the inside of the left labia minora were noted. Speculum examination revealed no cervical friability or mucopurulent discharge. There is also enlarged and tender left inguinal lymph nodes. Urethral catheterization was then performed due to difficulty with spontaneous voiding. The results of her urinalysis are as follows: Leukocyte esterase = positive, Nitrites = negative, Bacteria = none, White blood cells = 15/hpf. Her urine pregnancy test turned out negative. Which of the following tests will most likely be considered to establish the patient’s diagnosis?
Your Answer: Rapid plasma reagin testing for Treponema pallidum
Correct Answer: Viral culture of lesion for herpes simplex virus
Explanation:While HSV-1 often affects the perioral region and can be known to cause genital lesions, HSV-2 is more commonly the consideration when patients present with genital lesions.
HSV-2 is transmitted through direct contact of sections in a seropositive individual who is actively shedding the virus. The virus preferentially affects the skin and mucous membranes with the virus invading epithelial cells on initial exposure and ultimately replicating intracellularly at that site.HSV-2, in particular, may present as a primary infection with painful genital ulcers, sores, crusts, tender lymphadenopathy, and dysuria. The classical features are of macular or papular skin and mucous membrane lesions progressing to vesicles and pustules that often last for up to 3 weeks. Genital lesions can be especially painful, leading to swelling of the vulva in women, burning pain, and dysuria.
Given that symptoms can mimic acute urinary tract infection, consider urinalysis and culture.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 95
Incorrect
-
Whilst reviewing a 34 year old patient with amenorrhoea in clinic they tell you they have gained over 10kg in weight in the past 8 weeks and have noticed worsening acne. Routine bloods taken that morning show a random glucose 11.1mmol/l, normal thyroid function tests and negative pregnancy test. BP is 168/96 mmHg. You suspect Cushing's. What would the most appropriate investigation be to conform the diagnosis?
Your Answer: Random serum ACTH
Correct Answer: Dexamethasone suppression test
Explanation:In Cushing’s syndrome there is excess cortisol. Causes are broadly divided into 2 types: ACTH dependent disease: excess ACTH from the pituitary (Cushing’s disease), ectopic ACTH-producing tumours or excess ACTH administration. Non-ACTH-dependent: adrenal adenomas, adrenal carcinomas, excess glucocorticoid administration. The recommended diagnostic tests for the presence of Cushing’s syndrome are 24-hour urinary free cortisol, 1 mg overnight dexamethasone suppression test and late-night salivary cortisol. There are several other tests that may also be performed to find the cause. ACTH and cortisol measured together may show if this is ACTH dependent or not. MRI pituitary and CT abdo and pelvis may show if tumour is the cause.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 96
Incorrect
-
In early pregnancy at what gestation does the Embryonic pole become visible on transvaginal ultrasound?
Your Answer: 4 weeks + 3 days
Correct Answer: 5 weeks + 3 days
Explanation:The embryonic pole becomes visible on transvaginal ultrasound at around 5 and a half to 6 weeks gestation when it measures around 3mm.
-
This question is part of the following fields:
- Biophysics
-
-
Question 97
Correct
-
After eating a burger at a local restaurant, a 27-year-old lady comes to your office with nausea, vomiting, and diarrhoea. She's taking oral contraceptives. Even when she was quite unwell, she did not miss her pills. Which of the following would be the best piece of contraceptive and pill advise you could give her?
Your Answer: She should continue the pills and use condom for 7 days
Explanation:If diarrhoea occurs within 24 hours of taking oral birth control or continues for 24 to 48 hours after taking a pill, an additional dose is not needed.
If diarrhoea lasts more than 48 hours the patient should use backup birth control, such as condoms, or avoid sexual intercourse until pills have been taken for seven diarrhoea-free days.
Options to stop pills are incorrect as it increases risk of pregnancy.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 98
Incorrect
-
A patient is about to undergo an elective C-section. She wants to know how long it will take for her wound to completely heal. How much time does it take for healing by primary intention to reach full tensile strength?
Your Answer: 6 weeks
Correct Answer: 12 weeks
Explanation:Wound healing typically undergoes different stages that include haemostasis, inflammation, proliferation and remodelling. The phases are often shortened when healing occurs by primary intention such as in a surgical wound. Remodelling, which is the major strengthening phase, takes about 3 weeks, while it takes a total of 12 weeks to reach maximum tensile strength.
-
This question is part of the following fields:
- Physiology
-
-
Question 99
Correct
-
Question 100
Correct
-
In the earliest phase of wound healing platelets are held together by what?
Your Answer: Fibrin
Explanation:The 1st stage of wound healing is haemostasis. Even in incised wounds a small haematoma forms. Here the clotting cascade is activated by tissue factor and endothelial cells resulting in activation of platelets. This results in platelet aggregation and the laying down of a fibrin mesh that is cross linked and holds the platelets in place.
Wound healing is typically divided into phases:
1. Haemostasis Phase
2. Inflammatory phase
3. Proliferation phase
4. Remodelling phase -
This question is part of the following fields:
- Physiology
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)