-
Question 1
Incorrect
-
In pregnancy, the following lung function value remains unchanged:
Your Answer: Tidal Volume
Correct Answer: FEV1
Explanation:The biochemical and mechanical effects of progesterone and the enlarging uterus are responsible for some changes in lung function during pregnancy.
Progesterone increases the sensitivity of the respiratory centre to arterial carbon dioxide while also causing hyperaemia in the airway leading to nasal obstruction. As a result, minute ventilation and tidal volume increase by 50% to allow greater arterial oxygen saturation.
The enlarging uterus displaces the diaphragm upwards, and also limits the movement of the thoracic cage, thereby decreasing the functional residual capacity (FRC) and the expiratory reserve volume (ERV) by 20%.
Functional Expiratory Volume in 1 second (FEV1) and Forced Vital Capacity (FVC) remain unchanged in pregnancy.
-
This question is part of the following fields:
- Physiology
-
-
Question 2
Correct
-
A 27-year-old female reports to the emergency department due to severe right lower quadrant pain. Complaints started yesterday, as the patient noticed intermittent right lower abdominal pain associated with increased activity. She rested for remainder of the day, but the pain still continued to increase. An hour ago, the pain suddenly became constant and severe, associated with nausea and vomiting.The patient does not complaint of any radiation of pain. On examination patient's temperature is noted to be 37.2 C (99 F), blood pressure is 130/80 mm Hg, and pulse rate is 98/min.On palpation of the right lower quadrant there is tenderness without rebounding or guarding.Urine pregnancy test conducted came to be negative. Considering the following additional informations, which would be most appropriate in establishing the diagnosis of this patient?
Your Answer: History of ovarian cysts
Explanation:Common Risk factors for Ovarian torsion are presence of an ovarian mass, women who are in their reproductive age and history of infertility treatment with ovulation induction.
Common clinical presentations include sudden onset of unilateral pelvic pain along with nausea & vomiting and presence of a palpable adnexal mass. An adnexal mass with absent Doppler flow to ovary can be noted in ultrasound.
Laparoscopy with detorsion, ovarian cystectomy and oophorectomy if necrosis or malignancy is found are the common treatment options.Acute lower abdominal pain in a nonpregnant women can have various causes including pathologies of the gastrointestinal, gynecologic, or urologic systems due to the close proximity of these structures. All of these cases have classic presentations which help to characterize the disease process and thereby to differentiate the diagnosis.
In the given case, patient presents with right lower quadrant pain which is classic for ovarian torsion, occurring due to rotation of the ovary around the infundibulopelvic ligament, causing ovarian vessel occlusion. Although ovarian torsion can occur in any women in their reproductive-age, is seen more commonly in those with a history of ovarian cysts (eg, hemorrhagic cyst) or masses (eg, mature cystic teratoma) because of the greater size and density of the ovary which makes it prone to rotation and subsequent torsion. Patients will initially have intermittent pain associated with activity, as in this patient, due to partial ovarian torsion, this initial pain resolves when the adnexa spontaneously untwists and blood flow returns. When this progresses to complete ovarian torsion, patients typically develop sudden-onset, severe, nonradiating pain due to persistent ischemia, which is often associated with nausea and vomiting.
Ovarian torsion can be clinically diagnosed, but a Doppler ultrasound is performed to evaluate ovarian blood flow and also to confirm the diagnosis. Surgical detorsion to prevent ovarian necrosis and cystectomy/oophorectomy are the usual treatment options.
Any association of urinary symptoms will help to establish a urologic cause of acute right lower quadrant pain like pyelonephritis, nephrolithiasis, etc. However, patients with urologic conditions typically presents with suprapubic or flank pain which radiates to the right lower quadrant, making this diagnosis less likely in the given case.
A family history of malignancy usually does not aid in the diagnosis of acute lower abdominal pain. Although some ovarian cancers are inherited, patients with ovarian cancer typically have a chronic, indolent course with associated weight loss, early satiety, and abdominal distension.
Having multiple sexual partners is considered a risk factor for sexually transmitted infections and pelvic inflammatory disease, which can be a cause for lower abdominal pain. However, patients will typically have fever, constant and diffused pelvic pain along with rebound and guarding.
Recent sick contacts are a risk factor for gastroenteritis, which can present with nausea, vomiting and abdominal pain. However, in this case patient will typically have diffuse, cramping abdominal pain which will worsen gradually; along with persistent vomiting and diarrhea.
Ovarian torsion typically causes intermittent lower abdominal pain followed by sudden-onset of severe, nonradiating unilateral pain with associated nausea and vomiting. Ovarian torsion can occur in women in their reproductive-age, particularly those with a history of ovarian cysts.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 3
Correct
-
In twin deliveries: Which is true?
Your Answer: There is increased risk of postpartum haemorrhage
Explanation:Twin gestations are at increased risk for postpartum haemorrhage (PPH). A number of maternal and peripartum factors are associated with PPH requiring blood transfusion in twin gestations. Reducing the rate of caesarean delivery in twin pregnancies may decrease maternal hemorrhagic morbidity.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 4
Correct
-
During vertex presentation, the position is determined by relationship of which part of the fetal vertex to the mother's pelvis?
Your Answer: Occiput
Explanation:A cephalic presentation is the one where head of the foetus enters the pelvic cavity at the time of delivery. The commonest form of cephalic presentation is the vertex presentation in which the occiput of the foetus enters the birth canal.
-
This question is part of the following fields:
- Anatomy
-
-
Question 5
Correct
-
A patient admitted to the medical ward complains of a mild fever and vaginal discharge. Clue cells are seen on microscopy from a vaginal swab. Which of the following infections feature clue cells?
Your Answer: Bacterial Vaginosis
Explanation:Bacterial vaginosis (BV) is a common infection of the vagina caused by the overgrowth of atypical bacteria, most commonly Gardnerella vaginalis, a gram-negative rod. In diagnosing BV, a swab is taken for microscopy, often revealing clue cells. Clue cells are cells of the vaginal epithelium which are covered by adherent Gardnerella, giving them a distinctive look under the microscope. Though many are asymptomatic, some infected women complain of a greyish, foul-smelling vaginal discharge. Their vaginal fluid pH may also become more alkaline. BV does not however present with pyrexia, so the lady’s fever could be attributed to another cause as she is still a patient on the medical ward.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 6
Correct
-
According to the RCOG Green-top guidelines on prevention and management of post-partum haemorrhage (PPH) which of the following statements is true?
Your Answer: For women delivering by caesarean section, Oxytocin 5 iu by slow IV injection should be used
Explanation:Misoprostol is not as effective as oxytocin but may be used if Oxytocin is not available e.g. home birth Recommended doses of Oxytocin For vaginal deliveries: 5 iu or 10 iu by intramuscular injection. For C-section: 5 iu by IV injection
-
This question is part of the following fields:
- Clinical Management
-
-
Question 7
Correct
-
The lower part of the rectum is supplied by the middle rectal artery. What is the middle rectal artery a branch of?
Your Answer: Internal iliac artery
Explanation:The middle rectal artery arises from the anterior division of the internal iliac artery.
-
This question is part of the following fields:
- Anatomy
-
-
Question 8
Incorrect
-
Anna, a 39-year-old medical receptionist presents to your gynaecologic clinic for a refill of her Microgynin 30 (combined oral contraceptive pill). Her history is significant for smoking around 1 pack per day. Her BMI is 37. What should be the next management step?
Your Answer: Write a script for Microgynin
Correct Answer: Offer her progestogen-only contraceptive options
Explanation:This patient is above 35 and smokes more than 15 cigarettes per day, which is an absolute contraindication to using a combined oral contraceptive pill. A BMI of greater than 35 is a relative contraindication to the usage of the combined oral contraceptive pill.
Progestogen-only contraception, such as etonogestrel implant, levonorgestrel intrauterine device, and depot medroxyprogesterone, should be offered to her.
Without initially attempting lifestyle changes, a referral for weight loss surgery is not required. Also, nicotine replacement therapy may aid in quitting smoking, but it may take time. -
This question is part of the following fields:
- Gynaecology
-
-
Question 9
Incorrect
-
Raised FSH levels are found in all of the following conditions, EXCEPT:
Your Answer: Postmenopausal women
Correct Answer: Women on combined oral contraceptive pills
Explanation:Oestrogen- and progesterone-containing oral contraceptives inhibit LH, which suppresses the FSH and LH levels, preventing follicular development and ovulation. Combined pills suppress FSH and LH throughout the cycle, inhibit endometrial proliferation, and produce a scanty cervical mucus.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 10
Incorrect
-
What is the life span of the corpus luteum in days?
Your Answer: 26-30
Correct Answer: 14-16
Explanation:After the release of the oocyte, the theca and the granulosa cells form the corpus luteum which undergoes extensive vascularization for continued steroidogenesis. Progesterone is secreted by the luteal cells and is synthesized from cholesterol. The luteal phase lasts for 14 days and if implantation does not occurs the corpus luteum starts to degenerate. As B-HCG produced by the implanted embryo maintains it and without it luteolysis occurs.
-
This question is part of the following fields:
- Embryology
-
-
Question 11
Correct
-
At what angle is the plane of the pelvic inlet to the anatomical horizontal plane?
Your Answer: 60
Explanation:The female pelvic inlet tilts at an inclination that is about 60 degrees from the anatomical horizontal plane. This tilt is maintained by muscles and fascia. The pelvic outlet slopes at an angle of 15 degrees.
-
This question is part of the following fields:
- Anatomy
-
-
Question 12
Incorrect
-
High levels of alpha feto protein are found in all, EXCEPT?
Your Answer: Certain ovarian cancers
Correct Answer: Trisomy 21
Explanation:Pregnant maternal serum AFP levels elevated: Neural tube defects (e.g., spina bifida, anencephaly); Omphalocele; Gastroschisis.
Pregnant maternal serum AFP low levels: Down syndrome
-
This question is part of the following fields:
- Endocrinology
-
-
Question 13
Correct
-
A 25 year old primigravida with a regular cycle had her last menstrual period on June 30th. Therefore the expected date of delivery (EDD) is approximately when the following year:
Your Answer: 7-Apr
Explanation:Expected date of delivery (EDD) is a calculated from the first day of the woman’s last menstrual period. If her periods are regular i.e., 28-day menstrual cycle, Naegele’s rule may be used. Naegele’s rule involves a simple calculation: add seven days to the first day of your LMP and then subtract three months. e.g. 30 June + 7 days = 7 July, minus 3 months = 7 April.
-
This question is part of the following fields:
- Physiology
-
-
Question 14
Correct
-
Which of the following factors is fetal nutrition dependant on?
Your Answer: All of the options given
Explanation:Fetal nutrition is dependant upon multiple factors such as maternal nutritional state, quality of maternal diet, malnutrition, anorexia nervosa, metabolic rate of the mother or whether they suffer from malabsorption syndrome or other related conditions.
-
This question is part of the following fields:
- Physiology
-
-
Question 15
Correct
-
Hirsutism can be found in all of the following conditions, EXCEPT:
Your Answer: Patient on oral contraceptive pills
Explanation:Classically, hirsutism has been considered a marker of increased androgen levels in females from increased production of androgens (i.e. testosterone) either by the adrenals or due to an ovarian disease. The ovarian causes for hyperandrogenism are polycystic ovarian syndrome (PCOS) and ovarian tumours. Adrenal causes include Cushing’s syndrome, androgen-producing tumours, and congenital adrenal hyperplasia (CAH), most commonly due to 21-hydroxylase deficiency. Less common causes include the hyperandrogenic-insulin resistant-acanthosis nigricans syndrome (HAIRAN). Hyperprolactinemia by increasing adrenal dehydroepiandrosterone sulphate (DHEA-S) production may cause hirsutism. Androgenic drugs are also an important cause of hirsutism. About 20% of the patients may present with idiopathic hirsutism (IH) with normal androgen levels and ovarian function. The cause of increased hair in these women is thought to be related to disorders in peripheral androgen activity. Onset of IH occurs shortly after puberty with slow progression. PCOS and IH account for 90% of the hirsutism in women. Hirsutism can also occur in some premenopausal women and continue for a few years after menopause. This is due to decrease in ovarian oestrogen secretion with continuous androgen production.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 16
Incorrect
-
You are consenting a patient for a diagnostic hysteroscopy. What is the approximate risk of uterine perforation in diagnostic hysteroscopy?
Your Answer: 0.50%
Correct Answer: 0.10%
Explanation:The risk of uterine perforation is 0.1% during therapeutic hysteroscopy.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 17
Incorrect
-
When deciding on entry method for laparoscopy a patients build is important. Which of the following entry methods is inappropriately matched to the patient?
Your Answer: Hasson technique entry into obese patient (BMI 40)
Correct Answer: Varess needle entry in a very thin patient (BMI 16)
Explanation:In patients with normal BMI there is no preferential entry method. The Varess technique is not appropriate for morbidly obese or very thin patients for the reasons set out below: Morbid Obesity (BMI>40): Hasson technique or entry at Palmers point Reason: difficult penetration with Varess needle Very Thin Patients: Hasson technique or insertion at Palmers point Reason: higher risk of vascular injury
-
This question is part of the following fields:
- Clinical Management
-
-
Question 18
Correct
-
Looking at the picture below what is the diagnosis?
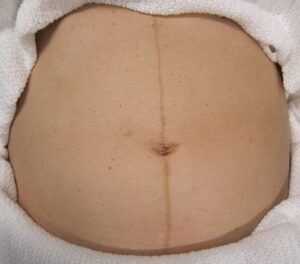
Your Answer: Linea Nigra
Explanation:This is Linea Nigra. It occurs in 3/4 of pregnancies and is due to increased melanocyte-stimulating hormone production by the placenta. This also causes melasma and darkening of the nipples.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 19
Incorrect
-
A 28-year-old woman who recently got married presents to your clinic. She has a history of extremely irregular menstrual cycles with the duration varying between four and ten weeks. She had attended her routine review appointment one week prior to her current presentation. At that time she had stated that her last period had occurred six weeks previously. You had recommended the following tests for which the results are as shown below: Serum follicle-stimulating hormone (FSH): 3 IU/L (<13), Serum luteinising hormone (LH): *850 IU/L (4-10 in follicular phase, 20-100 at mid-cycle), Serum prolactin (PRL): 475 mU/L (50-500). Which one of the following is the most probable reason for her amenorrhoea?
Your Answer: An LH-producing pituitary adenoma.
Correct Answer: Early pregnancy.
Explanation:All of the options provided could cause amenorrhoea and therefore need to be evaluated.
The luteinising hormone (LH) level reported here is exceedingly elevated. A patient with polycystic ovarian syndrome (PCOS) is unlikely to have such a raised level, but it could be because of a LH-producing adenoma. Such tumours are, however, extremely rare.
Early pregnancy (correct answer) is the most likely cause of this woman’s elevated LH level. This would be due to the presence of beta human chorionic gonadotropin (hCG) hormone that is produced during pregnancy.
LH and beta-HCG both have similar beta-subunits and cross-reactions are commonly noted in LH assays.
The serum prolactin (PRL) level is at the upper end of the normal range and this correlates to the levels observed in the early stages of pregnancy.
The follicle-stimulating hormone (FSH) levels remain low during early pregnancy.
If her amenorrhea had been caused by stress from her recent marriage, the LH level would have been normal or low.
If the cause was premature ovarian failure, the FSH level would have been significantly higher.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 20
Correct
-
Skin changes during pregnancy should include:
Your Answer: All of the options given
Explanation:Skin signs during pregnancy may include: dark spots on the breasts, nipples and inner thighs, melasma (chloasma), linea nigra, stretch marks, acne, spider telangiectasis and varicose veins.
-
This question is part of the following fields:
- Physiology
-
-
Question 21
Correct
-
A young couple, both 26 years of age, presents to you with 11 months’ duration of infertility. On investigation, she is found to be ovulating, and her hysterosalpingogram is normal. On semen analysis, the following results were found: Semen volume 5mL (2-6 mL) Sperm count 1 million/mL * (>20 million) Motility 15% (>40%) Abnormal forms 95% (<60%) A second specimen three months later confirms the above results. Which would be the most suitable next step in management?
Your Answer: Carry out in vitro fertilisation (IVF) using intracytoplasmic sperm injection (ICSI).
Explanation:Achieving spontaneous pregnancy is rare in cases where a couple have been infertile with abnormal semen analysis (count <5million/mL and reduced motility), hence there is generally an indication for treatment. FSH injection usually would not be expected to improve the semen specimen. Rate of pregnancy would be much lower if at the time of intrauterine insemination, the total motile count is less 5 million. In this case, his count is 1 million. Pregnancy is likely to be achieved with donor sperm but as it would not contain the husband’s genetic material, it would be only considered later on once all other methods involving his own sperm have failed. Out of all the options, IVF would most likely result in a pregnancy, in which it allows the husband’s sperm to spontaneously fertilise the oocyte. Rate of pregnancy would roughly be 2% per treatment cycle. This rate would increase to roughly 20% if ISCI is also used.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 22
Correct
-
Which of the following hormones is secreted by the corpus luteum in a non pregnant state?
Your Answer: Progesterone
Explanation:The corpus luteum is formed from the granulosa cells of the mature follicle. The structure functions as a transient endocrine organ which secretes mainly progesterone with additional secretion of oestradiol and inhibin, which serve to suppress FSH levels. In the event of no pregnancy, the corpus luteum stops producing progesterone and degenerates into the corpus albicans.
-
This question is part of the following fields:
- Embryology
-
-
Question 23
Correct
-
A patient who has been seen in fertility clinic phones regarding the timing of her progesterone blood test. She has regular 35 day menstrual cycles. When testing for ovulation what day of her cycle should she have the test on?
Your Answer: 28
Explanation:When testing for ovulation the best test is to check the progesterone level. The mid luteal progesterone levels should be checked 7 days prior to the next period. That will be the 28th day in a 35 day cycle.
-
This question is part of the following fields:
- Data Interpretation
-
-
Question 24
Correct
-
A 30-year-old primigravida was admitted to the hospital in active labor. On admission, her cervix was 7 cm dilated and 100% effaced. She received epidural anesthesia and proceeded to complete cervical dilation with fetal head at +3 station within a few hours.Patient who has been pushing for 4 hours is exhausted now and says she cannot feel her contractions, nor knows when to push because of the epidural anesthesia.Patient had no complications during the pregnancy and has no chronic medical conditions. Estimated fetal weight by Leopold maneuvers is 3.4 kg (7.5 lb), patient's vital signs are normal and fetal heart rate tracing is category 1.Tocodynamometer indicates contractions every 2-3 minutes and a repeat cervical examination shows complete cervical dilation with the fetal head at +3 station, in the left occiput anterior position with no molding or caput. Among the following, which is considered the best next step in management of this patient?
Your Answer: Perform vacuum-assisted vaginal delivery
Explanation:The period from attaining a complete cervical dilation of 10 cm to fetal delivery is considered as the second stage of labor. In the given case patient have achieved an excellent fetal descent to +3 due to her average-sized infant of 3.4 kg, suitable pelvis (no fetal molding or caput, suggesting no resistance against the bony maternal pelvis), and a favorable fetal position of left occiput anterior.
But with no further fetal descent the patient fulfills the following criterias suggestive of second-stage arrest like:
≥3 hours of pushing in a primigravida without an epidural or ≥4 hours pushing with an epidural, as in this patient
OR
≥2 hours of pushing in a multigravida without an epidural or ≥3 hours pushing with an epidural.As continued pushing without any effect will lead to complications like postpartum hemorrhage, limiting the chances of spontaneous vaginal delivery, it is better to manage this case by operative vaginal delivery procedures like vacuum-assisted delivery, to expedite delivery. maternal exhaustion, fetal distress, and maternal conditions like hypertrophic cardiomyopathy, in which the Valsalva maneuver is not recommended are the other indications for performing an operative vaginal delivery.
Fundal pressure is the technique were external pressure is applied to the most cephalad portion of the uterus, were the applied force is directed toward the maternal pelvis. The maneuver was not found to be useful in improving the rate of spontaneous vaginal deliveries.
Epidurals will not arrest or affect spontaneous vaginal delivery rates, instead they just lengthen the second stage of labor. Also an appropriate analgesia is a prerequisite to use in operative vaginal delivery.
Manual rotation of an infant to a breech presentation for breech vaginal delivery is called as internal podalic version. It is contraindicated in singleton deliveries due to the high risk associated with breech vaginal delivery in regards to neonatal mortality and morbidity.
The ideal fetal head position in vaginal delivery is occiput anterior (OA) as the flexed head in this provides a smaller diameter and facilitates the cardinal movements of labor. The occiput posterior (OP) position, in contrast to OA, presents with a larger-diameter head due to the deflexed position. So the chance for spontaneous vaginal delivery will be decreased if fetal head is rotated to OP position.
A lack of fetal descent after ≥4 hours of pushing in a primigravida with an epidural (≥3 hours without) or ≥3 hours in a multigravida with an epidural (≥2 hours without) is defined as second stage arrest of labor. The condition is effectively managed with operative vaginal delivery procedures like vacuum-assisted delivery. Other common indications for operative vaginal delivery are maternal exhaustion, fetal distress, and maternal conditions where the Valsalva maneuver is not recommended.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 25
Correct
-
Which one of the following muscles is the most important muscle forming the pelvic floor?
Your Answer: Levator ani
Explanation:Levator ani muscle is composed of three different muscles i.e. iliococcygeus, pubococcygeus and the puborectalis muscle. It is the main muscle that supports the organs of the pelvic cavity.
Bulbocavernosus and Ischiocavernosus muscles are located in-between the anus and scrotum and play an important role in sexual response in males.
Superficial and deep transverse perineal muscles are located in the perinium and pass in front of the anus. -
This question is part of the following fields:
- Anatomy
-
-
Question 26
Correct
-
A patient undergoes oophorectomy and the ovarian veins are ligated. Which vein does the left ovary drain into?
Your Answer: Left renal
Explanation:When it comes to questions on venous drainage the ovarian vein is likely to be a common question given its varied drainage depending on laterality. The right ovarian vein travels through the suspensory ligament of the ovary and generally joins the inferior vena cava whereas the left ovarian vein drains into the left renal vein.
-
This question is part of the following fields:
- Anatomy
-
-
Question 27
Incorrect
-
A 24-year-old college student comes to your clinic for contraception guidance. For the past three months, she has had migraine-like headaches once or twice a month. For the past two years, she has been taking combined oral contraceptive pills. Which of the following suggestions is the most appropriate?
Your Answer: Continuation of combined oral contraceptive pills
Correct Answer: Stopping the combined oral contraceptive pills and starting progesterone only pills (POP)
Explanation:Combined oral contraceptives are a safe and highly effective method of birth control, but they can also raise problems of clinical tolerability and/or safety in migraine patients. It is now commonly accepted that, in migraine with aura, the use of combined oral contraceptives is always contraindicated, and that their intake must also be suspended by patients suffering from migraine without aura if aura symptoms appear.
Discontinuation of contraception could risk in pregnancy. Barrier methods can be used but aren’t as effective as pills.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 28
Incorrect
-
All of the following statements regarding human chorionic gonadotrophin are true except::
Your Answer: Is reversible for the maintenance of corpus luteum
Correct Answer: It's level doubles every 48 hours in ectopic pregnancy
Explanation:In normal pregnancy the levels of hCG doubles after every 48-72 hours but in case of ectopic pregnancy the levels of hCG are lower than the normal. It is produced by the placenta and its main role is nourishment of the egg after implantation. Its levels reached a peak at 8-10 weeks of pregnancy and after that the levels decreases for the remainder of pregnancy. In hydatiform mole and trophoblastic diseases its the main hormone for diagnosis of the disease because the levels are highly elevated.
-
This question is part of the following fields:
- Physiology
-
-
Question 29
Correct
-
A patient who has been seen in fertility clinic phones regarding the timing of her progesterone blood test. She has regular 35 day menstrual cycles. When testing for ovulation what day of her cycle should she have the test on?
Your Answer: 28
Explanation:The mid-luteal progesterone sample should be taken 7 days before the expected period i.e. day 21 in a 28-day cycle or day 28 of a 35 day cycle
-
This question is part of the following fields:
- Data Interpretation
-
-
Question 30
Correct
-
Which one of the following methods helps determine the fetal position and presentation?
Your Answer: Leopold's manoeuvre
Explanation:Fetal position and presentation is best evaluated by Leopold’s manoeuvre. It will determine which part of the foetus is in the uterine fundus.
Cullen’s sign is found in ruptured ectopic pregnancy characterised by bruising and oedema of the periumbilical region.
Mauriceau-Smelli-Veit manoeuvre is done during a breech delivery. -
This question is part of the following fields:
- Obstetrics
-
-
Question 31
Incorrect
-
A 32-year-old woman, gravida 2 para 1, at 40 weeks gestation is admitted to the hospital due to contractions and spontaneous rupture of membranes.Patient underwent a cesarean delivery with her first child due to breech presentation, but this pregnancy has been uncomplicated.She has no chronic medical conditions and is taking only a prenatal vitamin. Her pre-pregnancy BMI was 20 kg/m2 and she has gained 15.9 kg (35 lb) during pregnancy. On examination her blood pressure is found to be 130/80 mm Hg. The patient is admitted and epidural anesthesia is administered with an intrauterine pressure catheter in place.She quickly dilates to 10 cm with the fetal vertex at 0 station, occiput transverse. Four hours later, the pelvic examination is unchanged but there is molding and caput on the fetal head. Fetal monitoring is category I. Contractions occur every 2-3 minutes and the patient pushes with each contraction. The contraction strength is an average of 210 MVU every 10 minutes. Which among the following is most likely the etiology for this patient’s clinical presentation?
Your Answer: Contraction inadequacy
Correct Answer: Fetal malposition
Explanation:Condition where there is insufficient fetal descent after pushing for ≥3 hours in nulliparous and ≥2 hours if multiparous women is defined as Second stage arrest of labor. Common risk factors for this presentation are maternal obesity, excessive weight gain during pregnancy and diabetes mellitus. Cephalopelvic disproportion, malposition, inadequate contractions and maternal exhaustion are the common etiologies of Second stage arrest of labor. Management includes Operative vaginal delivery or cesarean delivery as indicated in the case.
The second stage of labor begins with the dilatation of cervix to 10 cm and will end with fetal delivery. Parity and use of neuraxial anesthesia are the two factors which will affect the duration of second stage of labor and fetal station, which measures the descent of the fetal head through the pelvis determines its progression.
When there is no fetal descent after pushing for ≥3 hours or ≥2 hours in in nulliparous and multiparous patients respectively the condition is called an arrested second stage of labor. As her first delivery was a cesarean session due to breech presentation, this patient in the case is considered as nulliparous.
Most common cause of a protracted or arrested second stage is fetal malposition, which is the relation between the fetal presenting part to the maternal pelvis. Occiput anterior is the optimal fetal position as it facilitates the cardinal movements of labor, any deviations from this position like in occiput transverse position, can lead to cephalopelvic disproportion resulting in second stage arrest.
Inadequate contractions, that is less than 200 MVU averaged over 10 minutes, can lead to labor arrest but contractions are adequate in case of the patient mentioned.
Second stage arrest can be due to maternal obesity and excessive weight gain during pregnancy but this patient had a normal pre-pregnancy BMI of 20 kg/m2 and an appropriate weight gain of 15.9 kg 35 lb. So this also cannot be the reason.Maternal expulsive efforts will change the fetal skull shape. This process called as molding helps to facilitate delivery by changing the fetal head into the shape of the pelvis. Whereas prolonged pressure on head can result in scalp edema which is called as caput, presence of both molding and caput suggest cephalopelvic disproportion, but is not suggestive of poor maternal effort.
Patients with a prior history of uterine myomectomy or cesarean delivery are at higher risk for uterine rupture. In cases of uterine rupture, the patient will present with fetal heart rate abnormalities, sudden loss of fetal station (eg, going from +1 to −3 station) along with fetal retreat upward and into the abdominal cavity through the uterine scar due to decreased intrauterine pressure. In the given case patient’s fetal heart rate tracing is category 1 and fetal station has remained 0 which are non suggestive of uterine rupture.
When there is insufficient fetal descent after pushing ≥3 hours in nulliparous patients or ≥2 hours in multiparous patients is considered as second stage arrest of labor. The most common cause of second stage arrest is cephalopelvic disproportion, were the fetus presents in a nonocciput anterior position called as fetal malposition.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 32
Correct
-
A 26 year old patient with a past medical history of 2 terminations of pregnancies over the past 2 years, presents to the emergency centre complaining of severe abdominal pain and some vaginal bleeding. She has a regular 28 day cycle, and is on an oral contraceptive pill, but missed last month's period. Her last termination was over 6 months ago. She smokes almost a pack of cigarettes a day. Which of the following is the most likely diagnosis?
Your Answer: Ectopic pregnancy
Explanation:The clinical picture demonstrated is most likely that of a ruptured ectopic pregnancy. The period of amenorrhea may point to pregnancy, while the past medical history of 2 recent terminations of pregnancy may indicate a failure of her current contraceptive method. Smoking cigarettes have been shown to not only decrease the efficacy of OCPs, but also serve as a known risk factor for ectopic pregnancy. The lady is unlikely to have endometritis as her last termination was over 6 months ago. The lack of fever helps to make appendicitis, PID and pyelonephritis less likely, though they are still possible.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 33
Incorrect
-
A 43-year-old woman complains of a greenish foul smelling discharge from her left nipple. She has experienced the same case before. What is the most likely diagnosis?
Your Answer: Breast abscess
Correct Answer: Duct ectasia
Explanation:Mammary duct ectasia occurs when the lactiferous duct becomes blocked or clogged. This is the most common cause of greenish discharge. Mammary duct ectasia can mimic breast cancer. It is a disorder of peri- or post-menopausal age.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 34
Incorrect
-
The major cause of the increased risk of morbidity & mortality among twin gestation is:
Your Answer: Congenital anomalies
Correct Answer: Preterm delivery
Explanation:Twin pregnancy is associated with a number of obstetric complications, some of them with serious perinatal consequences, especially for the second twin. The rate of perinatal mortality can be up to six times higher in twin compared to singleton pregnancies, largely due to higher rates of preterm delivery and fetal growth restriction seen in twin pregnancies. Preterm birth and birth weight are also significant determinants of morbidity and mortality into infancy and childhood. More than 50% of twins and almost all triplets are born before 37 weeks of gestation and about 15–20% of admissions to neonatal units are associated with preterm twins and triplets.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 35
Incorrect
-
In which of the following situations are mini-pills unsafe to use?
Your Answer: Hypertension
Correct Answer: Ovarian cysts
Explanation:Progestin only pills increase the risk of developing follicular cysts. Sonographic studies have observed that follicular cysts are more common in POP users than women not using hormones. The follicular changes tend to increase and regress over time. No intervention is required in asymptomatic women, other than reassurance. POP users who have persistent concerns about ovarian follicular changes should be offered another method of contraception.
All other options are not contraindications to the use of mini-pills.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 36
Correct
-
A 35-year-old woman, gravida 2 para 1, at 14 weeks of gestation comes to the office for a routine prenatal visit. She is feeling well and has no concerns. The patient had daily episodes of nausea and vomiting for the first few weeks of her pregnancy and those symptoms resolved 2 weeks ago. She has had no pelvic pain or vaginal bleeding, and is yet to feel any fetal movements. Her first pregnancy ended in a cesarean delivery at 30 weeks of gestation due to breech presentation, complicated with severe features of preeclampsia. Patient has no other significant chronic medical conditions and her only medication is a daily dose of prenatal vitamin and have not reported of any medication allergies. The patient does not use tobacco, alcohol or other illicit drugs. On examination her blood pressure is 112/74 mm of Hg and BMI is 24 kg/m2.Fetal heart rate is found to be 155/min.The uterus is gravid and nontender and the remainder of the examination is unremarkable. Which of the following is considered to be the next best step in management of this patient?
Your Answer: Low-dose aspirin
Explanation:Preeclampsia prevention
Preeclampsia is defined as a new-onset hypertension along with other features like proteinuria &/or end-organ damage at >20 weeks of gestation.
Patients with the following histories are at high risk for preeclampsia:
– Those with prior history of preeclampsia
– Those with chronic kidney disease
– Those with chronic hypertension
– Those with diabetes mellitus
– Multiple gestation
– Autoimmune disease
Patients belonging in the following criteria are at moderate risk for preeclampsia:
– Obesity
– Advanced maternal age
– NulliparityPreeclampsia is considered as the leading cause for maternal and fetal morbidity and mortality. This is due to its increased risk for complications such as stroke, placental abruption and disseminated intravascular coagulation. It is most likely caused due to abnormal vasoconstriction and increased platelet aggregation, which thereby results in placental infarction and ischemia. The condition can be effectively prevented by the administration of low-doses of aspirin at 12 weeks of gestation.
Patients with predisposing factors, such as chronic kidney disease, chronic hypertension and a history of preeclampsia, particularly with severe features or at <37 weeks gestation as in this patient, are at higher risk for developing preeclampsia.
In high risk patients, the only therapy proven to decrease the risk of preeclampsia is a daily administration of low-dose aspirin, as it inhibits platelet aggregation and helps in preventing placental ischemia. Treatment is initiated at 12 – 28 weeks of gestation, optimally before 16 weeks and is continued till delivery.Betamethasone is a drug used to accelerate fetal lung maturity in patients who are prone to imminent risk of preterm delivery before 37 weeks of gestation. In this case, if the patient develops pre-eclampsia requiring an urgent preterm delivery betamethasone will be indicated.
High-doses (4 mg) of folic acid is indicated in patients with high risk for a fetus with neural tube defects, as in those who have a history of any prior pregnancies affected or those patients who use any folate antagonist medications. In the given case patient is at average risk and requires only a regular dose of 0.4 mg which is found in most prenatal vitamins.
Intramuscular hydroxyprogesterone is indicated in pregnant patients with prior spontaneous preterm delivery due to preterm prelabor rupture of membranes, preterm labor, etc to decrease the possible risk for any recurrence. In patients who underwent preterm delivery due to other indications like preeclampsia with severe features, fetal growth restriction, etc it is not indicated.
Vaginal progesterone is administered to decrease the risk of preterm delivery in patients diagnosed with a shortened cervix, which is usually identified incidentally on anatomy ultrasound scan done between 16 and 24 weeks of gestation. This patient is currently at her 14 weeks, so this is not advisable.
Patients at high risk for pre-eclampsia, like those with preeclampsia in a prior pregnancy, are advised to start taking a daily low-dose aspirin as prophylaxis for prevention of pre-eclampsia during pregnancy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 37
Correct
-
The β-hCG curve in maternal serum in a normal pregnancy peaks at:
Your Answer: 10 weeks of pregnancy
Explanation:During the first 8 weeks of pregnancy, concentrations of hCG in the blood and urine usually double every 24 hours. Levels of the hormone typically peak at around 10 weeks, decline until 16 weeks, then remain constant.
-
This question is part of the following fields:
- Physiology
-
-
Question 38
Correct
-
A 28 year old women presents at 30 weeks complaining of intense itching particularly on the hands and feet that is worse in the evenings. She has taken cetirizine but this hasn't settled her symptoms. Examination is unremarkable with no rash. What is the likely diagnosis
Your Answer: Intrahepatic Cholestasis of Pregnancy
Explanation:The history is typical of Intrahepatic Cholestasis of Pregnancy, also known as obstetric cholestasis and prurigo gravidarum. The features are: Intense itching typically of the hands and feet Itch gets worse at night Responds poorly to antihistamines There is no rash. The mechanism is poorly understood but tests may show deranged LFTs. It usually resolves quickly after delivery. The other diagnoses listed are possible though less likely. Scabies normally has a rash
-
This question is part of the following fields:
- Clinical Management
-
-
Question 39
Correct
-
You see a patient in fertility clinic who you suspect has Klinefelters. What is the likely karyotype?
Your Answer: 47XXY
Explanation:Klinefelter syndrome occurs in 1:1000 individuals. They are phenotypically male and genotypically they have 47,XXY chromosomes. These individuals have small testes, are tall with disproportionate long lower limbs.40% will also have gynecomastia.
-
This question is part of the following fields:
- Genetics
-
-
Question 40
Incorrect
-
A 23-year-old G1P0 female presents to your department with a complaint of not having menstrual periods over the last 6 months. She had her first menstrual periods at the age of 13 and they have been consistent since then with a cycle of 28 days. She reports that she had an unplanned pregnancy 8 months ago and did an elective abortion at the 8th week of gestation. Since that time she has not had menstrual periods. She is sexually active with her boyfriend and they use condoms consistently. The pregnancy test is negative. Which of the following diagnostic tests is most likely to confirm the diagnosis?
Your Answer: Brain MRI
Correct Answer: Hysteroscopy
Explanation:This patient presents with secondary amenorrhea, most likely caused by Asherman’s syndrome- Secondary amenorrhea is defined as absence of menstruation for – 3 months in a patient who had regular menstruation previously or absence of menstruation for 9 months in a patient who had oligomenorrhea- Asherman’s syndrome as the cause of her amenorrhea is suggested by its beginning shortly after undergoing elective abortion. It is an outflow tract obstruction caused by intrauterine synechiae resulting from the procedure.
The best diagnostic test to confirm this diagnosis is hysteroscopy. It can allow visualization of the uterine cavity, the nature and extent of intrauterine synechiae.
→ Progesterone withdrawal test is one of the diagnostic studies done in the early work-up of secondary amenorrhoea- It is usually followed by the estrogen-progesterone challenge test and other tests. Progesterone withdrawal test alone would not confirm Asherman’s syndrome.
→ Pelvic ultrasound is more useful in primary amenorrhea work-up when the presence or absence of the uterus is to be confirmed- It is not very useful in the evaluation of intrauterine adhesions.
→ Brain MRI is useful in confirming the presence of pituitary tumours in patients, who are found to have high levels of prolactin. This patient’s most likely cause of secondary amenorrhea is Asherman’s syndrome.
→ TSH and prolactin levels should be the next step in the work-up of secondary amenorrhea after pregnancy has been ruled out; however, these studies cannot confirm Asherman’s syndrome. -
This question is part of the following fields:
- Obstetrics
-
-
Question 41
Incorrect
-
A 33 year old lady in her first trimester of pregnancy presented with loss of weight, abdominal pain and frequent episodes of vomiting. Her vital signs are normal. She has been given a cyclizine injection but without any significant improvement. The next step would be?
Your Answer: IV fluids
Correct Answer: IV steroids
Explanation:In hyperemesis gravidarum, IV corticosteroids can be given to reduce vomiting, if the patient is not responding to standard anti emetics.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 42
Correct
-
An 20-year-old woman presents to you 6 hours after she was raped on day-12 of her menses which usually lasts for 28 days. You have decided to give her Postinor-2 (levonorgestrel 0.75 mg) as a post-intercourse contraceptive. She is requesting information about any potential adverse effects as well as its efficacy. Which of the following statements is correct?
Your Answer: The treatment fails to prevent pregnancy in 2-3% of women treated.
Explanation:Postinor-2 (levonorgestrel 750pg) is only an emergency contraceptive and is not designed to be a regular form of contraception. If taken within 24 hours, it is estimated to be able to prevent up 97-98% of pregnancies and 58% if given between 48-72 hours post-unprotected intercourse. It can cause vaginal bleeding within a few days of its administration if it is given before day 8-10 of her menstrual cycle. However, if given mid-cycle, it typically doesn’t affect the timing of her next period unless conception occurs. Nausea and vomiting were common when high doses of OCP were used as a post-intercourse contraceptive. Nausea and vomiting still can occur with Postinor-2, but not up to 50% of women. There is currently no evidence to suggest that the levonorgestrel dose would cause a virilising effect on female foetuses.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 43
Correct
-
A 36-year-old woman presents to the gynaecology clinic with a complaint of headache, irritability, abdominal bloating, anxiety, and breast tenderness around 4 to 5 days before menstruation for the last 8 months. There's also a limitation on daily activities and she has to take a week off from work. The patient's symptoms are relieved completely with the onset of menstruation. Which of the following suggests an appropriate diagnosis?
Your Answer: Premenstrual syndrome
Explanation:This patient meets the diagnostic criteria for premenstrual syndrome.
Affective and somatic symptoms over the five days before menses in each of the three previous menstrual cycles are diagnostic criteria for premenstrual syndrome.
Affective symptoms include:
– Depression.
– Anger outbursts.
– Irritability.
– Anxiety.
– Confusion.
– social withdrawal.
Somatic symptoms include:
– breast tenderness
– abdominal bloating
– headache and swelling of extremities.
Symptoms normally disappear within four days of menstruation and are present even when no medical therapy, drugs, or alcohol are used.Premenstrual dysphoric disorder is a severe form of premenstrual syndrome marked by intense melancholy, emotional lability with frequent crying, loss of interest in daily activities, reduced focus, exhaustion, sleeplessness, and a sense of being overwhelmed or out of control.
Symptoms must have been present for the majority of the previous 12 months, interfering with daily activities.The diagnoses of generalised anxiety disorder and depression alone are doubtful.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 44
Correct
-
A 28-year-old primigravid woman at 18 weeks of gestation comes to office for a routine prenatal visit and anatomy ultrasound. Patient feels well generally and has no concerns, also has no chronic medical conditions, and her only daily medication is a prenatal vitamin. She is accompanied by her mother as her husband was unable to get off work. Ultrasound shows a cephalic singleton fetus measuring at <10th percentile consistent with severe growth restriction.There are bilateral choroid plexus cysts, clenched fists, and a large ventricular septal defect. Amniotic fluid level is normal with a posterior and fundal placenta. Which of the following statements is the most appropriate initial response by the physician?
Your Answer: There are some things about your ultrasound that I need to discuss with you; is it okay to do that now?
Explanation:SPIKES protocol for delivering serious news to patients includes:
– Set the stage includes arranging for a private, comfortable setting space, introduce patient/family & team members, maintain eye contact & sit at the same level and schedule appropriate time interval & minimize space for interruptions.
– Perception: Use open-ended questions to assess the patient’s/family’s perception of the medical situation.
– Invitation: should ask patient/family how much information they would like to know and remain cognizant of their cultural, educational & religious issues.
– Knowledge:
Warn the patient/family that serious news is coming, Speak in simple & straightforward terms, stop & check whether they are understanding.
– Empathy: Express understanding & give support when responding to emotions
– Summary & strategy: Summarize & create follow-through plan, including end-of-life discussions if applicable.The ultrasound findings of severe growth restriction, bilateral choroid plexus cysts, clenched fists, and a large ventricular septal defect are consistent with trisomy 18, the second most common autosomal trisomy, which results in fetal loss or neonatal death in the majority of cases. In this case, the physician is to deliver a very serious news to the patient who is presenting for a routine visit, believing her pregnancy was normal. When serious news is unexpected, it is especially important to prepare the patient and determine how the patient would like to receive the results.
The physician is supposed to provide a comfortable setting and must ask patient’s permission to share the results. This allows the patient to respond with her preference and avoids making assumptions about whom, if anyone, she would like to be present with. For example, some patients may prefer to defer discussion of the results until a major support person (eg, husband, mother) is present. In addition to establish patient’s preferred setting, physician should determine how much information the patient would like to receive. Some patients will prefer a detailed medical information about diagnosis and prognosis, whereas others may prefer to have time to process the news emotionally and receive further information later. The SPIKES protocol (Setting the stage, Perception, Invitation, Knowledge, Empathy, and Summary/strategy) is a six-step model that can guide physicians in delivering serious news to patients.These statements do not allow the patient to choose how she receives the results and assume that she does not want her mother present.
This statement fails to prepare the patient for serious news and prematurely jumps to sharing results using technical, medical terminology that may be difficult for the patient to comprehend. This approach could also be upsetting to a patient undergoing a routine ultrasound who is not expecting anything abnormal.
This statement inappropriately determines when and with whom the patient should receive the results. Instead the patient should be asked how she prefers to receive the results.
While delivering unexpected, serious news, physicians should prepare the patient and determine how the patient prefers to receive the information.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 45
Incorrect
-
What is the RCOG advice regarding timing of Rhesus Anti-D Immunoglobulin following abortion?
Your Answer: Anti-D IgG within 4 hours following abortion
Correct Answer: Anti-D IgG within 72 hours following abortion
Explanation:All non-sensitised RhD negative women should receive Anti-D IgG within 72 hours following abortion
-
This question is part of the following fields:
- Clinical Management
-
-
Question 46
Correct
-
Lowered haemoglobin during normal pregnancy is a physiological finding which is mainly due to:
Your Answer: Increased plasma volume
Explanation:During pregnancy, anaemia increases more than fourfold from the first to third trimester. It is a well established fact that there is a physiological drop in haemoglobin (Hb) in the mid trimester. This physiological drop is attributed to increase of plasma volume and hence decrease of blood viscosity lead to better circulation in placenta.
-
This question is part of the following fields:
- Physiology
-
-
Question 47
Correct
-
A 29 year old female presented at her 38th week of gestation to the ER with severe hypertension (210/100) and proteinuria (+++). Soon after admission, she developed generalized tonic clonic fits. What is the first line of management in this case?
Your Answer: Magnesium sulphate IV
Explanation:Magnesium Sulphate is the drug of choice in eclamptic patients. A loading dose of 4g magnesium sulphate in 100mL 0.9% saline IVI over 5min followed by maintenance IVI of 1g/h for 24h. Signs of toxicity include respiratory depression and jerky tendon reflexes. In recurrent fits additional 2g can be given. Magnesium should be stopped when the respiratory rate is <14/min, absent tendon reflexes, or urine output is <20mL/h.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 48
Correct
-
A 37 year old lady attends clinic following laparotomy and unilateral oophorectomy. The histology shows mucin vacuoles. What type of tumour would this be consistent with?
Your Answer: Mucinous
Explanation:Mucinous tumours are cystic masses which are indistinguishable from the serous tumours on gross examination except by its contents. On histology it is lined with mucin producing epithelium – mucin vacuoles whereas serous tumours have psammoma bodies. Malignant tumours are characterised by the presence of architectural complexity, cellular stratification, stromal invasion and cytological atypia.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 49
Incorrect
-
A 10 day old infant present with signs of disseminated Herpes Simplex Virus (HSV) infection. Her mother had her first episode of HSV three weeks prior to delivery. The infant was treated with antivirals upon clinical suspicion. What is the case fatality rate of infants who develop disseminated HSV despite treatment?
Your Answer: 10%
Correct Answer: 30%
Explanation:Congenital Herpes Simplex Virus infection may cause high levels of morbidity and mortality in neonates. Risk of infection with HSV 1 and 2 is highest within 6 weeks of delivery and is transferred to the neonate via maternal secretions at birth. Affected babies can present as skin manifestations, CNS infection, or disseminated infection, which carries an 85% risk of mortality if left untreated. Treatment with high dose antivirals such as acyclovir can help decrease the case mortality rate to 30% in cases of disseminated infection.
-
This question is part of the following fields:
- Microbiology
-
-
Question 50
Correct
-
Regarding anti-epileptic use in the 1st trimester of pregnancy, which of the following is closely associated with the development of congenital malformations?
Your Answer: Sodium valproate
Explanation:Sodium Valproate is known to be the most teratogenic when used in the first trimester of pregnancy. This antiepileptic increases the risk of congenital malformations including a 10-20 fold risk of neurodevelopmental defects. Though the use of antiepileptics should generally be avoided during pregnancy, carbamazepine, or newer drugs such as Lamotrigine are thought to carry less of a risk of teratogenicity.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 51
Incorrect
-
A 30 year old female with type I diabetes for 13 years, came for pre-pregnancy counselling. Which of the following is the most suitable advise for her?
Your Answer: The risks are highest for women who have a recent diagnosis of diabetes
Correct Answer:
Explanation:According to NICE guidelines women with type I diabetes, who are expecting a child should aim to keep their HbA1c level[1] below 48 mmol/mol (6.5%) without causing problematic hypoglycaemia. Women with diabetes whose HbA1c level is above 86 mmol/mol (10%) should be strongly advised not to get pregnant because of the associated risks. The risks are higher with chronic diabetes. There is an increased risk to the foetus or mother due to diabetes in pregnancy. Women who are waiting to become pregnant should take folic acid (5 mg/day) until 12 weeks of gestation to reduce the risk of having a baby with a neural tube defect.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 52
Correct
-
During pregnancy, maternal oestrogen levels increase markedly. Most of this oestrogen is produced by the:
Your Answer: Placenta
Explanation:The placenta does not have all the necessary enzymes to make oestrogens from cholesterol, or even progesterone. Human trophoblast lack 17-hydroxylase and therefore cannot convert C21-steroids to C19-steroids, the immediate precursors of oestrogen. To bypass this deficit, dehydroisoandrosterone sulphate (DHA) from the fetal adrenal is converted to estradiol-17ί by trophoblasts. In its key location as a way station between mother and foetus, placenta can use precursors from either mother or foetus to circumvent its own deficiencies in enzyme activities.
-
This question is part of the following fields:
- Physiology
-
-
Question 53
Correct
-
Your 64-year-old patient has come to you with a uterine prolapse complaint. Which of the following ligaments plays the most critical role in uterine prolapse pathophysiology?
Your Answer: Uterosacral ligament
Explanation:The uterus needs support in order to remain centered inside the pelvic cavity. The support it receives comes in two forms: dynamic and passive. The ligaments of the uterus have an important role in both.
Dynamic support is provided by the pelvic diaphragm through tonic contractions while standing and sitting and active contractions during moments of increased abdominal pressure, such as coughing or sneezing. During these moments, the ligaments of the uterus transmit the force of the diaphragm towards the organ itself, maintaining its position.
The ligaments are also crucial in providing passive support. By minimizing movement of the body and the cervix, they maintain the uterus in the typical anteverted and anteflexed position directly on top of the bladder. This provides a support for the uterus when the abdominal pressure increases.
Hence, even though the broad ligament, round ligament and ovarian ligament have some role in the suspension of the uterus, the uterosacral ligament plays the most significant role. It is also the ligament used for surgical suspension of POP.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 54
Correct
-
A 22-year-old woman walks into your clinic. She had no menstrual cycles. Her genital development appears to be within the usual range. The uterus and fallopian tubes are normal on a pelvic ultrasound. Ovaries have no follicles and just a little quantity of connective tissue. What do you think the most likely reason for her amenorrhea is?
Your Answer: Turner syndrome
Explanation:Turner syndrome is the clinical diagnosis for this patient. Turner syndrome affects women who are lacking all of one X chromosome (45, characterized by X gonadal dysgenesis).
Turner Syndrome is characterized by small stature and non-functioning ovaries, resulting in infertility and lack of sexual development. Other sexual and reproductive organs (uterus and vagina) are normal despite the inadequate or missing ovarian activity.Webbing of the neck, puffy hands and feet, coarctation of the aorta, and cardiac anomalies are all physical symptoms of Turner Syndrome. Streak gonads are also a feature of Turner syndrome.
The ovaries are replaced with fibrous tissue and do not produce much oestrogen, resulting in amenorrhea.
Until puberty, when oestrogen-induced maturation fails, the external female genitalia, uterus, and fallopian tubes develop normally.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 55
Correct
-
At what gestational age does the luteo-placental shift occur?
Your Answer: 6-8 weeks
Explanation:Luteo-placental shifts occurs around 6-8 week when the placenta takes over from the corpus luteum as the main producer of oestrogen and progesterone.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 56
Correct
-
A 23-year-old woman, G1PO comes to your clinic at 12 week of pregnancy. She is complaining of mild vaginal bleeding for the past 12 hours, along with bouts of mild cramping lower abdominal pain. On vaginal examination, the cervical os is closed with mild discharge containing blood clots and an ultrasonography confirms the presence of a live fetus with normal heart rate. Which among of the following is the most likely diagnosis?
Your Answer: Threatened abortion
Explanation:Uterine bleeding in the presence of a closed cervix along with sonographic visualization of an intrauterine pregnancy with detectable fetal cardiac activity are diagnostic of threatened abortion.
Abortion does not always follow a uterine bleeding in early pregnancy, sometimes not even after repeated episodes or large amounts of bleeding, that is why the term “threatened” is used in this case. In about 90 to 96% cases, the pregnancy continues after vaginal bleeding if occured in the presence of a closed os and a detectable fetal heart rate. Also as the gestational age advances its less likely the condition will end in miscarriage.
In cases of inevitable abortion, there will be dilatation of cervix along with progressive uterine bleeding and painful uterine contractions. The gestational tissue can be either felt or seen through the cervical os and the passage of this tissue occurs within a short time.
In case were the membranes have ruptured, partly expelling the products of conception with a significant amounts of placental tissue left in the uterus is called as incomplete abortion. During the late first and early second trimesters this will be the most common presentation of an abortion. Examination findings of this includes an open cervical os with gestational tissues observed in the cervix and a uterine size smaller than expected for gestational age and a partially contracted uterus. The amount of bleeding will vary but can be severe enough to cause hypovolemic shock, with painful contractions and an ultrasound revealing tissues in the uterus.
An in utero death of the embryo or fetus prior to 20 weeks of gestation is called as a missed abortion. In this case the women may notice that the symptoms associated with early pregnancy like nausea, breast tenderness, etc have disappeared and they don’t ‘feel pregnant’ anymore. Vaginal bleeding may occur but the cervix remains closed and the ultrasound done reveals an intrauterine gestational sac with or without an embryonic/fetal pole, but no embryonic/fetal cardiac activity will be noticed.
In case of complete abortion, miscarriage occurs before the 12th week and the entire contents of conception will be expelled out of uterus. If this case, the physical examination will show a small and well contracted uterus with an open or closed cervix. There is scant vaginal bleeding with only mild cramping and ultrasound will reveal an empty uterus without any extra-uterine pregnancy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 57
Incorrect
-
A 22-year-old nulliparous otherwise healthy woman presents with lower abdominal pain at 16 weeks of gestation. Her body temperature is 37.8 degrees Celsius. She appears to be in good health and is eating properly. Her uterus had been discovered to be retroverted but of normal size at her prior antenatal check at 11 weeks of pregnancy. Which of the following diagnoses is the most likely?
Your Answer: Impaction of a retroverted gravid uterus.
Correct Answer: Urinary tract infection.
Explanation:Lower abdominal pain can be caused by any of the conditions listed in the answers.
A urinary tract infection is the most likely cause.
Unless it was an abdominal ectopic or an interstitial pregnancy, an ectopic pregnancy.
will almost definitely have shown up before the 15th week of pregnancy.
A retroverted gravid uterus may impinge at 15 weeks of pregnancy, however, this is unlikely to be linked to a temperature of 37.8°C.
It’s also possible that it’s the source of acute urine retention.
Complications of the corpus luteum cyst normally manifest themselves considerably earlier in pregnancy, and severe appendicitis is far less likely to be the source of discomfort than a urinary tract infection. -
This question is part of the following fields:
- Obstetrics
-
-
Question 58
Correct
-
Which one of the following statements regarding Turner's syndrome is true?
Your Answer: Usually presents with primary amenorrhea
Explanation:Turner syndrome patients present with primary amenorrhea, have non functional or streak ovaries and cant conceive. They are 45X genetically.
-
This question is part of the following fields:
- Embryology
-
-
Question 59
Incorrect
-
The first stage of labour:
Your Answer: Effacement of the cervix
Correct Answer: Ends with fully dilation of the cervix
Explanation:First stage of the labour starts with the contractions of the uterus. With time, the no. of contractions, its duration and intensity increases. It ends once the cervix is fully dilated.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 60
Incorrect
-
A pregnant patient who is needle phobic has her nuchal translucency (NT) scan but refuses serum markers. You advise her the False Positive Rate of the scan is 5%. What would you advise the mother regarding the detection rate of Down Syndrome using NT alone?
Your Answer: 50%
Correct Answer: 70%
Explanation:The nuchal lucency measurement is the measure of the nuchal pad thickness. Children with down syndrome have an increased thickness of the nuchal pad. The risk of down’s syndrome increases with maternal age. The nuchal lucency test has an accuracy rate of 70%.
-
This question is part of the following fields:
- Genetics
-
-
Question 61
Correct
-
A 25-year old woman presented to the medical clinic for her first prenatal check-up. Upon interview, the patient revealed that she has been smoking one pack of cigarettes per day for the past five years. All of the following are considered correct regarding the disadvantages of smoking during pregnancy, except:
Your Answer: Increased risk of developing small teeth with faulty enamel
Explanation:Small teeth with faulty enamel is more associated with fetal alcohol syndrome (FAS).
In FAS, the most common orofacial changes are small eyelid fissures , flat facies, maxillary hypoplasia, short nose, long and hypoplastic nasal filter, and thin upper lip. The unique facial appearance of FAS patients is the result of changes in 4 areas: short palpebral fissures, flat nasal bridge with an upturned nasal tip, hypoplastic philtrum with a thin upper vermillion border, and a flat midface. Other facial anomalies include micrognathia, occasional cleft lip and/or palate and small teeth with defective enamel.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 62
Correct
-
A 35-year-old African female presents with a history of heavy menstrual bleeding and dysmenorrhoea for 4 months. Which of the following could be the most likely cause for this presentation?
Your Answer: Fibroid
Explanation:History of heavy menstrual bleeding and amenorrhoea favour the diagnosis of a fibroid uterus. All the given responses are causes for subfertility. Ectopic pregnancy presents with abdominal pain has an acute presentation. Endometriosis and adenomyosis usually don’t present with amenorrhoea or heavy bleeding respectively. PID presents with chronic pelvic pain and is not related to menstruation.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 63
Correct
-
Which increases the risk for developing endometrial cancer?
Your Answer: Early menarche
Explanation:Endometrioid endometrial carcinoma is oestrogen-responsive, and the main risk factor for this disease is long-term exposure to excess endogenous or exogenous oestrogen without adequate opposition by a progestin.
Early age at menarche is a risk factor for endometrial carcinoma in some studies; late menopause is less consistently associated with an increased risk of the disease. Both of these factors result in prolonged oestrogen stimulation and at times of the reproductive years during which anovulatory cycles are common
Other risk factors include
obesity,
nulliparity,
diabetes mellitus, and
hypertension.The risk of endometrial hyperplasia and carcinoma with oestrogen therapy can be significantly reduced by the concomitant administration of a progestin. In general, combined oestrogen-progestin preparations do not increase the risk of endometrial hyperplasia.
Endometrial carcinoma usually occurs in postmenopausal women (mean age at diagnosis is 62 years). Women under age 50 who develop endometrial cancer often have risk factors such as obesity or chronic anovulation.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 64
Correct
-
The following ultrasonic measurements may be used to confirm or establish gestational age:
Your Answer: Crown rump length
Explanation:Fetal ultrasound scanning is considered an essential part of routine antenatal care with first trimester scans recommended for confirming viability, accurate estimation of gestational age and determining the number of foetuses. Fetal crown-rump length (CRL) is measured in early pregnancy primarily to determine the gestation age (GA) of a foetus and is most reliable between 9+0 to 13+6 weeks’ gestation, but not beyond.
-
This question is part of the following fields:
- Physiology
-
-
Question 65
Correct
-
A patient is attending for medical abortion. She is 15 weeks gestation. She has no known drug allergies. Which of the following is the most appropriate regarding antibiotic prophylaxis?
Your Answer: Stat Azithromycin 1g and metronidazole 800 mg orally at time of abortion
Explanation:If the patient has a negative Chlamydia screen then a stat dose of metronidazole monotherapy is appropriate. You do not know this patients Chlamydia status and therefore dual therapy with metronidazole + doxycycline or azithromycin is appropriate.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 66
Incorrect
-
A 31-year-old woman at her 18th week of pregnancy presented to the emergency department with complaints of fishy, thin, white homogeneous vaginal discharge accompanied with an offensive odour. The presence of clue cells was noted during a microscopic test on the discharge. All of the following statements are considered false regarding her condition, except:
Your Answer: Partner should also be treated
Correct Answer: Relapse rate > 50 percent within 3 months
Explanation:Bacterial vaginosis (BV) affects women of reproductive age and can either be symptomatic or asymptomatic. Bacterial vaginosis is a condition caused by an overgrowth of normal vaginal flora. Most commonly, this presents clinically with increased vaginal discharge that has a fish-like odour. The discharge itself is typically thin and either grey or white.
Although bacterial vaginosis is not considered a sexually transmitted infection, women have an increased risk of acquiring other sexually transmitted infections (STI), and pregnant women have an increased risk of early delivery.
Though effective treatment options do exist, metronidazole or clindamycin, these methods have proven not to be effective long term.
BV recurrence rates are high, approximately 80% three months after effective treatment.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 67
Correct
-
A pregnant woman who is a heavy smoker, observed some thick white patches on the inside of her mouth. Her oral cavity appears inflamed on examination. Which diagnosis is most likely correct?
Your Answer: Candidiasis
Explanation:During pregnancy, the chances for a woman to develop oral candidiasis double. An aphthous ulcer has a yellowish floor which is surrounded by an erythematous halo while in lichen planus, the lesions do not have the appearance of a thick white mark but are more or less lace-like. The lesions in leucoplakia have raised edges and they appear as bright white patches which are sharply defined and cannot be rubbed out. Smoking may affect the tongue, producing tongue coating. In this case the tongue is just inflamed which is a sign of infection.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 68
Correct
-
What is the most common cause of sepsis in the puerperium?
Your Answer: Endometritis
Explanation:Significant puerperal pyrexia is defined as a temperature of 38ºC or higher on any two of the first 10 days postpartum, exclusive of the first 24 hours. A mixed flora normally colonizes the vagina with low virulence. Puerperal infection is usually polymicrobial and involves contaminants from the bowel that colonize the perineum and lower genital tract. Following delivery, natural barriers to infection are temporarily removed and therefore organisms with a pathogenic potential can ascend from the lower genital tract into the uterine cavity. Placental separation exposes a large raw area equivalent to an open wound, and retained products of conception and blood clots within the uterus can provide an excellent culture medium for infection.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 69
Incorrect
-
A diminishing blood volume within the first 4 hours post-partum may be seen when a warning sign occurs. Which of the following is considered the single most important warning sign for the said situation?
Your Answer: Decrease in blood pressure
Correct Answer: Tachycardia
Explanation:Postpartum haemorrhage (PPH) is a cumulative blood loss greater than 1000 mL with signs and symptoms of hypovolemia within 24 hours of the birth process, regardless of the route of delivery.
The first step in managing hemorrhagic shock is recognition. This should occur before the development of hypotension. Close attention should be paid to physiological responses to low blood volume. Tachycardia, tachypnoea, and narrowing pulse pressure may be the initial signs.
Tachycardia is typically the first abnormal vital sign of hemorrhagic shock. As the body attempts to preserve oxygen delivery to the brain and heart, blood is shunted away from extremities and nonvital organs. This causes cold and modelled extremities with delayed capillary refill. This shunting ultimately leads to worsening acidosis.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 70
Correct
-
A 30 year old women who is 24 weeks pregnant attends EPU due to suprapubic pain. Ultrasound shows a viable foetus and also a fibroid with a cystic fluid filled centre. What is the likely diagnosis?
Your Answer: Red degeneration of fibroid
Explanation:Red degeneration of fibroids is one of 4 methods of fibroid degeneration. Although uncommon outside pregnancy it is thought to be the most common form of fibroid degeneration during pregnancy and typically occurs in the 2nd trimester. It is thought to arise from the fibroid outgrowing its blood supply and haemorrhagic infarction occurs. Ultrasound will typically show a localised fluid collection (blood) within the fibroid.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 71
Incorrect
-
Galactorrhoea (non-gestational lactation) may result from all of the following EXCEPT:
Your Answer: Pituitary adenoma
Correct Answer: Intrapartum haemorrhage
Explanation:Pituitary tumours, the most common pathologic cause of galactorrhoea can result in hyperprolactinemia by producing prolactin or blocking the passage of dopamine from the hypothalamus to the pituitary gland. Approximately 30 percent of patients with chronic renal failure have elevated prolactin levels, possibly because of decreased renal clearance of prolactin. Primary hypothyroidism is a rare cause of galactorrhoea in children and adults. In patients with primary hypothyroidism, there is increased production of thyrotropin-releasing hormone, which may stimulate prolactin release. Nonpituitary malignancies, such as bronchogenic carcinoma, renal adenocarcinoma and Hodgkin’s and T-cell lymphomas, may also release prolactin.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 72
Correct
-
The arcuate line forms part of the border of the pelvic brim. Where is it located?
Your Answer: Ilium
Explanation:Arcuate means ‘bow shaped’ and there are different arcuate lines in anatomical terms. Regarding the pelvic brim this is composed of the arcuate line of the ilium, pectineal line and prominences of sacrum and pubic symphysis (as demonstrated in the images below). As can be seen the arcuate line is a smooth rounded border on the internal surface of the ilium inferior to the iliac fossa and Iliacus. Image sourced from Wikipedia Note: The pelvic outlet is also called the inferior aperture. The pelvic brim is the superior aperture
-
This question is part of the following fields:
- Anatomy
-
-
Question 73
Incorrect
-
Your Answer: HRT given to women with vasomotor symptoms, while they are still menstruating, is likely to increase the incidence of AD in the future.
Correct Answer: HRT given from the time of menopause at the age of approximately 50 years, reduces the decline of cognitive function, often seen as an early manifestation of AD.
Explanation:Although there have been some mixed results regarding the use of hormone replacement therapy (HRT) and the prevalence of Alzheimer’s disease (AD), there is little question that HRT started during menopause lowers cognitive decline, which is a common early symptom of AD.
This is in contrast to the effect shown when HRT is started at the age of 60-65, when the risk of Alzheimer’s disease rises.
There are no statistics on the effect of HRT on the incidence of Alzheimer’s disease when it is started before menopause, but it is apparent that it does not slow the progression of the disease or make advanced dementia less severe. -
This question is part of the following fields:
- Gynaecology
-
-
Question 74
Incorrect
-
Which of the following fasting plasma glucose (FPG) values for OGTT (Oral glucose tolerance test) is diagnostic of gestational diabetes according to the WHO criteria?
Your Answer: FPG 5.3mmol/L; 2 hour 8.6mmol/L
Correct Answer: FPG 6.1mmol/L; 2 hour 7.8mmol/L
Explanation:There are several criteria that aid in the diagnosis of gestational diabetes in pregnancy including NICE, WHO and modified WHO:
GDM Diagnostic Criteria:
NICE: Immediate FBG >5.6, 2 hour glucose >7.8
WHO: Immediate FBG >6.1, 2 hour glucose >7.8
Modified WHO: Immediate FBG >7.1, 2 hour glucose >7.8Random glucose and OGTT 2 hour readings of >11.1 are diagnostic of diabetes in non-pregnant states but are not part of the gestational diabetes criteria.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 75
Incorrect
-
A 26-year-old woman developed nausea and vomiting since 5th week of gestation, her symptoms started getting worsening over the last two weeks. On examination, she presents with signs of moderate degree of dehydration, along with a weight loss of approximately 10%. Urine dipstick examination is negative for both leukocytes and nitrites but is positive for ketones. Serum ketone level is elevated and other electrolytes including blood glucose levels are within normal range. Which of the below mentioned treatment options is not appropriate in this situation?
Your Answer: IV fluid resuscitation with Ringer’s lactate
Correct Answer: Encourage oral intake and discharge home
Explanation:Patient mentioned in the case has developed severe nausea and vomiting at the initial weeks of pregnancy. If the following clinical features are present, it confirms the diagnosis of hyperemesis gravidarum:
– Weight loss of more than 5% of pre-pregnancy weight
– Moderate to severe dehydration.
– Ketosis
– Electrolyte abnormalities.Management of hyperemesis gravidarum include:
– Temporary suspension of oral intake, followed by gradual resumption.
– Intravenous fluid resuscitation, beginning with 2 L of Ringer’s lactate infused over 3 hours to maintain a urine output of more than 100 mL/h.
– Use of Antiemetics like metoclopramide, if needed.
– Oral administration of Vitamin B6.
– Replacement of electrolytes if required in the case.Encouraging oral intake and sending this patient home without any intravenous hydration, is not considered the correct treatment option in this case.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 76
Incorrect
-
You are called to see a 24 year old patient in A&E. She is 34 weeks gestation and her blood pressure is 149/98. Urine dip shows protein 3+. You send a for a protein:creatinine ratio. What level would be diagnostic of significant proteinuria?
Your Answer: >130 mg/mmol
Correct Answer: >30 mg/mmol
Explanation:Significant proteinuria = urinary protein:creatinine ratio >30 mg/mmol or 24-hour urine collection result shows greater than 300 mg protein
-
This question is part of the following fields:
- Clinical Management
-
-
Question 77
Incorrect
-
A 29-year-old single lady comes to your clinic with two days history of minor left-sided lower abdomen ache. Her blood pressure is 125/90 mmHg, her pulse rate is 90 beats per minute, and her temperature is 37.3°C. She is otherwise in perfect health. There is no discomfort, rebound, or guarding on the abdominal exam. On the left side of the uterus, an ultrasonographic examination reveals a 6cm solid mass lateral to the uterus. Which of the following diagnoses is the most likely?
Your Answer: Corpus luteal cyst
Correct Answer: Ovarian teratoma
Explanation:Mature cystic teratomas of the ovary are often discovered as incidental findings on physical examination, during radiographic studies, or during abdominal surgery performed for other indications.
When symptoms are present, they may include abdominal pain, mass or swelling, and abnormal uterine bleeding. Bladder symptoms, gastrointestinal disturbances, and back pain are less frequent. When abdominal pain is present, it usually is constant and ranges from slight to moderate in intensity.
Mucinous cystadenomas are relatively common (12% to 15% of all ovarian tumours). They can become massive. These tumours usually develop in the third to fifth decades of life and typically cause vague symptoms, such as increasing abdominal girth, abdominal or pelvic pain, emesis, fatigue, indigestion, constipation, and urinary incontinence.
Corpus luteal cysts present with irregular menses, abdominal fullness due to fluid build up and pelvic pressure.
Endometriosis mainly presents with cyclic pain at site of involvement and dysmenorrhea.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 78
Incorrect
-
You diagnose Erb-Duchenne palsy in a baby born with shoulder dystocia who suffered a brachial plexus injury. Which of the following nerve roots are likely to be affected?
Your Answer: C3 and C4
Correct Answer: C5 and C6
Explanation:Shoulder dystocia occurs when the fetal shoulder impacts on the maternal symphysis or sacrum during vaginal delivery. About 10% of babies with shoulder dystocia will suffer a brachial plexus injury, the most common one being Erb-Duchenne palsy. In Erb’s palsy, the upper nerve roots C5 and C6 are damaged due to excessive widening of the angle between the head and the shoulder. This causing temporary paralysis in the affected arm whereby the infant will present with its hand hanging limp by his side, internal rotation of the forearm, plus wrist and finger flexion. This sign is called the ‘waiter’s tip hand’. The palsy usually resolves spontaneously in a large proportion of cases.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 79
Incorrect
-
A 24 year old patient decides to take a Chlamydia screening test whilst in the GP surgery. He is asymptomatic. The results are positive for chlamydia infection. His partner attends for testing and wants to know the risk of contracting Chlamydia. What is the risk of chlamydia infection following intercourse with an asymptomatic chlamydia positive partner?
Your Answer: 25%
Correct Answer: 65%
Explanation:The chances of transmitting chlamydia from an asymptomatic partner through sexual intercourse is 65%.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 80
Incorrect
-
A 29-year-old pregnant woman, at 26 weeks of gestation, is involved in a car accident while wearing a seatbelt. On examination there are visible bruises on the abdomen but patient is otherwise normal. Fetal heart sounds are audible and are within normal parameters and CTG is reassuring. Which of the following will be the best next step in management of this case?
Your Answer: Observe for six hours and discharge home
Correct Answer: Admit her and observe for 24 hours
Explanation:Trauma is a major contributor for maternal mortality and is one of the leading causes of pregnancy-associated maternal deaths.
As a result of maternal hypotension or hypoxemia, placental abruption, uterine rupture or fetal trauma a maternal trauma can compromise the fetus also.
Patient’s bruises on the abdomen which are seatbelt marks, are indications that this woman has positioned the seat belt incorrectly over the uterus. So there is a good chance that the uterus and its contents, including the fetus, has been affected by the impact. In a pregnant woman, the correct position of seat belt is when the lap belt is placed on the hip below uterus and the sash is placed between breasts and above the uterus.A minimum of 24-hour period monitoring is recommended for all pregnant women, apart from the routine trauma workup indicated in non-pregnant women, in case they have sustained trauma in the presence of any of the following:
– Regular uterine contractions
– Vaginal bleeding
– A non-reassuring fetal heart rate tracing
– Abdominal/uterine pain
– Significant trauma to the abdomenConsidering the bruises over her abdomen this patient should be considered as having significant abdominal trauma and must be kept under observation for a minimum of 24 hours. Such patients should not be discharged unless the clinician makes sure they do not have any complications like abruption or preterm labor.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 81
Incorrect
-
The ovaries produce androgen and progesterone. What is the common precursor for both of these hormones?
Your Answer: Inhibin A
Correct Answer: Cholesterol
Explanation:Both the female hormones, namely progesterone and oestrogen as well as the male hormones or androgens are lipid soluble. The common precursor of these is cholesterol.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 82
Incorrect
-
Question 83
Incorrect
-
What is the Gold standard investigation to diagnose abnormal uterine bleeding?
Your Answer: Transabdominal ultrasound
Correct Answer: Hysteroscopy along with dilatation and curettage
Explanation:During the last decade hysteroscopy has become the tool of choice for the evaluation of the endometrial cavity, including for assessment of abnormal uterine bleeding (AUB). Many clinicians would consider that, in most patients, the combination of transvaginal sonography and out-patient endometrial biopsy with diagnostic hysteroscopy could replace the need for dilation and curettage. Hysteroscopy was reported to have sensitivity, specificity, negative predictive value and positive predictive value of 94.2, 88.8, 96.3 and 83.1% respectively, in predicting normal or abnormal endometrial histopathology.
The highest accuracy of hysteroscopy was in diagnosing endometrial polyps, whereas the worst result was in estimating hyperplasia. Therefore, since the incidence of focal lesions in patients with AUB is high, it seems that the most beneficial approach is to proceed with hysteroscopy complemented by endometrial biopsy early in the assessment of AUB.
Transabdominal and transvaginal ultrasounds can be used but are inferior to hysteroscopy.
Coagulation profile can only diagnose possible coagulopathies and pregnancy test can only diagnose pregnancy. All other causes can not be identified with these laboratory investigations.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 84
Incorrect
-
What is the average volume of blood loss during the menstrual cycle?
Your Answer: 80-85ml
Correct Answer: 35-40ml
Explanation:Normal menstrual blood loss is about 40-45 ml. More than 80 ml per period is defined as heavy menstrual bleeding.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 85
Incorrect
-
A 19-year-old girl, with menarche at age 12, presents with a 2-year duration of severe dysmenorrhea. Analgesia with paracetamol, panadeine as well as indomethacin did not provide much relief. The girl is very concerned that the underlying cause could be something sinister. What is the most likely cause of her dysmenorrhea?
Your Answer: An endometrial polyp.
Correct Answer: Endometrial prostaglandin release.
Explanation:It is less common for a girl of this age to develop fibroids, endometriosis and endometrial polyps, although these are all causes of severe dysmenorrhea. Chronic pelvic infection can be due to sexually transmitted disease but the history does not mention any previous episodes of pelvic pain or symptoms of infection such as fever. In this case, it is most likely that she has primary dysmenorrhea. Primary dysmenorrhea, in which no pathological cause can be identified, is believed to be due to the prostaglandins released by the secretory endometrium. If secondary dysmenorrhea is suspected, then endometriosis would be the most prominent cause.
While hysteroscopic and laparoscopic examinations are commonly done in adult women to rule out organic causes such as those mentioned earlier, in younger girls, they are usually only carried out if pain management with, for example, NSAIDs and the use of COCPs, have failed to either provide symptom relief or reduction.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 86
Incorrect
-
All of the following statements is considered incorrect regarding the management of deep vein thrombosis in pregnancy, except:
Your Answer: Warfarin therapy is contraindicated only in the first trimester of pregnancy
Correct Answer: Warfarin therapy is contraindicated throughout pregnancy but safe during breast feeding
Explanation:Anticoagulant therapy is the standard treatment for deep vein thrombosis (DVT) but is mostly used in non-pregnant patients. In pregnancy, unfractionated heparin (UFH) and low molecular weight heparin (LMWH) are commonly used. Warfarin therapy is generally avoided in pregnancy because of its fetal toxicity.
Warfarin is contraindicated during pregnancy, but is safe to use postpartum and is compatible with breastfeeding. Low-molecular-weight heparin has largely replaced unfractionated heparin for prophylaxis and treatment in pregnancy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 87
Incorrect
-
Question 88
Correct
-
Which one of the following is true regarding routine prenatal screening ultrasonography before 24 weeks gestation?
Your Answer: It has not been proven to have any significant benefits
Explanation:Routine ultrasonography at around 18-22 weeks gestation has become the standard of care in many communities. Acceptance is based on many factors, including patient preference, medical-legal pressure, and the perceived benefit by physicians. However, rigorous testing has found little scientific benefit for, or harm from, routine screening ultrasonography.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 89
Incorrect
-
Which of the following arteries branches directly from the aorta?
Your Answer: Vaginal
Correct Answer: Ovarian
Explanation:The uterine and vaginal arteries branch from the internal iliac artery. The ovarian artery branches direct from the aorta.
-
This question is part of the following fields:
- Anatomy
-
-
Question 90
Correct
-
A patient has had limited response to conservative measures for her overactive bladder (OAB). Which of the following is the most appropriate pharmacological choice?
Your Answer: Darifenacin
Explanation:Detrusor overactivity can be treated with anti-cholinergic agents such as oxybutynin or tolterodine, solifenacin, fesoterodine and darifenacin. They are used as first line agents. Imipramine is used for enuresis and desmopressin is used for nocturia.
NICE pathwayPrior to initiating anticholinergics:
Bladder training
Consider treating vaginal atrophy and nocturia with topical oestrogen and desmopressin respectively before commencing treatments below.
Consider catheterisation if chronic retention
1st line treatments:
1. Oxybutynin (immediate release) – Do not offer to frail elderly patients
2. Tolterodine (immediate release)
3. Darifenacin (once daily preparation)
DO NOT offer any of the 3 drugs below:
1. Flavoxate
2. Propantheline
3. Imipramine
2nd line treatment
Consider transdermal anticholinergic (antimuscarinic)
Mirabegron
Adjuvant Treatments
Desmopressin can be considered for those with nocturia
Duloxetine may be considered for those who don’t want/unsuitable for surgical treatment
Intravaginal oestrogen can be offered to postmenopausal women with OAB -
This question is part of the following fields:
- Clinical Management
-
-
Question 91
Incorrect
-
A 55 year old patient with a who has tried unsuccessful conservative measures for her overactive bladder, would like to consider Oxybutynin. She wants to know how common dry mouth is as a side effect, as her sister suffered from it on while on the same drug.
Your Answer: approximately 1 in 1000 patients
Correct Answer: approximately 1 in 10 patients
Explanation:Urinary incontinence can be divided into two main aetiologies, stress incontinence, or overactive bladder. Conservative management include lifestyle interventions, controlling fluid intake, or bladder exercises. If conservative management is no longer efficient, then medications may be indicated. Oxybutynin is an anticholinergic drug used in the treatment of urinary incontinence. As with other anticholinergic drugs, side effects include dry mouth, dry eyes, blurry vision and constipation. About 1 in 10 patients taking Oxybutynin will experience some of these side effects.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 92
Incorrect
-
Which one of the following features indicates complete placental separation after delivery?
Your Answer: Changes of uterine shape from discoid to globular
Correct Answer: All of the options given
Explanation:At the time of delivery, the most important signs of complete placental separation are lengthening of the umbilical cord, per vaginal bleeding and change in shape of uterus from discoid to globular shape. The uterus contracts in size and rises upward.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 93
Incorrect
-
Which of the following amniotic fluid indexes define oligohydramnios?
Your Answer: < 8 mm
Correct Answer:
Explanation:An assessment of amniotic fluid in pregnancy can be done by taking ultrasound measurements of the depth of amniotic fluid pockets. The combination of the measurements in four quadrants is called the amniotic fluid index (AFI), one of the major determinants of the biophysical profile which predicts pregnancy outcome. An AFI of less than 5 cm, or less than the 5th percentile is defined as oligohydramnios while an AFI of more than 25 cm is considered polyhydramnios.
-
This question is part of the following fields:
- Biophysics
-
-
Question 94
Incorrect
-
Renal cell carcinoma is associated with which type of metastasis?
Your Answer: Transplantation
Correct Answer: Haematogenous
Explanation:Most carcinomas spread primarily via lymphatic invasion. Renal cell is the exception spreading via the bloodstream.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 95
Incorrect
-
A 45 year old women has a transvaginal ultrasound that is reported as showing a partially echogenic mass with posterior sound attenuation owing to sebaceous material and hair within the cyst cavity. What is the likely diagnosis?
Your Answer: Functional cyst
Correct Answer: Mature teratoma
Explanation:Dermoid cysts and teratomas contain elements from multiple germ cell layers. They are often considered the same entity (even in medical texts) however a dermoid is composed only of dermal and epidermal elements. A teratoma has mesodermal and endodermal elements Mature teratomas are composed of well-differentiated derivations from at least 2/3 germ cell layers (i.e. ectoderm, mesoderm, and endoderm). They contain developmentally mature skin complete with hair follicles, sweat glands, sometimes hair, and sometimes sebum, blood, fat, bone, nails, teeth, eyes, cartilage, and thyroid tissue.
-
This question is part of the following fields:
- Data Interpretation
-
-
Question 96
Incorrect
-
A 56 year old lady presents with a vulval itch and discolouration. A biopsy conforms Lichen Sclerosis (LS). What is the risk of developing squamous cell carcinoma compared to patients with a normal vulval biopsy?
Your Answer: 100% - histological features confirm SCC
Correct Answer:
Explanation:Lichen Sclerosis is a destructive inflammatory condition that effects the anogenital region of women. It effects around 1 in 300 women. It destroys the subdermal layers of the skin resulting in hyalinization of the skin leading to parchment paper appearance of the skin. It is associated with vulval cancer and it is estimated that the risk of developing vulval cancer after lichen sclerosis is around 3-5%.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 97
Incorrect
-
A 52-year-old lady comes to your office with vaginal bleeding 7 hours after sexual intercourse. She hasn't had a menstrual period in over a year. A year ago, she had a normal pap smear. She has no other symptoms and appears to be in good condition. Which of the following is the most likely underlying cause of this woman's postcoital bleeding?
Your Answer: Cervical ectropion
Correct Answer: Vaginal atrophy
Explanation:Vaginal atrophy (thinning of vaginal tissue): Oestrogen helps to keep this tissue healthy. After menopause, low oestrogen levels can cause your vaginal walls to become thin, dry, and inflamed. That often leads to bleeding after sex.
Vaginal atrophy is the most common cause of post menopausal vaginal bleeding.
With a normal pap smear a year ago, this patient is unlikely to develop cervical cancer.
Cervical ectropions are not common in post-menopausal women.
Endometrial cancer and cervical polyps are possible causes of postcoital bleeding, however, they are not as common as vaginal atrophy.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 98
Incorrect
-
What is the definition of premature menopause?
Your Answer: Menopause at or before 45 years of age
Correct Answer: Menopause at or before 40 years of age
Explanation:Menopause is defined as the cessation of menstruation for a period of 12 months. Premature menopause is defined as cessation of menstruation before the age of 40.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 99
Incorrect
-
Question 100
Incorrect
-
A 27-year-old woman complains of a hard, irregular lump in her right breast that presented after a car accident 2 weeks ago. Which is the most likely diagnosis?
Your Answer:
Correct Answer:
Explanation:Since the car crash happened two weeks prior, breast trauma is suggested and thus fat necrosis is the most probable diagnosis. Phyllodes tumours are typically a firm, palpable mass. These tumours are very fast-growing, and can increase in size in just a few weeks. Occurrence is most common between the ages of 40 and 50, prior to menopause.
-
This question is part of the following fields:
- Gynaecology
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Mins)