-
Question 1
Incorrect
-
A 60-year-old man with a long history of diabetes arrives at the emergency department complaining of excruciating pain around his 'rear end', inability to defecate due to the pain, and spiking temperatures. During the examination, the patient is unable to tolerate an anal examination, but the anus appears red and inflamed. What is the most probable cause of this man's symptoms?
Your Answer: Anal fissure
Correct Answer: Perianal abscess
Explanation:Understanding Perianal Abscesses
A perianal abscess is a type of anorectal abscess that occurs when pus collects within the subcutaneous tissue surrounding the anal sphincter. It is the most common form of anorectal abscess, accounting for around 60% of cases, and is more prevalent in men with an average age of 40 years. Symptoms include pain around the anus, hardened tissue in the anal region, and pus-like discharge from the anus. In some cases, patients may also experience systemic infection.
Perianal abscesses are typically caused by gut flora such as E. coli, although those caused by Staph. aureus are more likely to be a skin infection. Diagnosis can be made through inspection of the anus and digital rectal examination, with further investigations such as colonoscopy and blood tests used to determine underlying causes. Imaging such as MRI and transperineal ultrasound may also be used in complicated cases.
Treatment for perianal abscesses involves surgical incision and drainage under local anaesthetic, with the wound either packed or left open to heal over several weeks. Antibiotics may be used in cases of systemic infection, but are not typically used for wound healing. It is important to note that perianal abscesses are just one type of anorectal abscess, with others classified by the layers and planes they occupy, such as ischiorectal, supralevator, intersphincteric, and horseshoe abscesses.
Overall, understanding perianal abscesses and their causes, symptoms, and treatment options is important for proper diagnosis and management of this common condition.
-
This question is part of the following fields:
- Surgery
-
-
Question 2
Incorrect
-
A 29-year-old male presents to the Emergency Department following a head injury sustained during a soccer game. The patient reports a loss of consciousness for about 10 seconds at the time of injury. What would be a clear indication to perform a CT scan of the head?
Your Answer:
Correct Answer: A past medical history of Von Willebrand disease
Explanation:When deciding if a CT head is necessary for a patient with a head injury, clinical judgement should be utilized. If the patient has coagulopathy and has experienced some loss of consciousness or amnesia, according to the NICE head injury guidelines, a CT head should be conducted within 8 hours. This is because Von Willebrand disease is a type of coagulopathy.
NICE Guidelines for Investigating Head Injuries in Adults
Head injuries can be serious and require prompt medical attention. The National Institute for Health and Care Excellence (NICE) has provided clear guidelines for healthcare professionals to determine which adult patients need further investigation with a CT head scan. Patients who require immediate CT head scans include those with a Glasgow Coma Scale (GCS) score of less than 13 on initial assessment, suspected open or depressed skull fractures, signs of basal skull fractures, post-traumatic seizures, focal neurological deficits, and more than one episode of vomiting.
For patients with any loss of consciousness or amnesia since the injury, a CT head scan within 8 hours is recommended for those who are 65 years or older, have a history of bleeding or clotting disorders, experienced a dangerous mechanism of injury, or have more than 30 minutes of retrograde amnesia of events immediately before the head injury. Additionally, patients on warfarin who have sustained a head injury without other indications for a CT head scan should also receive a scan within 8 hours of the injury.
It is important for healthcare professionals to follow these guidelines to ensure that patients receive appropriate and timely care for their head injuries. By identifying those who require further investigation, healthcare professionals can provide the necessary treatment and support to prevent further complications and improve patient outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 3
Incorrect
-
A 42-year-old man presents to the emergency department with persistent vomiting. He reports feeling very bloated for the past week, experiencing cramping abdominal pain and discomfort. This morning he began to feel very nauseous and has been vomiting small amounts of green liquid for the past few hours. The patient has a history of laparoscopic appendectomy for appendicitis at the age of 37.
What investigation would be most suitable to confirm the probable underlying diagnosis?Your Answer:
Correct Answer: CT abdomen
Explanation:The most appropriate diagnostic investigation for small bowel obstruction is CT abdomen, according to NICE guidelines. This is because it is highly sensitive and can distinguish between mechanical obstruction and pseudo-obstruction. In this case, the obstruction was likely caused by adhesions from previous surgery. Symptoms of small bowel obstruction include abdominal pain, distension, nausea, vomiting, constipation, and potential perforation. Abdominal X-rays are not as useful as CT abdomen and may require additional imaging, exposing the patient to unnecessary radiation. Abdominal ultrasound scan is not used for bowel obstruction. Blood tests, including CEA tumour marker, are not relevant in this case as there is no indication of bowel cancer. Bowel cancer typically presents in older patients with symptoms such as blood in stools, weight loss, and signs of anaemia.
Small bowel obstruction occurs when the small intestines are blocked, preventing the passage of food, fluids, and gas. The most common cause of this condition is adhesions, which can develop after previous surgeries, followed by hernias. Symptoms of small bowel obstruction include diffuse, central abdominal pain, nausea and vomiting (often bilious), constipation, and abdominal distension. Tinkling bowel sounds may also be present in early stages of obstruction. Abdominal x-ray is typically the first-line imaging for suspected small bowel obstruction, showing distended small bowel loops with fluid levels. CT is more sensitive and considered the definitive investigation, particularly in early obstruction. Management involves initial steps such as NBM, IV fluids, and nasogastric tube with free drainage. Some patients may respond to conservative management, but others may require surgery.
-
This question is part of the following fields:
- Surgery
-
-
Question 4
Incorrect
-
You are asked to assess a 35-year-old male who is currently recuperating after experiencing a subarachnoid haemorrhage (SAH) three days ago. The patient has reported feeling more lethargic and nauseous today, and has developed a new headache and muscle cramps. Upon conducting a physical examination, no abnormalities were detected.
What is the probable diagnosis?Your Answer:
Correct Answer: Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
Explanation:SIADH is frequently seen as a result of subarachnoid hemorrhage, which is a type of brain injury. This condition causes the body to produce too much antidiuretic hormone, leading to low sodium levels and symptoms such as headaches, nausea, vomiting, muscle cramps, and decreased consciousness. While adrenal crisis can also cause hyponatremia and similar symptoms, it typically presents with additional clinical signs like hyperpigmentation. Cerebral herniation, which can occur after SAH due to increased intracranial pressure, would be expected to cause reduced consciousness and abnormal physical exam findings. Encephalitis, a rare condition characterized by brain swelling often caused by viral infection, is not commonly associated with SAH and typically presents with flu-like symptoms followed by confusion, behavioral changes, and hallucinations.
A subarachnoid haemorrhage (SAH) is a type of bleeding that occurs within the subarachnoid space of the meninges in the brain. It can be caused by head injury or occur spontaneously. Spontaneous SAH is often caused by an intracranial aneurysm, which accounts for around 85% of cases. Other causes include arteriovenous malformation, pituitary apoplexy, and mycotic aneurysms. The classic symptoms of SAH include a sudden and severe headache, nausea and vomiting, meningism, coma, seizures, and ECG changes.
The first-line investigation for SAH is a non-contrast CT head, which can detect acute blood in the basal cisterns, sulci, and ventricular system. If the CT is normal within 6 hours of symptom onset, a lumbar puncture is not recommended. However, if the CT is normal after 6 hours, a lumbar puncture should be performed at least 12 hours after symptom onset to check for xanthochromia and other CSF findings consistent with SAH. If SAH is confirmed, referral to neurosurgery is necessary to identify the underlying cause and provide urgent treatment.
Management of aneurysmal SAH involves supportive care, such as bed rest, analgesia, and venous thromboembolism prophylaxis. Vasospasm is prevented with oral nimodipine, and intracranial aneurysms require prompt intervention to prevent rebleeding. Most aneurysms are treated with a coil by interventional neuroradiologists, but some require a craniotomy and clipping by a neurosurgeon. Complications of aneurysmal SAH include re-bleeding, hydrocephalus, vasospasm, and hyponatraemia. Predictive factors for SAH include conscious level on admission, age, and amount of blood visible on CT head.
-
This question is part of the following fields:
- Surgery
-
-
Question 5
Incorrect
-
A 28-year-old male has come for his pre-operative assessment before his tonsillectomy due to recurrent tonsillitis. During the assessment, the anaesthetist asks about his family history and he reveals that his father and paternal grandfather both had malignant hyperthermia after receiving general anaesthesia. However, his mother and paternal grandmother have never had any adverse reactions to general anaesthesia. What is the likelihood of this patient experiencing a similar reaction after receiving general anaesthesia?
Your Answer:
Correct Answer: 50%
Explanation:Malignant Hyperthermia: A Condition Triggered by Anaesthetic Agents
Malignant hyperthermia is a medical condition that often occurs after the administration of anaesthetic agents. It is characterized by hyperpyrexia and muscle rigidity, which is caused by the excessive release of calcium ions from the sarcoplasmic reticulum of skeletal muscle. This condition is associated with defects in a gene on chromosome 19 that encodes the ryanodine receptor, which controls calcium release from the sarcoplasmic reticulum. Susceptibility to malignant hyperthermia is inherited in an autosomal dominant fashion. It is worth noting that neuroleptic malignant syndrome may have a similar aetiology.
The causative agents of malignant hyperthermia include halothane, suxamethonium, and other drugs such as antipsychotics (which can trigger neuroleptic malignant syndrome). To diagnose this condition, doctors may perform tests such as checking for elevated levels of creatine kinase and conducting contracture tests with halothane and caffeine.
The management of malignant hyperthermia involves the use of dantrolene, which prevents the release of calcium ions from the sarcoplasmic reticulum. With prompt and appropriate treatment, patients with malignant hyperthermia can recover fully. Therefore, it is essential to be aware of the risk factors and symptoms of this condition, especially when administering anaesthetic agents.
-
This question is part of the following fields:
- Surgery
-
-
Question 6
Incorrect
-
A 39-year-old patient with a history of peripheral vascular disease presents to the emergency department with complaints of rest pain in their left leg. Despite being a smoker, their BMI is 25 kg/m² and they have no other medical issues. Upon examination, the patient has absent foot pulses and lower limb pallor. A CT angiogram is performed and reveals a long segmental obstruction, leading to suspicion of critical limb ischaemia. What is the best course of treatment?
Your Answer:
Correct Answer: Open bypass graft
Explanation:Open surgical revascularization is more appropriate for low-risk patients with long-segment/multifocal lesions who have peripheral arterial disease with critical limb ischaemia.
Peripheral arterial disease (PAD) is a condition that is strongly associated with smoking. Therefore, patients who still smoke should be provided with assistance to quit smoking. It is also important to treat any comorbidities that the patient may have, such as hypertension, diabetes mellitus, and obesity. All patients with established cardiovascular disease, including PAD, should be taking a statin, with Atorvastatin 80 mg being the recommended dosage. In 2010, NICE published guidance recommending the use of clopidogrel as the first-line treatment for PAD patients instead of aspirin. Exercise training has also been shown to have significant benefits, and NICE recommends a supervised exercise program for all PAD patients before other interventions.
For severe PAD or critical limb ischaemia, there are several treatment options available. Endovascular revascularization and percutaneous transluminal angioplasty with or without stent placement are typically used for short segment stenosis, aortic iliac disease, and high-risk patients. On the other hand, surgical revascularization, surgical bypass with an autologous vein or prosthetic material, and endarterectomy are typically used for long segment lesions, multifocal lesions, lesions of the common femoral artery, and purely infrapopliteal disease. Amputation should only be considered for patients with critical limb ischaemia who are not suitable for other interventions such as angioplasty or bypass surgery.
There are also drugs licensed for use in PAD, including naftidrofuryl oxalate, a vasodilator sometimes used for patients with a poor quality of life. Cilostazol, a phosphodiesterase III inhibitor with both antiplatelet and vasodilator effects, is not recommended by NICE.
-
This question is part of the following fields:
- Surgery
-
-
Question 7
Incorrect
-
A 25-year-old woman presents to her GP with a lump on her left breast. She has no family history of breast cancer. Upon examination, a smooth, rubbery, mobile mass measuring 4 cm in diameter with clearly defined edges is found. An ultrasound of her breasts reveals a single round solid mass of 4 cm diameter, which is well circumscribed and lobulated. Core biopsy confirms the presence of epithelial and stromal elements consistent with a fibroadenoma. The lump is causing her moderate discomfort and she expresses a desire to have it removed. What is the most appropriate advice to give this patient?
A) The lump will regress by itself so no need to remove.
B) The lump is non-cancerous and hence cannot be removed, but she should return if it changes or grows.
C) Refer her for excision biopsy to remove the mass.
D) Prescribe her ibuprofen for the pain, and advise her that she does not require removal of the lump.
E) Refer her for a breast mammogram to assess the lump.
Explanation:
As the lump has examination, ultrasound, and histological findings consistent with a fibroadenoma and is causing moderate discomfort, surgical excision should be recommended. It is important to obtain histological evidence to confirm the diagnosis of fibroadenoma if excision is required. Observation and simple advice would be sufficient if the fibroadenoma were less than 3 cm, but the size and discomfort of this lump make that option incorrect. A breast mammogram is usually ineffective for a younger woman due to dense breasts. Prescribing ibuprofen is generally the treatment for fibroadenosis, which is a different condition where women experience painful breasts generally around their periods. It would not be a solution for the discomfort caused by the mass effect of the fibroadenoma.Your Answer:
Correct Answer: Refer her for excision biopsy to remove the mass
Explanation:Surgical excision is the recommended course of action for a breast fibroadenoma that is over 3 cm in size and causing moderate discomfort, based on examination, ultrasound, and histological findings. It is important to confirm the diagnosis of fibroadenoma through histological evidence before proceeding with excision. While some fibroadenomas may disappear without treatment, this is not the case for larger ones causing discomfort. Observation and simple advice are only appropriate for fibroadenomas that are less than 3 cm in size. A breast mammogram is generally not effective for younger women with dense breasts. Prescribing ibuprofen is not a solution for the discomfort caused by the fibroadenoma, as this is a different condition from fibroadenosis, which causes painful breasts around the time of menstruation.
Understanding Breast Fibroadenoma
Breast fibroadenoma is a type of breast mass that develops from a whole lobule. It is characterized by a mobile, firm, and smooth lump in the breast, which is often referred to as a breast mouse. Fibroadenoma accounts for about 12% of all breast masses and is more common in women under the age of 30.
Fortunately, fibroadenomas are usually benign and do not increase the risk of developing breast cancer. In fact, over a two-year period, up to 30% of fibroadenomas may even get smaller on their own. However, if the lump is larger than 3 cm, surgical excision is typically recommended.
In summary, breast fibroadenoma is a common type of breast mass that is usually benign and does not increase the risk of breast cancer. While it may cause concern for some women, it is important to remember that most fibroadenomas do not require treatment and may even resolve on their own.
-
This question is part of the following fields:
- Surgery
-
-
Question 8
Incorrect
-
An 80-year-old man is scheduled for a surgery to remove a cancerous growth in his large intestine. He has been noticing a gradual decrease in weight and alteration in bowel movements for the past two months. A recent colonoscopy has revealed a mass in the lower part of his descending colon. Despite his age, he appears to be in good health and is prepared to proceed with the procedure. What is the most probable surgery he will undergo?
Your Answer:
Correct Answer: Left hemicolectomy
Explanation:The appropriate surgical procedure for a patient with distal transverse or descending colon cancer is a left hemicolectomy. This procedure involves removing the distal two-thirds of the transverse colon, the descending colon, and the sigmoid colon. The rectum is left intact and anastomosed with the proximal transverse colon, avoiding the need for a permanent stoma.
Other surgical options, such as Hartmann’s procedure, high anterior resection, low anterior resection, and right hemicolectomy, are not suitable for this patient’s condition. Hartmann’s procedure is reserved for emergencies, while high anterior resection and low anterior resection are used for rectal tumors. Right hemicolectomy is performed for cancers in the cecum, ascending colon, or proximal third of the transverse colon.
Colorectal cancer is typically diagnosed through CT scans and colonoscopies or CT colonography. Patients with tumors below the peritoneal reflection should also undergo MRI to evaluate their mesorectum. Once staging is complete, a treatment plan is formulated by a dedicated colorectal MDT meeting.
For colon cancer, surgery is the primary treatment option, with resectional surgery being the only cure. The procedure is tailored to the patient and tumor location, with lymphatic chains being resected based on arterial supply. Anastomosis is the preferred method of restoring continuity, but in some cases, an end stoma may be necessary. Chemotherapy is often offered to patients with risk factors for disease recurrence.
Rectal cancer management differs from colon cancer due to the rectum’s anatomical location. Tumors can be surgically resected with either an anterior resection or an abdominoperineal excision of rectum (APER). A meticulous dissection of the mesorectal fat and lymph nodes is integral to the procedure. Neoadjuvant radiotherapy is often offered to patients prior to resectional surgery, and those with obstructing rectal cancer should have a defunctioning loop colostomy.
Segmental resections based on blood supply and lymphatic drainage are the primary operations for cancer. The type of resection and anastomosis depend on the site of cancer. In emergency situations where the bowel has perforated, an end colostomy is often safer. Left-sided resections are more risky, but ileocolic anastomoses are relatively safe even in the emergency setting and do not need to be defunctioned.
-
This question is part of the following fields:
- Surgery
-
-
Question 9
Incorrect
-
A 62-year-old man presents to the pre-admission clinic for assessment prior to an elective prostatectomy. You find no adverse past medical history and examination is unremarkable. An electrocardiogram (ECG) is indicated in all pre-operative patients undergoing major surgery who are over the age of 60. The ECG is shown below.
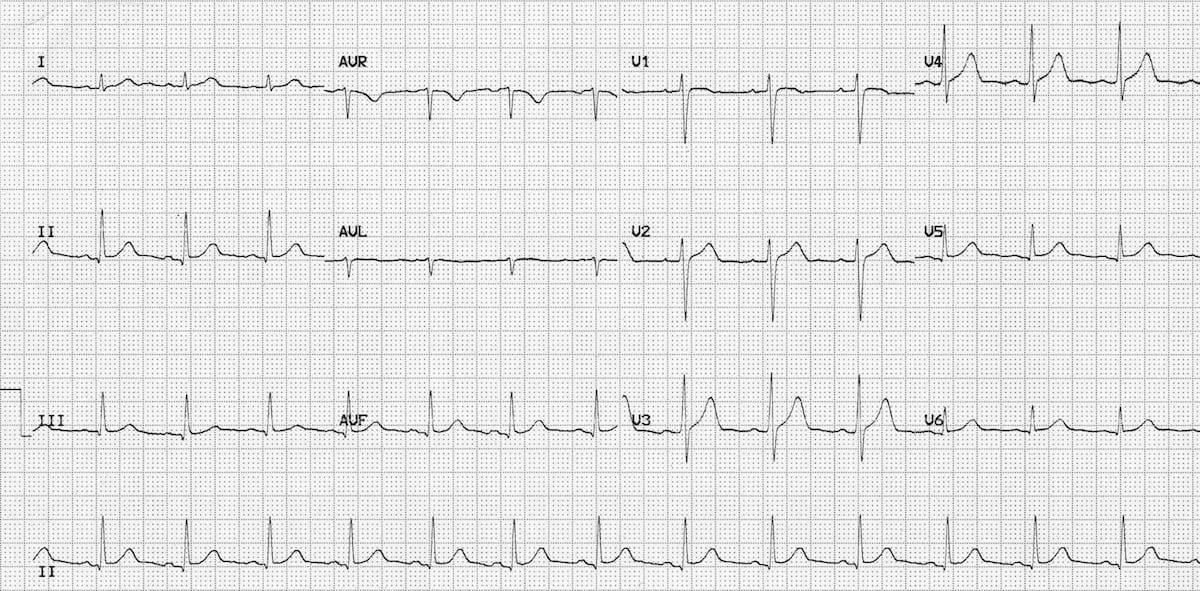 After having reviewed the ECG, what is the next best step to take with this patient?
After having reviewed the ECG, what is the next best step to take with this patient? Your Answer:
Correct Answer: No further assessment is required
Explanation:Assessing Cardiac Risk in Preoperative Patients: Common Misconceptions
There are several misconceptions when it comes to assessing cardiac risk in preoperative patients. One common mistake is assuming that all patients require extensive cardiac testing, even when there are no significant risk factors or symptoms present. For example, if a patient has no significant past medical history and their examination is unremarkable, an echocardiogram is not necessary.
On the other hand, some clinicians may be too cautious and cancel a patient’s procedure based on a perceived cardiac risk that is not supported by evidence. If the patient’s ECG is normal and there are no cardiac risk factors, cancelling the procedure would be unreasonable.
It is important to recognise that not all preoperative patients require extensive cardiac testing. Instead, clinicians should focus on identifying patients with specific cardiac conditions that require closer monitoring and management. By avoiding unnecessary testing and interventions, clinicians can improve patient outcomes and reduce healthcare costs.
-
This question is part of the following fields:
- Surgery
-
-
Question 10
Incorrect
-
A 50-year-old woman presents with fever and pain in the upper right quadrant. Her blood work reveals an elevated CRP and an ultrasound confirms acute cholecystitis. The patient is administered analgesia and IV fluids. What other treatment options are likely to be prescribed for this patient?
Your Answer:
Correct Answer: Intravenous antibiotics + laparoscopic cholecystectomy within 1 week
Explanation:Acute cholecystitis is a condition where the gallbladder becomes inflamed. This is usually caused by gallstones, which are present in 90% of cases. The remaining 10% of cases are known as acalculous cholecystitis and are typically seen in severely ill patients who are hospitalized. The pathophysiology of acute cholecystitis is multifactorial and can be caused by gallbladder stasis, hypoperfusion, and infection. In immunosuppressed patients, it may develop due to Cryptosporidium or cytomegalovirus. This condition is associated with high morbidity and mortality rates.
The main symptom of acute cholecystitis is right upper quadrant pain, which may radiate to the right shoulder. Patients may also experience fever and signs of systemic upset. Murphy’s sign, which is inspiratory arrest upon palpation of the right upper quadrant, may be present. Liver function tests are typically normal, but deranged LFTs may indicate Mirizzi syndrome, which is caused by a gallstone impacted in the distal cystic duct, causing extrinsic compression of the common bile duct.
Ultrasound is the first-line investigation for acute cholecystitis. If the diagnosis remains unclear, cholescintigraphy (HIDA scan) may be used. In this test, technetium-labelled HIDA is injected IV and taken up selectively by hepatocytes and excreted into bile. In acute cholecystitis, there is cystic duct obstruction, and the gallbladder will not be visualized.
The treatment for acute cholecystitis involves intravenous antibiotics and cholecystectomy. NICE now recommends early laparoscopic cholecystectomy, within 1 week of diagnosis. Previously, surgery was delayed for several weeks until the inflammation had subsided. Pregnant women should also proceed to early laparoscopic cholecystectomy to reduce the chances of maternal-fetal complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 11
Incorrect
-
A 65-year-old patient arrives at the emergency department with complaints of abdominal pain and distention. They have not had a bowel movement in 4 days and have not passed gas in 1 day. During the examination, hyperactive bowel sounds are heard, and a digital rectal exam reveals an empty rectum. An urgent CT scan of the abdomen and pelvis with contrast reveals a suspicious large localized lesion in the descending colon, causing bowel obstruction and severely dilated bowel loops.
What is the most appropriate initial surgical option for this patient?Your Answer:
Correct Answer: Loop colostomy
Explanation:The preferred surgical procedure for obstructing cancers in the distal colon is a loop colostomy. This involves creating a stoma with two openings, one connected to the functioning part of the bowel and the other leading into the distal colon to dysfunction and decompress it. The stoma can be reversed at a later time. However, other procedures such as AP resection, ileocolic anastomosis, and ileostomy are not appropriate for this patient’s descending colon mass.
Abdominal stomas are created during various abdominal procedures to bring the lumen or contents of organs onto the skin. Typically, this involves the bowel, but other organs may also be diverted if necessary. The type and method of construction of the stoma will depend on the contents of the bowel. Small bowel stomas should be spouted to prevent irritant contents from coming into contact with the skin, while colonic stomas do not require spouting. Proper siting of the stoma is crucial to reduce the risk of leakage and subsequent maceration of the surrounding skin. The type and location of the stoma will vary depending on the purpose, such as defunctioning the colon or providing feeding access. Overall, abdominal stomas are a necessary medical intervention that requires careful consideration and planning.
-
This question is part of the following fields:
- Surgery
-
-
Question 12
Incorrect
-
A 76-year-old male presents with a one day history of abdominal distension and vomiting.
Upon examination, there is an irreducible lump in the right groin arising below and lateral to the pubic tubercle. A plain abdominal radiograph reveals distended loops of small bowel.
Which of the following hernias are most likely to have caused these symptoms?Your Answer:
Correct Answer: Femoral
Explanation:Small Bowel Obstruction and Femoral Hernias
This patient is experiencing a small bowel obstruction, which is likely caused by an obstructed femoral hernia. The lump in the left groin that cannot be reduced arises below and lateral to the pubic tubercle, indicating a femoral hernia rather than an inguinal hernia, which would produce a lump above and medial to the pubic tubercle. Femoral hernias are the third most common type of hernia, with a higher incidence in elderly multiparous women. It is important to repair all femoral hernias, as 40% of cases are strangulated upon initial presentation. If the overlying skin becomes erythematosus, it is a sign of poor outcome. Obturator hernias are rare and typically do not present with a lump.
Overall, it is crucial to identify the type of hernia causing a small bowel obstruction in order to provide appropriate treatment. Femoral hernias, in particular, require prompt repair to prevent strangulation and potential complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 13
Incorrect
-
A 49-year-old female patient complains of loin pain and haematuria. Upon urine dipstick examination, the results show:
Blood ++++
Nitrites POS
Leucocytes +++
Protein ++
Further urine culture reveals a Proteus infection, while an x-ray confirms the presence of a stag-horn calculus in the left renal pelvis. What is the probable composition of the renal stone?Your Answer:
Correct Answer: Struvite
Explanation:Stag-horn calculi consist of struvite and develop in urine with high alkalinity, which is often caused by the presence of ammonia-producing bacteria.
Types of Renal Stones and their Appearance on X-ray
Renal stones, also known as kidney stones, are solid masses that form in the kidneys due to the accumulation of certain substances. There are different types of renal stones, each with a unique appearance on x-ray. Calcium oxalate stones are the most common, accounting for 40% of cases, and appear opaque on x-ray. Mixed calcium oxalate/phosphate stones and calcium phosphate stones also appear opaque and make up 25% and 10% of cases, respectively. Triple phosphate stones, which develop in alkaline urine and are composed of struvite, account for 10% of cases and appear opaque as well. Urate stones, which are radiolucent, make up 5-10% of cases. Cystine stones, which have a semi-opaque, ‘ground-glass’ appearance, are rare and only account for 1% of cases. Xanthine stones are the least common, accounting for less than 1% of cases, and are also radiolucent. Staghorn calculi, which involve the renal pelvis and extend into at least 2 calyces, are composed of triple phosphate and are more likely to develop in alkaline urine. Infections with Ureaplasma urealyticum and Proteus can increase the risk of their formation.
-
This question is part of the following fields:
- Surgery
-
-
Question 14
Incorrect
-
A 13-year-old boy comes to the clinic with swelling at the lower end of his right femur. Upon examination, a calcified, nodular shadow is observed in his lung on a chest x-ray. What is the most probable diagnosis?
Your Answer:
Correct Answer: Osteosarcoma
Explanation:Osteogenic Sarcoma: A Common Bone Cancer in Children and Adolescents
Osteogenic sarcoma is a prevalent type of bone cancer that primarily affects children and adolescents. It is the third most common malignancy in this age group. The tumour usually originates in the metaphyseal regions of the distal femur, proximal tibia, and proximal humerus, but it can develop in any bone. The cancer can spread regionally within the same extremity or systemically to other organs, such as the lung. Unfortunately, the prognosis worsens dramatically when the tumour metastasises. A common radiological finding in such cases is chest nodules or cannonball lesions.
-
This question is part of the following fields:
- Surgery
-
-
Question 15
Incorrect
-
Which of the following is not a factor that contributes to sensorineural hearing loss?
Your Answer:
Correct Answer: Early otosclerosis
Explanation:Hearing Loss and Cochlear Implants
Hearing loss can be classified into two types: conductive and sensorineural. Conductive hearing loss affects the outer and middle ear, while sensorineural hearing loss affects the cochlea in the inner ear. Cochlear implants are a solution for sensorineural hearing loss, as they provide direct electrical stimulation to the auditory nerve fibers in the cochlea to replicate the function of damaged hair cells.
There are various causes of hair cell damage, including gentamicin toxicity, bacterial meningitis, skull fractures, noise exposure, presbycusis, genetic syndromes, hereditary deafness, and unknown factors. Otosclerosis is another cause of hearing loss, resulting from an overgrowth of bone in the middle ear that fixes the footplate of the stapes at the oval window, leading to conductive hearing loss. If left untreated for an extended period, the cochlea can also become affected, resulting in a mixed hearing loss that is both conductive and sensorineural.
In summary, the different types and causes of hearing loss is crucial in finding the appropriate treatment. Cochlear implants are a viable solution for sensorineural hearing loss, while conductive hearing loss may require different interventions. It is essential to seek medical attention and diagnosis to determine the best course of action for hearing loss.
-
This question is part of the following fields:
- Surgery
-
-
Question 16
Incorrect
-
A 20-year-old student falls from a 2nd-floor window. She is persistently hypotensive. A chest x-ray shows a widened mediastinum with depression of the left main bronchus and deviation of the trachea to the right. What is the most probable injury?
Your Answer:
Correct Answer: Aortic rupture
Explanation:The patient has suffered a deceleration injury and is experiencing ongoing low blood pressure due to a contained hematoma. This suggests that there may be a rupture in the aorta, although a widened mediastinum may not always be visible on a chest X-ray. To obtain a more accurate assessment of the injury, a CT angiogram is recommended. The fact that the patient has been experiencing persistent hypotension from an early stage is more indicative of a hematoma than a tension pneumothorax, which typically only causes low blood pressure as a final symptom before cardiac arrest.
Thoracic Trauma: Common Conditions and Treatment
Thoracic trauma can result in various conditions that require prompt medical attention. Tension pneumothorax, for instance, occurs when pressure builds up in the thorax due to a laceration to the lung parenchyma with a flap. This condition is often caused by mechanical ventilation in patients with pleural injury. Symptoms of tension pneumothorax overlap with cardiac tamponade, but hyper-resonant percussion note is more likely. Flail chest, on the other hand, occurs when the chest wall disconnects from the thoracic cage due to multiple rib fractures. This condition is associated with pulmonary contusion and abnormal chest motion.
Pneumothorax is another common condition resulting from lung laceration with air leakage. Traumatic pneumothoraces should have a chest drain, and patients should never be mechanically ventilated until a chest drain is inserted. Haemothorax, which is most commonly due to laceration of the lung, intercostal vessel, or internal mammary artery, is treated with a large bore chest drain if it is large enough to appear on CXR. Surgical exploration is warranted if more than 1500 ml blood is drained immediately.
Cardiac tamponade is characterized by elevated venous pressure, reduced arterial pressure, and reduced heart sounds. Pulsus paradoxus may also occur with as little as 100 ml blood. Pulmonary contusion is the most common potentially lethal chest injury, and arterial blood gases and pulse oximetry are important. Early intubation within an hour is necessary if significant hypoxia is present. Blunt cardiac injury usually occurs secondary to chest wall injury, and ECG may show features of myocardial infarction. Aorta disruption, diaphragm disruption, and mediastinal traversing wounds are other conditions that require prompt medical attention.
-
This question is part of the following fields:
- Surgery
-
-
Question 17
Incorrect
-
As an FY1 on medical ward cover, you have been tasked with cannulating a 72-year-old female with type-1 diabetes. She is currently being treated for pneumonia, has a right below the knee amputation, and suffers from diabetic neuropathy. What would be the appropriate course of action in this scenario?
Your Answer:
Correct Answer: You should avoid cannulating his foot
Explanation:It is advisable to avoid cannulating the feet of a patient with a known history of diabetes. In this case, the patient has poorly controlled diabetes, diabetic retinopathy, and likely peripheral neuropathy, which has led to amputation. Cannulating the foot could easily result in a diabetic ulcer due to the neuropathy. However, there is no reason why the hand cannot be used for cannulation. While diabetics are more susceptible to infections, there are no guidelines stating that a cannula can only remain in place for 24 hours. It can stay in for up to 3 days, as in most other patients. Administering a shot of antibiotics prior to cannulation is unnecessary and potentially dangerous. A sterile, non-touch technique should be used to minimize the risk of infection, as in any other patient. While cannulation can be stressful for some patients, administering insulin would be inappropriate and hazardous. It is always important to check the patient’s blood glucose levels before administering insulin.
Intravenous Cannula: Colour, Size, and Maximal Flow Rates
Intravenous cannulas are medical devices used to administer fluids, medications, and blood products directly into a patient’s bloodstream. These cannulas come in different sizes and colours, each with a specific maximal flow rate. The colour and size of the cannula determine the amount of fluid that can be administered per minute.
The orange cannula, which has a size of 14g, has the highest maximal flow rate of 270 ml/min. The grey cannula, which has a size of 16g, has a maximal flow rate of 180 ml/min. The green cannula, which has a size of 18g, has a maximal flow rate of 80 ml/min. The pink cannula, which has a size of 20g, has a maximal flow rate of 54 ml/min. Lastly, the blue cannula, which has a size of 22g, has a maximal flow rate of 33 ml/min.
It is important to choose the appropriate cannula size and colour based on the patient’s needs and the type of fluid or medication being administered. Using the wrong cannula size or colour can result in complications such as infiltration, phlebitis, and extravasation. Therefore, healthcare professionals must be knowledgeable about the different types of cannulas and their maximal flow rates to ensure safe and effective patient care.
-
This question is part of the following fields:
- Surgery
-
-
Question 18
Incorrect
-
Which tumour marker is most effective in detecting hepatocellular carcinoma?
Your Answer:
Correct Answer: Serum AFP
Explanation:Liver Tumours: Types, Diagnosis, and Treatment
Liver tumours can be classified as primary or metastatic. Primary liver tumours are relatively rare, with cholangiocarcinoma and hepatocellular carcinoma being the most common types. Hepatocellular carcinoma accounts for 75% of primary liver tumours and is often associated with chronic inflammatory activity, such as cirrhosis or chronic hepatitis B infection. Diagnosis is typically made through imaging modalities like CT or MRI, with elevated levels of a-fetoprotein being a common marker. Biopsy should be avoided as it can spread tumour cells. Treatment options include surgical resection, liver resection, transplantation, and tumour ablation. However, the poor overall survival rate of 15% at 5 years highlights the need for better treatment options.
Cholangiocarcinoma is the second most common type of primary liver malignancy, with up to 80% of tumours arising in the extrahepatic biliary tree. Primary sclerosing cholangitis is a major risk factor, and patients typically present with jaundice. Diagnosis is made through liver function tests, imaging methods like CT or MRI, and elevated levels of tumour markers like CA 19-9, CEA, and CA 125. Surgical resection offers the best chance of cure, but local invasion of peri hilar tumours and lobar atrophy can often make it impossible. Palliation of jaundice is important, but metallic stents should be avoided in those considered for resection. The poor survival rate of approximately 5-10% 5 year survival highlights the need for better treatment options.
In summary, liver tumours can be classified as primary or metastatic, with primary liver tumours being relatively rare. Hepatocellular carcinoma and cholangiocarcinoma are the most common types of primary liver tumours, with diagnosis typically made through imaging modalities and elevated tumour markers. Treatment options include surgical resection, liver resection, transplantation, and tumour ablation, but the poor overall survival rate highlights the need for better treatment options.
-
This question is part of the following fields:
- Surgery
-
-
Question 19
Incorrect
-
A 28-year-old woman presents to the breast clinic with a lump in her right breast that she has noticed for the past 4 weeks. She denies any pain, discharge, or skin changes. The patient is concerned about the lump as she has recently started a new relationship and her partner has also noticed it. On examination, a mobile, smooth, firm breast lump measuring 3.5 cm is palpated. Ultrasound confirms a fibroadenoma. What is the best course of action for this patient?
Your Answer:
Correct Answer: Surgical excision
Explanation:Surgical excision is the recommended treatment for fibroadenomas larger than 3 cm in size. This is because such masses can cause cosmetic concerns and discomfort, especially if they continue to grow. Given the patient’s expressed anxiety about the mass, surgical excision should be offered as a treatment option. Anastrozole, which is used to treat hormone-receptor-positive breast cancer in postmenopausal women, is not appropriate in this case as the patient has a benign breast lesion, and there is no information about hormone receptor status or menopausal status. Tamoxifen, which has been shown to reduce benign breast lump development in some pre-menopausal women, is not a primary treatment for fibroadenomas. Ultrasound-guided monochloroacetic acid injection is also not a suitable treatment option as it is used for plantar wart management and not for breast cryotherapy. While some centers may offer ultrasound-guided cryotherapy for fibroadenomas smaller than 4 cm, surgical excision is the more common treatment.
Understanding Breast Fibroadenoma
Breast fibroadenoma is a type of breast mass that develops from a whole lobule. It is characterized by a mobile, firm, and smooth lump in the breast, which is often referred to as a breast mouse. Fibroadenoma accounts for about 12% of all breast masses and is more common in women under the age of 30.
Fortunately, fibroadenomas are usually benign and do not increase the risk of developing breast cancer. In fact, over a two-year period, up to 30% of fibroadenomas may even get smaller on their own. However, if the lump is larger than 3 cm, surgical excision is typically recommended.
In summary, breast fibroadenoma is a common type of breast mass that is usually benign and does not increase the risk of breast cancer. While it may cause concern for some women, it is important to remember that most fibroadenomas do not require treatment and may even resolve on their own.
-
This question is part of the following fields:
- Surgery
-
-
Question 20
Incorrect
-
A 21-year-old male comes to the emergency department with a complaint of vomiting fresh blood after a 72-hour drinking binge. He denies regular alcohol abuse.
During the examination, his pulse is found to be 92 beats per minute and his blood pressure is 146/90 mmHg.
What is the probable diagnosis for this patient?Your Answer:
Correct Answer: Mallory-Weiss tear
Explanation:Causes of Gastrointestinal Bleeding
Gastrointestinal bleeding can be caused by various factors, including Mallory-Weiss tears, aortoduodenal fistula, Meckel’s diverticulum, oesophageal varices, and peptic ulcers. Mallory-Weiss tears occur in the gastro-oesophageal junction due to forceful or prolonged coughing or vomiting, often after excessive alcohol intake or epileptic convulsions. This can result in vomiting bright red blood or passing blood per rectum. Aortoduodenal fistula is caused by erosion of the duodenum into the aorta due to tumour or previous repair of the aorta with a synthetic graft. Meckel’s diverticulum, which occasionally occurs in the ileum, may contain ectopic gastric mucosa, leading to rectal bleeding. Oesophageal varices are dilated venous collaterals that result from portal hypertension in patients with liver cirrhosis. Finally, peptic ulcers are the most common cause of upper gastrointestinal bleeds, with mucosal erosions developing due to non-steroidal anti-inflammatory drugs, steroids, or prolonged alcohol abuse. Despite the potential severity of these conditions, bleeding usually stops spontaneously.
-
This question is part of the following fields:
- Surgery
-
-
Question 21
Incorrect
-
A 67-year-old man visits his GP complaining of pain in his buttocks. The vascular team is consulted as they suspect he may have peripheral arterial disease. He experiences pain while walking, which subsides within 2 minutes of resting, but reports no pain in his calves. Angiography is recommended. Which vessel is most likely affected based on his symptoms?
Your Answer:
Correct Answer: Iliac stenosis
Explanation:When a person experiences claudication, the affected vessels can be determined by the location of their pain. If the pain is mainly in the buttocks, it is likely that the iliac vessels are stenosed. However, if the pain is mainly in the calves, it is more likely that the femoral artery is affected. Other vessels listed are located below the distribution of the femoral artery, so symptoms would occur lower than this.
Understanding Peripheral Arterial Disease: Intermittent Claudication
Peripheral arterial disease (PAD) can present in three main patterns, one of which is intermittent claudication. This condition is characterized by aching or burning in the leg muscles following walking, which is typically relieved within minutes of stopping. Patients can usually walk for a predictable distance before the symptoms start, and the pain is not present at rest.
To assess for intermittent claudication, healthcare professionals should check the femoral, popliteal, posterior tibialis, and dorsalis pedis pulses. They should also perform an ankle brachial pressure index (ABPI) test, which measures the ratio of blood pressure in the ankle to that in the arm. A normal ABPI result is 1, while a result between 0.6-0.9 indicates claudication. A result between 0.3-0.6 suggests rest pain, and a result below 0.3 indicates impending limb loss.
Duplex ultrasound is the first-line investigation for PAD, while magnetic resonance angiography (MRA) should be performed prior to any intervention. Understanding the symptoms and assessment of intermittent claudication is crucial for early detection and management of PAD.
-
This question is part of the following fields:
- Surgery
-
-
Question 22
Incorrect
-
A 16-year-old male patient complains of sudden pain in his left testicle. He denies any sexual activity. Upon examination, the scrotum appears normal, but the left testis is swollen and tender. The right testis appears to be normal. A urine dip test shows negative results. What is the probable diagnosis?
Your Answer:
Correct Answer: Testicular torsion
Explanation:Acute Testicular Pain and Its Implications
Acute testicular pain is a serious condition that requires immediate attention. It is often caused by testicular torsion, which can lead to irreversible damage if not treated promptly. The diagnosis of testicular torsion is primarily clinical, and investigations such as ultrasound may not be helpful or may cause delay. Therefore, surgical referral is necessary if acute testicular pain is suspected.
In cases of testicular torsion, exploration and fixing of the other side may also be necessary. It is better to explore and be wrong than to delay treatment and risk irreversible damage. The features of testicular torsion include acute pain and swelling of the testis, with an absent cremasteric reflex. On the other hand, epididymitis may also cause acute pain and swelling, but it is rare before puberty and more common in sexually active individuals.
In summary, acute testicular pain is a serious condition that requires urgent attention. Testicular torsion is a clinical diagnosis that should prompt surgical referral, and investigations may not be helpful or may cause delay. It is better to explore and fix the other side if necessary than to delay treatment and risk irreversible damage.
-
This question is part of the following fields:
- Surgery
-
-
Question 23
Incorrect
-
An 80-year-old male is admitted to the urology ward with acute urinary retention. He is catheterised successfully with a large retention volume of 1.5 litres and therefore kept on the ward for observation. Over the next 24 hours, the patient has a urine output of 200 ml/hour and develops increasing confusion. His blood results are as follows:
Hb 130 g/L Male: (135-180)
Platelets 280 * 109/L (150 - 400)
WBC 9 * 109/L (4.0 - 11.0)
Na+ 136 mmol/L (135 - 145)
K+ 4.5 mmol/L (3.5 - 5.0)
Urea 8 mmol/L (2.0 - 7.0)
Creatinine 130 µmol/L (55 - 120)
CRP 3 mg/L (< 5)
What could be the possible reason for the patient's confusion?Your Answer:
Correct Answer: Post-obstructive diuresis
Explanation:To prevent any further deterioration of AKI, the patient’s urine output was replaced with intravenous fluids. Delirium, which can present as confusion, is often caused by infection or uncontrolled pain. However, since there were no indications of infection or pain in the patient’s medical history, delirium was not considered the primary differential diagnosis. Although diabetes insipidus can cause polyuria, it is unlikely in this case as there were no known triggers such as lithium therapy.
Acute urinary retention is a condition where a person suddenly becomes unable to pass urine voluntarily, typically over a period of hours or less. It is a common urological emergency that requires investigation to determine the underlying cause. While it is more common in men, it rarely occurs in women, with an incidence ratio of 13:1. Acute urinary retention is most frequently seen in men over 60 years of age, and the incidence increases with age. It has been estimated that around a third of men in their 80s will develop acute urinary retention over a five-year period.
The most common cause of acute urinary retention in men is benign prostatic hyperplasia, a non-cancerous enlargement of the prostate gland that presses on the urethra, making it difficult for the bladder to empty. Other causes include urethral obstructions, such as strictures, calculi, cystocele, constipation, or masses, as well as certain medications that affect nerve signals to the bladder. In some cases, there may be a neurological cause for the condition. Acute urinary retention can also occur postoperatively and in women postpartum, typically due to a combination of risk factors.
Patients with acute urinary retention typically experience an inability to pass urine, lower abdominal discomfort, and considerable pain or distress. Elderly patients may also present with an acute confusional state. Unlike chronic urinary retention, which is typically painless, acute urinary retention is associated with pain and discomfort. A palpable distended urinary bladder may be detected on abdominal or rectal examination, and lower abdominal tenderness may also be present. All patients should undergo a rectal and neurological examination, and women should also have a pelvic examination.
To confirm the diagnosis of acute urinary retention, a bladder ultrasound should be performed. The bladder volume should be greater than 300 cc to confirm the diagnosis, but if the history and examination are consistent with acute urinary retention, an inconsistent bladder scan does not rule out the condition. Acute urinary retention is managed by decompressing the bladder via catheterisation. Further investigation should be targeted by the likely cause, and patients may require IV fluids to correct any temporary over-diuresis that may occur as a complication.
-
This question is part of the following fields:
- Surgery
-
-
Question 24
Incorrect
-
A 50-year-old woman presents to the surgical assessment unit with worsening upper right abdominal pain after dining out with friends. She reports experiencing this pain for the past few months, but it has never been this severe. The pain tends to worsen after dinner, especially with fast food, and occasionally radiates to her right shoulder. Upon examination, you note an increase in body weight. Her abdomen is soft and non-tender, and bowel sounds are present. She is currently not running a fever. What is the definitive treatment for this condition?
Your Answer:
Correct Answer: Elective laparoscopic cholecystectomy
Explanation:Elective laparoscopic cholecystectomy is the preferred treatment for biliary colic.
Biliary colic is typically characterized by worsening pain after eating, but the patient is generally in good health, has no fever, and has a soft abdomen. In contrast, cholecystitis is associated with signs of infection, such as fever and tachycardia, and may involve palpable gallbladder and positive Murphy’s sign. If the patient is clinically stable and a good candidate for surgery, elective cholecystectomy is the appropriate management option. Cholecystostomy is reserved for cases of acute cholecystitis with pus accumulation, while ERCP is used to remove obstructing gallstones in patients with jaundice or risk of ascending cholangitis. MRCP is a diagnostic tool and not a treatment option.
Biliary colic is a condition that occurs when gallstones pass through the biliary tree. The risk factors for this condition are commonly referred to as the ‘4 F’s’, which include being overweight, female, fertile, and over the age of forty. Other risk factors include diabetes, Crohn’s disease, rapid weight loss, and certain medications. Biliary colic occurs due to an increase in cholesterol, a decrease in bile salts, and biliary stasis. The pain associated with this condition is caused by the gallbladder contracting against a stone lodged in the cystic duct. Symptoms include right upper quadrant abdominal pain, nausea, and vomiting. Diagnosis is typically made through ultrasound. Elective laparoscopic cholecystectomy is the recommended treatment for biliary colic. However, around 15% of patients may have gallstones in the common bile duct at the time of surgery, which can result in obstructive jaundice. Other possible complications of gallstone-related disease include acute cholecystitis, ascending cholangitis, acute pancreatitis, gallstone ileus, and gallbladder cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 25
Incorrect
-
A 67-year-old male is admitted to your surgical ward for an elective hemicolectomy tomorrow due to Duke's B colonic cancer. During your admission assessment, you observe that his full blood count (FBC) indicates a microcytic anaemia with a haemoglobin level of 60 g/L. His previous FBC 4 months ago showed Hb 90 g/L. Haematinic blood tests reveal that the cause of the microcytosis is iron deficiency.
What would be the most suitable approach to manage his anaemia?Your Answer:
Correct Answer: Pre-operative blood transfusion
Explanation:To prepare for surgery, it is necessary to correct the haemoglobin level of 58 g/L. However, this can only be achieved within a short period of time through a blood transfusion. If the issue had been detected earlier, iron transfusions or oral iron supplements would have been recommended over a longer period of weeks to months.
Preparation for surgery varies depending on whether the patient is undergoing an elective or emergency procedure. For elective cases, it is important to address any medical issues beforehand through a pre-admission clinic. Blood tests, urine analysis, and other diagnostic tests may be necessary depending on the proposed procedure and patient fitness. Risk factors for deep vein thrombosis should also be assessed, and a plan for thromboprophylaxis formulated. Patients are advised to fast from non-clear liquids and food for at least 6 hours before surgery, and those with diabetes require special management to avoid potential complications. Emergency cases require stabilization and resuscitation as needed, and antibiotics may be necessary. Special preparation may also be required for certain procedures, such as vocal cord checks for thyroid surgery or bowel preparation for colorectal cases.
-
This question is part of the following fields:
- Surgery
-
-
Question 26
Incorrect
-
A 20-year-old female presents to the emergency department with a 3 day history of lower abdominal pain. She also complains of nausea and vomiting, and has not had a bowel movement for 24 hours. She has mild dysuria and her LMP was 20 days ago. She smokes 15 cigarettes a day and drinks 10 units of alcohol per week. On examination she is stable, with pain in the left iliac fossa. Urinary pregnancy and dipstick are both negative. What is the most likely diagnosis?
Your Answer:
Correct Answer: Appendicitis
Explanation:Typical symptoms of acute appendicitis, such as being young, experiencing pain in the lower right abdomen, and having associated symptoms, were observed. Urinary tests ruled out the possibility of a urinary tract infection or ectopic pregnancy. Mittelschmerz, also referred to as mid-cycle pain, was also considered.
Possible Causes of Right Iliac Fossa Pain
Right iliac fossa pain can be caused by various conditions, and it is important to differentiate between them to provide appropriate treatment. One of the most common causes is appendicitis, which is characterized by pain radiating to the right iliac fossa, anorexia, and a short history. On the other hand, Crohn’s disease often has a long history, signs of malnutrition, and a change in bowel habit, especially diarrhea. Mesenteric adenitis, which mainly affects children, is caused by viruses and bacteria and is associated with a higher temperature than appendicitis. Diverticulitis, both left and right-sided, may present with right iliac fossa pain, and a CT scan may help in refining the diagnosis.
Other possible causes of right iliac fossa pain include Meckel’s diverticulitis, perforated peptic ulcer, incarcerated right inguinal or femoral hernia, bowel perforation secondary to caecal or colon carcinoma, gynecological causes such as pelvic inflammatory disease and ectopic pregnancy, urological causes such as ureteric colic and testicular torsion, and other conditions like TB, typhoid, herpes zoster, AAA, and situs inversus.
It is important to consider the patient’s clinical history, physical examination, and diagnostic tests to determine the underlying cause of right iliac fossa pain. Prompt diagnosis and treatment can prevent complications and improve outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 27
Incorrect
-
A 68-year-old man presents with a three-month history of typical dyspepsia symptoms, including epigastric pain and a 2-stone weight loss. Despite treatment with a proton pump inhibitor, he has not experienced any relief. He now reports difficulty eating solids and frequent post-meal vomiting. On examination, a palpable mass is found in the epigastrium. His full blood count shows a haemoglobin level of 85 g/L (130-180). What is the probable diagnosis?
Your Answer:
Correct Answer: Carcinoma of stomach
Explanation:Alarm Symptoms of Foregut Malignancy
The presence of alarm symptoms in patients over 55 years old, such as weight loss, bleeding, dysphagia, vomiting, blood loss, and a mass, are indicative of a malignancy of the foregut. It is crucial to refer these patients for urgent endoscopy, especially if dysphagia is a new onset symptom. However, it is unfortunate that patients with alarm symptoms are often treated with PPIs instead of being referred for further evaluation. Although PPIs may provide temporary relief, they only delay the diagnosis of the underlying tumor.
The patient’s symptoms should not be ignored, and prompt referral for endoscopy is necessary to rule out malignancy. Early detection and treatment of foregut malignancy can significantly improve patient outcomes. Therefore, it is essential to recognize the alarm symptoms and refer patients for further evaluation promptly. Healthcare providers should avoid prescribing PPIs as a first-line treatment for patients with alarm symptoms and instead prioritize timely referral for endoscopy.
-
This question is part of the following fields:
- Surgery
-
-
Question 28
Incorrect
-
A 50-year-old man is at his pre-operative assessment for his scheduled hernia repair next week. During the consultation, he informs the anaesthetist that his father and brother had a reaction to an anaesthetic in the past, which was later diagnosed as malignant hyperthermia.
What medication should the anaesthetist avoid administering in this situation?Your Answer:
Correct Answer: Suxamethonium
Explanation:Out of the drugs listed, suxamethonium is the only one that can trigger malignant hyperthermia. The rest of the drugs are considered safe for use in individuals with this condition.
Malignant Hyperthermia: A Condition Triggered by Anaesthetic Agents
Malignant hyperthermia is a medical condition that often occurs after the administration of anaesthetic agents. It is characterized by hyperpyrexia and muscle rigidity, which is caused by the excessive release of calcium ions from the sarcoplasmic reticulum of skeletal muscle. This condition is associated with defects in a gene on chromosome 19 that encodes the ryanodine receptor, which controls calcium release from the sarcoplasmic reticulum. Susceptibility to malignant hyperthermia is inherited in an autosomal dominant fashion. It is worth noting that neuroleptic malignant syndrome may have a similar aetiology.
The causative agents of malignant hyperthermia include halothane, suxamethonium, and other drugs such as antipsychotics (which can trigger neuroleptic malignant syndrome). To diagnose this condition, doctors may perform tests such as checking for elevated levels of creatine kinase and conducting contracture tests with halothane and caffeine.
The management of malignant hyperthermia involves the use of dantrolene, which prevents the release of calcium ions from the sarcoplasmic reticulum. With prompt and appropriate treatment, patients with malignant hyperthermia can recover fully. Therefore, it is essential to be aware of the risk factors and symptoms of this condition, especially when administering anaesthetic agents.
-
This question is part of the following fields:
- Surgery
-
-
Question 29
Incorrect
-
Which one of the following is not typically observed in coning caused by elevated intracranial pressure?
Your Answer:
Correct Answer: Hypotension
Explanation:The three components of Cushings triad are changes in pulse pressure, respiratory patterns, and widening of the pulse pressure.
Coning and the Effects of Increased Intracranial Pressure
The cranial vault is a limited space within the skull, except in infants with an unfused fontanelle. When intracranial pressure (ICP) rises, cerebrospinal fluid (CSF) can shift to accommodate the increase. However, once the CSF has reached its capacity, ICP will rapidly rise. The brain has the ability to regulate its own blood supply, and as ICP increases, the body’s circulation will adjust to meet the brain’s perfusion needs, often resulting in hypertension.
As ICP continues to rise, the brain will become compressed, leading to cranial nerve damage and compression of vital centers in the brainstem. If the cardiac center is affected, bradycardia may develop. This process is known as coning and can have severe consequences if left untreated. It is important to monitor ICP and intervene promptly to prevent coning and its associated complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 30
Incorrect
-
A 67-year-old man presents to the emergency department with central abdominal pain. He denies any fever, weight loss or recent travel. Past medical history included hypertension and appendicectomy for an inflamed appendix 3 years ago.
On examination, there is a firm mass over the abdominal wall. The overlying skin is dusky with signs of ischaemia and necrosis.
Given the signs of ischaemia, you perform a venous blood gas (VBG).
pH 7.22 (7.35-7.45)
pCO2 3.1kPa (4.5-6.0)
pO2 5.1kPa (4.0-5.3)
HCO3- 15 mmol/L (22-26)
Routine work-up to investigate the underlying cause reveals:
Hb 128 g/L Male: (135-180)
Female: (115 - 160)
Platelets 200 * 109/L (150 - 400)
WBC 13 * 109/L (4.0 - 11.0)
Bilirubin 15 µmol/L (3 - 17)
ALP 50 u/L (30 - 100)
ALT 39 u/L (3 - 40)
What is the most likely diagnosis?Your Answer:
Correct Answer: Richter's hernia
Explanation:Richter’s hernia can cause strangulation without any signs of obstruction. This is because the bowel lumen remains open while the bowel wall is compromised. A VBG test may reveal metabolic acidosis, indicated by a low pH, low bicarbonate, and low pCO2 due to partial respiratory compensation. This type of acidosis can occur due to lactate build-up. Unlike Richter’s hernia, small bowel obstruction is less likely to cause a firm, red mass on the abdominal wall. Conditions such as diabetic ketoacidosis and pancreatitis may cause abdominal pain and metabolic acidosis, but they do not explain the presence of a firm mass on the abdominal wall or the skin’s dusky appearance. Ascending cholangitis typically presents with Charcot’s triad, which includes right upper quadrant pain, fever, and jaundice, but this is not the case here. In some cases, it may also cause confusion and hypotension, which is known as Reynold’s pentad.
Abdominal wall hernias occur when an organ or the fascia of an organ protrudes through the wall of the cavity that normally contains it. Risk factors for developing these hernias include obesity, ascites, increasing age, and surgical wounds. Symptoms of abdominal wall hernias include a palpable lump, cough impulse, pain, obstruction (more common in femoral hernias), and strangulation (which can compromise the bowel blood supply and lead to infarction). There are several types of abdominal wall hernias, including inguinal hernias (which account for 75% of cases and are more common in men), femoral hernias (more common in women and have a high risk of obstruction and strangulation), umbilical hernias (symmetrical bulge under the umbilicus), paraumbilical hernias (asymmetrical bulge), epigastric hernias (lump in the midline between umbilicus and xiphisternum), incisional hernias (which may occur after abdominal surgery), Spigelian hernias (rare and seen in older patients), obturator hernias (more common in females and can cause bowel obstruction), and Richter hernias (a rare type of hernia that can present with strangulation without symptoms of obstruction). In children, congenital inguinal hernias and infantile umbilical hernias are the most common types, with surgical repair recommended for the former and most resolving on their own for the latter.
-
This question is part of the following fields:
- Surgery
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)