-
Question 1
Correct
-
A 25-year-old woman presents to the emergency department complaining of right-sided back pain and dysuria that has been bothering her for the past two days. The pain is constant and severe, and it radiates from her renal angle to her groin. Upon examination, her temperature is 38.1ºC, her heart rate is 101 bpm, her blood pressure is 139/91 mmHg, and she has a tender renal angle with a palpable mass on the right side of her abdomen. What is the most appropriate investigation to evaluate her abdominal mass?
Your Answer: Ultrasound of the renal tract
Explanation:The most likely diagnosis for the patient’s symptoms is a ureteric stone causing obstruction in the right kidney, resulting in hydronephrosis. A physical examination may reveal a palpable mass. To confirm the diagnosis, an ultrasound of the renal tract is the best initial investigation as it can detect any obstruction in the renal tract. It is important to avoid exposing the patient to unnecessary radiation, especially if they are under 20 years old or women of childbearing age. The first-line treatment for hydronephrosis is a nephrostomy, which is performed under ultrasound guidance. Once the diagnosis is confirmed, a CT scan of the abdomen and pelvis without contrast is recommended to identify the cause of the obstruction. Contrast agents are not useful in this situation as they make stones invisible on the scan. An intravenous urogram is also not helpful as it does not provide 3-dimensional images of the kidneys. A urine dip may show blood, which could suggest stone pathology, but it cannot determine the cause of the palpable mass.
Hydronephrosis is a condition where the kidney becomes swollen due to urine buildup. There are various causes of hydronephrosis, including pelvic-ureteric obstruction, aberrant renal vessels, calculi, tumors of the renal pelvis, stenosis of the urethra, urethral valve, prostatic enlargement, extensive bladder tumor, and retroperitoneal fibrosis. Unilateral hydronephrosis is caused by one of these factors, while bilateral hydronephrosis is caused by a combination of pelvic-ureteric obstruction, aberrant renal vessels, and tumors of the renal pelvis.
To investigate hydronephrosis, ultrasound is the first-line test to identify the presence of hydronephrosis and assess the kidneys. IVU is used to assess the position of the obstruction, while antegrade or retrograde pyelography allows for treatment. If renal colic is suspected, a CT scan is used to detect the majority of stones.
The management of hydronephrosis involves removing the obstruction and draining urine. In cases of acute upper urinary tract obstruction, a nephrostomy tube is used, while chronic upper urinary tract obstruction is treated with a ureteric stent or a pyeloplasty. The CT scan image shows a large calculus in the left ureter with accompanying hydroureter and massive hydronephrosis in the left kidney.
Overall, hydronephrosis is a serious condition that requires prompt diagnosis and treatment to prevent further complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 2
Incorrect
-
A 13-year-old boy comes to the clinic with swelling at the lower end of his right femur. Upon examination, a calcified, nodular shadow is observed in his lung on a chest x-ray. What is the most probable diagnosis?
Your Answer: Osteomyelitis
Correct Answer: Osteosarcoma
Explanation:Osteogenic Sarcoma: A Common Bone Cancer in Children and Adolescents
Osteogenic sarcoma is a prevalent type of bone cancer that primarily affects children and adolescents. It is the third most common malignancy in this age group. The tumour usually originates in the metaphyseal regions of the distal femur, proximal tibia, and proximal humerus, but it can develop in any bone. The cancer can spread regionally within the same extremity or systemically to other organs, such as the lung. Unfortunately, the prognosis worsens dramatically when the tumour metastasises. A common radiological finding in such cases is chest nodules or cannonball lesions.
-
This question is part of the following fields:
- Surgery
-
-
Question 3
Incorrect
-
To which bone does Sever's disease refer, and at what age is it commonly diagnosed?
Your Answer: Radius
Correct Answer: Calcaneum
Explanation:Sever’s Disease
Sever’s disease is a condition that causes pain in one or both heels when walking or standing. It occurs due to a disturbance or interruption in the growth plates located at the back of the heel bone, also known as the calcaneus. This condition typically affects children between the ages of 8 and 13 years old.
The pain associated with Sever’s disease can occur after general activities such as running, jumping, or playing sports like netball, basketball, and football. Symptoms include extreme pain when placing the heel on the ground, which can be alleviated when the child walks on their tiptoes.
In summary, Sever’s disease is a common condition that affects children during their growth and development. It is important to recognize the symptoms and seek medical attention if necessary to ensure proper treatment and management of the condition.
-
This question is part of the following fields:
- Surgery
-
-
Question 4
Incorrect
-
A 55-year-old male with hypercalcaemia secondary to primary hyperparathyroidism presents with renal colic. An ultrasound scan reveals ureteric obstruction caused by a stone. Despite multiple attempts at stone extraction, the stone remains lodged. The patient is now experiencing sepsis with a fever of 39.5ºC and has been administered antibiotics. What is the optimal plan of action?
Your Answer: Cystoscopy and insertion of ureteric stent
Correct Answer: Insertion of nephrostomy
Explanation:When a person experiences acute upper urinary tract obstruction, the recommended course of action is to undergo nephrostomy. In this case, it is likely that the obstruction was caused by a calculus or stone in the ureter. If left untreated, the stagnant urine can become infected, which is considered a serious urological emergency. Since the stone cannot be removed, a nephrostomy is necessary.
Hydronephrosis is a condition where the kidney becomes swollen due to urine buildup. There are various causes of hydronephrosis, including pelvic-ureteric obstruction, aberrant renal vessels, calculi, tumors of the renal pelvis, stenosis of the urethra, urethral valve, prostatic enlargement, extensive bladder tumor, and retroperitoneal fibrosis. Unilateral hydronephrosis is caused by one of these factors, while bilateral hydronephrosis is caused by a combination of pelvic-ureteric obstruction, aberrant renal vessels, and tumors of the renal pelvis.
To investigate hydronephrosis, ultrasound is the first-line test to identify the presence of hydronephrosis and assess the kidneys. IVU is used to assess the position of the obstruction, while antegrade or retrograde pyelography allows for treatment. If renal colic is suspected, a CT scan is used to detect the majority of stones.
The management of hydronephrosis involves removing the obstruction and draining urine. In cases of acute upper urinary tract obstruction, a nephrostomy tube is used, while chronic upper urinary tract obstruction is treated with a ureteric stent or a pyeloplasty. The CT scan image shows a large calculus in the left ureter with accompanying hydroureter and massive hydronephrosis in the left kidney.
Overall, hydronephrosis is a serious condition that requires prompt diagnosis and treatment to prevent further complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 5
Correct
-
A 67-year-old woman visits her GP complaining of left flank pain and haematuria that has persisted for 3 weeks. She also reports a dry cough that has worsened over the past month. The patient has a history of smoking for 10 pack years. During the examination, a palpable mass is detected in the left flank. The patient is prescribed pembrolizumab and axitinib for treatment. What stage of cancer is likely to have been present at the time of diagnosis?
Your Answer: Stage 4
Explanation:The patient’s renal cell carcinoma had progressed to stage 4, which is metastatic and often presents with symptoms. This was supported by the fact that the patient was treated with pembrolizumab and axitinib, which are the first-line options for stage 4 disease. Stage 1 and 2 were ruled out as they are typically treated with surgical resection, surveillance, or local ablation. Stage 3 was also ruled out as it involves nearby structure invasion but no distant metastases, and is treated with radical nephrectomy.
Understanding Renal Cell Cancer
Renal cell cancer, also known as hypernephroma, is a primary renal neoplasm that accounts for 85% of cases. It typically arises from the proximal renal tubular epithelium, with the clear cell subtype being the most common. This type of cancer is more prevalent in middle-aged men and is associated with smoking, von Hippel-Lindau syndrome, and tuberous sclerosis. While renal cell cancer is only slightly increased in patients with autosomal dominant polycystic kidney disease, it can present with a classical triad of haematuria, loin pain, and abdominal mass. Other features include pyrexia of unknown origin, endocrine effects, and paraneoplastic hepatic dysfunction syndrome.
The T category criteria for renal cell cancer are based on the size and extent of the tumour. For confined disease, a partial or total nephrectomy may be recommended depending on the tumour size. Patients with a T1 tumour are typically offered a partial nephrectomy, while those with larger tumours may require a total nephrectomy. Treatment options for renal cell cancer include alpha-interferon, interleukin-2, and receptor tyrosine kinase inhibitors such as sorafenib and sunitinib. These medications have been shown to reduce tumour size and treat patients with metastases. It is important to note that renal cell cancer can have paraneoplastic effects, such as Stauffer syndrome, which is associated with cholestasis and hepatosplenomegaly. Overall, early detection and prompt treatment are crucial for improving outcomes in patients with renal cell cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 6
Correct
-
A twenty-five-year-old male with Crohn's disease is admitted to the gastroenterology ward. Despite infliximab therapy, the patient's symptoms persist, and he complains of abdominal pain and high output through his stoma. On examination, he appears pale and cachectic, with a heart rate of 74/minute, regular respiratory rate of 14/minute, oxygen saturations of 99%, temperature of 38.2 ºC, and blood pressure of 122/74 mmHg. The stoma bag is situated in the left iliac fossa, and the stoma site is pink and spouted without evidence of infarction or parastomal hernias. What type of stoma does this patient have?
Your Answer: Ileostomy
Explanation:An ileostomy is a type of stoma that is created to prevent the skin from being exposed to the enzymes in the small intestine. This is commonly seen in patients with Crohn’s disease, which affects the entire gastrointestinal tract. While the location of the stoma may vary, it is the structure of the stoma itself that determines whether it is an ileostomy or a colostomy. In contrast, a tracheostomy is an opening in the trachea, while a nephrostomy is an opening in the kidneys that is used to drain urine into a bag. A urostomy is another type of stoma that is used to divert urine from the urinary system into a bag, but it differs from an ileostomy in that it involves the use of an ileal conduit.
Abdominal stomas are created during various abdominal procedures to bring the lumen or contents of organs onto the skin. Typically, this involves the bowel, but other organs may also be diverted if necessary. The type and method of construction of the stoma will depend on the contents of the bowel. Small bowel stomas should be sprouted to prevent irritant contents from coming into contact with the skin, while colonic stomas do not require spouting. Proper siting of the stoma is crucial to reduce the risk of leakage and subsequent maceration of the surrounding skin. The type and location of the stoma will vary depending on the purpose, such as defunctioning the colon or providing feeding access. Overall, abdominal stomas are a necessary medical intervention that requires careful consideration and planning.
-
This question is part of the following fields:
- Surgery
-
-
Question 7
Incorrect
-
Which one of the following scenarios is the most common presentation of testicular cancer?
Your Answer: Painful testicular lump in a 56-year-old man
Correct Answer: Painless testicular lump in a 27-year-old man
Explanation:Understanding Testicular Cancer
Testicular cancer is a type of cancer that commonly affects men between the ages of 20 and 30. Germ-cell tumors are the most common type of testicular cancer, accounting for around 95% of cases. These tumors can be divided into seminomas and non-seminomas, which include embryonal, yolk sac, teratoma, and choriocarcinoma. Other types of testicular cancer include Leydig cell tumors and sarcomas. Risk factors for testicular cancer include infertility, cryptorchidism, family history, Klinefelter’s syndrome, and mumps orchitis.
The most common symptom of testicular cancer is a painless lump, although some men may experience pain. Other symptoms may include hydrocele and gynaecomastia, which occurs due to an increased oestrogen:androgen ratio. Tumor markers such as hCG, AFP, and beta-hCG may be elevated in germ cell tumors. Ultrasound is the first-line diagnostic tool for testicular cancer.
Treatment for testicular cancer depends on the type and stage of the tumor. Orchidectomy, chemotherapy, and radiotherapy may be used. Prognosis for testicular cancer is generally excellent, with a 5-year survival rate of around 95% for seminomas and 85% for teratomas if caught at Stage I. It is important for men to perform regular self-examinations and seek medical attention if they notice any changes or abnormalities in their testicles.
-
This question is part of the following fields:
- Surgery
-
-
Question 8
Incorrect
-
A 68-year-old male presents to the emergency department with acute right loin pain which has gotten progressively worse over the last couple of hours. On examination, his heart rate is 78 beats per minute, respiratory rate is 19 breaths per minute, blood pressure is 130/85 mmHg, and temperature is 36.6 ºC.
The abdomen is soft and non-tender with a bulge noted in the groin region superior and medial to the pubic tubercle which is unable to be pushed back in. Bowel sounds are present.
What is the most likely diagnosis based on the patient's symptoms?Your Answer: Inguinal strangulated hernia
Correct Answer: Inguinal incarcerated hernia
Explanation:When a hernia cannot be pushed back into place, it is called an incarcerated hernia. These types of hernias are usually painless.
The correct option in this case is an inguinal incarcerated hernia. An incarcerated hernia occurs when the herniated tissue becomes trapped and cannot be pushed back into place. This can cause pain, but there are no other symptoms. If the blood supply to the herniated tissue is compromised, it can lead to strangulation. However, in this case, the patient has a tender, distended abdomen with normal bowel sounds, which suggests that it is not a strangulated hernia.
The option of an incarcerated femoral hernia is incorrect because femoral hernias are located inferior and lateral to the pubic tubercle, whereas inguinal hernias are medial and superior.
The option of a femoral strangulated hernia is also incorrect because the patient’s vital signs are normal and there are no systemic symptoms. Additionally, femoral hernias are located inferior and lateral to the pubic tubercle, whereas inguinal hernias are medial and superior.
The absence of systemic symptoms and normal vital signs suggest that the hernia is likely an inguinal incarcerated hernia, rather than a strangulated hernia.
Understanding Strangulated Inguinal Hernias
An inguinal hernia occurs when abdominal contents protrude through the superficial inguinal ring. This can happen directly through the deep inguinal ring or indirectly through the posterior wall of the inguinal canal. Hernias should be reducible, meaning that the herniated tissue can be pushed back into place in the abdomen through the defect using a hand. However, if a hernia cannot be reduced, it is referred to as an incarcerated hernia, which is at risk of strangulation. Strangulation is a surgical emergency where the blood supply to the herniated tissue is compromised, leading to ischemia or necrosis.
Symptoms of a strangulated hernia include pain, fever, an increase in the size of a hernia or erythema of the overlying skin, peritonitic features such as guarding and localised tenderness, bowel obstruction, and bowel ischemia. Imaging can be used in cases of suspected strangulation, but it is not considered necessary and is more useful in excluding other pathologies. Repair involves immediate surgery, either from an open or laparoscopic approach with a mesh technique. This is the same technique used in elective hernia repair, however, any dead bowel will also have to be removed. While waiting for the surgery, it is not recommended that you manually reduce strangulated hernias, as this can cause more generalised peritonitis. Strangulation occurs in around 1 in 500 cases of all inguinal hernias, and indications that a hernia is at risk of strangulation include episodes of pain in a hernia that was previously asymptomatic and irreducible hernias.
-
This question is part of the following fields:
- Surgery
-
-
Question 9
Correct
-
A 75-year-old woman undergoes a left hemicolectomy for colon cancer. The pathology report reveals that the tumour has invaded the muscle layer surrounding the colon but there is no lymph node involvement or distant metastasis on the CT scan of the abdomen and pelvis. What is the Dukes stage of the tumour in this patient?
Your Answer: B
Explanation:The tumour in this patient is classified as Duke Stage B, as it has invaded the local tissue outside of the mucosa but does not involve any lymph nodes, which would make it Duke Stage C. Duke Stage D would involve distant metastases. Staging is crucial in determining prognosis and further management.
While Dukes staging is still widely used, TNM classification is gradually replacing it for colorectal tumours. Tumours that are still within the mucosal wall are classified as T1 or T2, while those that have spread outside the mucosal wall are classified as T3 or T4. Lymph node involvement is classified as N0 (no involvement), N1 (up to 3 regional lymph nodes), or N2 (4 or more regional lymph nodes). Metastasis is classified as either M0 (no metastasis) or M1 (metastasis present).
Duke Stage B can be classified as either T3N0M0 or T4N0M0.
Dukes’ Classification: Stages of Colorectal Cancer
Dukes’ classification is a system used to describe the extent of spread of colorectal cancer. It is divided into four stages, each with a different level of severity and prognosis. Stage A refers to a tumour that is confined to the mucosa, with a 95% 5-year survival rate. Stage B describes a tumour that has invaded the bowel wall, with an 80% 5-year survival rate. Stage C indicates the presence of lymph node metastases, with a 65% 5-year survival rate. Finally, Stage D refers to distant metastases, with a 5% 5-year survival rate (although this increases to 20% if the metastases are resectable).
Overall, Dukes’ classification is an important tool for doctors to use when determining the best course of treatment for patients with colorectal cancer. By understanding the stage of the cancer, doctors can make more informed decisions about surgery, chemotherapy, and other treatments. Additionally, patients can use this information to better understand their prognosis and make decisions about their own care.
-
This question is part of the following fields:
- Surgery
-
-
Question 10
Correct
-
A 22-year-old man is struck on the left side of his face while playing rugby. He reports experiencing double vision when both eyes are open and finds it painful to open his mouth.
What is the likely explanation for his symptoms?Your Answer: Depressed fracture of the zygoma
Explanation:Facial trauma can result in fractures of the facial bones, which are often caused by assaults or accidents. The location of the impact can determine the type of injury, with a punch to the cheek bone or eye area commonly resulting in a fractured zygoma. If the globe is ruptured, there will be a significant loss of vision. Monocular visual blurring may indicate a hyphaema, which can be diagnosed through inspection. A ramus fracture can cause difficulty opening the mouth, but will not affect vision. A maxillary antrum rupture may occur as a result of a comminuted maxillary fracture or blowout fracture of the orbit. If a patient has binocular vision and facial trauma, it may suggest a depressed fracture of the zygoma. Inspection and palpation of the orbital margins can reveal a step deformity or depressed contour of the cheek.
Patients with head injuries should be managed according to ATLS principles and extracranial injuries should be managed alongside cranial trauma. There are different types of traumatic brain injuries, including extradural hematoma, subdural hematoma, and subarachnoid hemorrhage. Primary brain injury may be focal or diffuse, and secondary brain injury can occur due to cerebral edema, ischemia, infection, or herniation. Management may include IV mannitol/furosemide, decompressive craniotomy, and ICP monitoring. Pupillary findings can provide information on the location and severity of the injury.
-
This question is part of the following fields:
- Surgery
-
-
Question 11
Incorrect
-
A 65-year-old man complains of dysuria and haematuria. He has no significant medical history, but reports working in a rubber manufacturing plant for 40 years where health and safety regulations were not always strictly enforced. A cystoscopy reveals a high-grade papillary carcinoma, specifically a transitional cell carcinoma of the bladder. What occupational exposure is a known risk factor for this type of bladder cancer?
Your Answer: Strongyloides stercoralis
Correct Answer: Aniline dye
Explanation:Risk Factors for Bladder Cancer
Bladder cancer is a type of cancer that affects the bladder, and there are different types of bladder cancer. The most common type is urothelial (transitional cell) carcinoma, and the risk factors for this type of bladder cancer include smoking, exposure to aniline dyes, rubber manufacture, and cyclophosphamide. Smoking is the most important risk factor in western countries, with a hazard ratio of around 4. Exposure to aniline dyes, such as working in the printing and textile industry, can also increase the risk of bladder cancer. Rubber manufacture and cyclophosphamide are also risk factors for urothelial carcinoma.
On the other hand, squamous cell carcinoma of the bladder has different risk factors. Schistosomiasis and smoking are the main risk factors for this type of bladder cancer. Schistosomiasis is a parasitic infection that can cause inflammation and damage to the bladder, which can increase the risk of developing squamous cell carcinoma. Smoking is also a risk factor for squamous cell carcinoma, as it can cause changes in the cells of the bladder lining that can lead to cancer.
In summary, the risk factors for bladder cancer depend on the type of cancer. Urothelial carcinoma is mainly associated with smoking, exposure to aniline dyes, rubber manufacture, and cyclophosphamide, while squamous cell carcinoma is mainly associated with schistosomiasis and smoking. It is important to be aware of these risk factors and take steps to reduce your risk of developing bladder cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 12
Incorrect
-
A 65-year-old woman comes to the clinic complaining of sudden pain in her right groin. She mentions that she had noticed a swelling in the area on and off for a few years, but it never bothered her before. She denies any nausea, vomiting, changes in bowel habits, or weight loss.
Upon examination, the abdomen appears normal, but there is a tender and irreducible swelling below and to the side of the pubic tubercle.
What is the probable diagnosis?Your Answer: Indirect inguinal hernia
Correct Answer: Femoral hernia
Explanation:Diagnosis and Treatment of Femoral Hernia
The patient’s hernia is located in the typical position of a femoral hernia, which is below and to the side of the pubic tubercle. The patient has reported an intermittent swelling that has become irreducible. Based on these symptoms, it is likely that the femoral canal has been blocked by omentum, rather than a loop of bowel becoming trapped. Since the patient has no other concerning signs, it is safe for them to undergo hernia repair on the next available CEPOD list.
-
This question is part of the following fields:
- Surgery
-
-
Question 13
Correct
-
A 6-month old boy is brought to his pediatrician by the parents. They request circumcision due to their religious beliefs. The doctor explains that this is not a service provided by the NHS unless there is a medical necessity, and it must be done at a private clinic. Before making a decision about performing the procedure, what should be ruled out?
Your Answer: Hypospadias
Explanation:Hypospadias is a reason why circumcision should not be performed in infancy as the foreskin is required for the repair process.
Circumcision is a practice that has been carried out in various cultures for centuries. Today, it is mainly practiced by people of the Jewish and Islamic faith for religious or cultural reasons. However, it is important to note that circumcision for these reasons is not available on the NHS.
The medical benefits of circumcision are still a topic of debate. However, some studies have shown that it can reduce the risk of penile cancer, urinary tract infections, and sexually transmitted infections, including HIV.
There are also medical indications for circumcision, such as phimosis, recurrent balanitis, balanitis xerotica obliterans, and paraphimosis. It is crucial to rule out hypospadias before performing circumcision as the foreskin may be needed for surgical repair.
Circumcision can be performed under local or general anesthesia. It is a personal decision that should be made after careful consideration of the potential benefits and risks.
-
This question is part of the following fields:
- Surgery
-
-
Question 14
Incorrect
-
A 29-year-old patient involved in a car accident is being treated in the ICU. The patient has a challenging airway and has undergone multiple traumatic intubations during their stay, resulting in a persistent air leak in the ventilator circuit. They are now experiencing recurrent hospital-acquired pneumonia. Upon examination, crackles and dullness to percussion are heard at the lung bases, but breath sounds are present throughout the lung fields. The patient's Hb level is 137 g/L (normal range for males: 135-180; females: 115-160), platelet count is 356 * 109/L (normal range: 150-400), and WBC count is 12.9 * 109/L (normal range: 4.0-11.0). What is the most likely cause of the patient's recurring pneumonia?
Your Answer: Atelectasis
Correct Answer: Tracheo-oesophageal fistula
Explanation:The formation of tracheo-oesophageal fistula can be a consequence of prolonged mechanical ventilation in trauma patients.
Airway Management Devices and Techniques
Airway management is a crucial aspect of medical care, especially in emergency situations. In addition to airway adjuncts, there are simple positional manoeuvres that can be used to open the airway, such as head tilt/chin lift and jaw thrust. There are also several devices that can be used for airway management, each with its own advantages and limitations.
The oropharyngeal airway is easy to insert and use, making it ideal for short procedures. It is often used as a temporary measure until a more definitive airway can be established. The laryngeal mask is widely used and very easy to insert. It sits in the pharynx and aligns to cover the airway, but it does not provide good control against reflux of gastric contents. The tracheostomy reduces the work of breathing and may be useful in slow weaning, but it requires humidified air and may dry secretions. The endotracheal tube provides optimal control of the airway once the cuff is inflated and can be used for long or short-term ventilation, but errors in insertion may result in oesophageal intubation.
It is important to note that paralysis is often required for some of these devices, and higher ventilation pressures can be used with the endotracheal tube. Capnography should be monitored to ensure proper placement and ventilation. Each device has its own unique benefits and drawbacks, and the choice of device will depend on the specific needs of the patient and the situation at hand.
-
This question is part of the following fields:
- Surgery
-
-
Question 15
Incorrect
-
A 75-year-old male has been diagnosed with rectal carcinoma and is scheduled for a lower anterior resection with the goal of restoring intestinal continuity. What type of stoma would be most suitable?
Your Answer: End ileostomy
Correct Answer: Loop ileostomy
Explanation:The loop ileostomy is a technique used to redirect the flow of bowel contents away from a distal anastomosis, typically in cases of rectal cancer. When the ileostomy is reversed, it allows for the restoration of bowel continuity and can greatly enhance the patient’s quality of life.
Abdominal stomas are created during various abdominal procedures to bring the lumen or contents of organs onto the skin. Typically, this involves the bowel, but other organs may also be diverted if necessary. The type and method of construction of the stoma will depend on the contents of the bowel. Small bowel stomas should be spouted to prevent irritant contents from coming into contact with the skin, while colonic stomas do not require spouting. Proper siting of the stoma is crucial to reduce the risk of leakage and subsequent maceration of the surrounding skin. The type and location of the stoma will vary depending on the purpose, such as defunctioning the colon or providing feeding access. Overall, abdominal stomas are a necessary medical intervention that requires careful consideration and planning.
-
This question is part of the following fields:
- Surgery
-
-
Question 16
Incorrect
-
You are working as a locum on the paediatric neurosurgical unit. Three of the patients seen on the ward round have subarachnoid haemorrhages. Your consultant wants blood tests on all of them, but forgets to tell you which ones. All three patients are stable. Their aneurysms are secured and they will be discharged in a few days time. Which single blood test is most valuable in these patients?
Your Answer: Full blood count
Correct Answer: Urea and electrolytes
Explanation:Subarachnoid haemorrhages often lead to the development of hyponatraemia, which is a frequently occurring complication. During the acute phase, sodium levels are closely monitored. Blood sugar levels are only relevant if the patient is diabetic or loses consciousness. Liver and thyroid function are usually unaffected by subarachnoid haemorrhages. While a full blood count is useful upon admission, it does not require the same level of monitoring as sodium levels.
A subarachnoid haemorrhage (SAH) is a type of bleeding that occurs within the subarachnoid space of the meninges in the brain. It can be caused by head injury or occur spontaneously. Spontaneous SAH is often caused by an intracranial aneurysm, which accounts for around 85% of cases. Other causes include arteriovenous malformation, pituitary apoplexy, and mycotic aneurysms. The classic symptoms of SAH include a sudden and severe headache, nausea and vomiting, meningism, coma, seizures, and ECG changes.
The first-line investigation for SAH is a non-contrast CT head, which can detect acute blood in the basal cisterns, sulci, and ventricular system. If the CT is normal within 6 hours of symptom onset, a lumbar puncture is not recommended. However, if the CT is normal after 6 hours, a lumbar puncture should be performed at least 12 hours after symptom onset to check for xanthochromia and other CSF findings consistent with SAH. If SAH is confirmed, referral to neurosurgery is necessary to identify the underlying cause and provide urgent treatment.
Management of aneurysmal SAH involves supportive care, such as bed rest, analgesia, and venous thromboembolism prophylaxis. Vasospasm is prevented with oral nimodipine, and intracranial aneurysms require prompt intervention to prevent rebleeding. Most aneurysms are treated with a coil by interventional neuroradiologists, but some require a craniotomy and clipping by a neurosurgeon. Complications of aneurysmal SAH include re-bleeding, hydrocephalus, vasospasm, and hyponatraemia. Predictive factors for SAH include conscious level on admission, age, and amount of blood visible on CT head.
-
This question is part of the following fields:
- Surgery
-
-
Question 17
Incorrect
-
An Emergency Department receives a 70-year-old man who slipped on ice and fell backwards, hitting his head on the kerb and landing on his right arm. The patient has a medical history of atrial fibrillation and is currently taking bisoprolol and warfarin. His INR was 2.2 four days ago. There are no visible injuries on his arm or scalp. What is the best course of action for his head injury?
Your Answer: Admit for 24 hours of observation
Correct Answer: Arrange a CT head scan to be performed within 8 hours
Explanation:NICE Guidelines for Investigating Head Injuries in Adults
Head injuries can be serious and require prompt medical attention. The National Institute for Health and Care Excellence (NICE) has provided clear guidelines for healthcare professionals to determine which adult patients need further investigation with a CT head scan. Patients who require immediate CT head scans include those with a Glasgow Coma Scale (GCS) score of less than 13 on initial assessment, suspected open or depressed skull fractures, signs of basal skull fractures, post-traumatic seizures, focal neurological deficits, and more than one episode of vomiting.
For patients with any loss of consciousness or amnesia since the injury, a CT head scan within 8 hours is recommended for those who are 65 years or older, have a history of bleeding or clotting disorders, experienced a dangerous mechanism of injury, or have more than 30 minutes of retrograde amnesia of events immediately before the head injury. Additionally, patients on warfarin who have sustained a head injury without other indications for a CT head scan should also receive a scan within 8 hours of the injury.
It is important for healthcare professionals to follow these guidelines to ensure that patients receive appropriate and timely care for their head injuries. By identifying those who require further investigation, healthcare professionals can provide the necessary treatment and support to prevent further complications and improve patient outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 18
Correct
-
What is the most frequent complication associated with a clavicle fracture?
Your Answer: Malunion
Explanation:Complications and Risk Factors in Clavicle Fractures
Clavicle fractures are common injuries that can result in various complications. The most frequent complication is malunion, which can cause angulation, shortening, and poor appearance. Although non-anatomic union is typical of most displaced middle-third clavicle fractures, many experts suggest that such malunion does not significantly affect function.
Nonunion is another complication that occurs when there is a failure to show clinical or radiographic progression of healing after four to six months. Several risk factors have been identified, including the extent of initial trauma, fracture combinations, fracture displacement, inadequate immobilisation, distal-third fractures, primary open reduction, and refracture.
It is essential to identify these risk factors to prevent complications and ensure proper treatment. Adequate immobilisation and careful monitoring of the healing process are crucial in preventing nonunion and malunion. In cases where complications do occur, prompt intervention can help minimise the impact on function and appearance.
-
This question is part of the following fields:
- Surgery
-
-
Question 19
Incorrect
-
A 49-year-old woman arrives at the surgical assessment unit with fever, right upper quadrant pain, and yellowing of the sclera. Imaging confirms ascending cholangitis. She has a history of multiple hospitalizations for biliary colic. What is the primary cause of this condition?
Your Answer: Mycobacterium avium complex
Correct Answer: Escherichia coli
Explanation:Ascending cholangitis is commonly caused by E. coli, while Mycobacterium avium complex is unlikely to cause chronic diarrhea in immunodeficient patients. Clostridium difficile is also unlikely to cause this condition, as it typically follows an antibiotic course. Staphylococcus aureus would not be a likely cause of this condition, as it requires a breach in the skin to enter the body.
Understanding Ascending Cholangitis
Ascending cholangitis is a bacterial infection that affects the biliary tree, with E. coli being the most common culprit. This condition is often associated with gallstones, which can predispose individuals to the infection. Patients with ascending cholangitis may present with Charcot’s triad, which includes fever, right upper quadrant pain, and jaundice. However, this triad is only present in 20-50% of cases. Other common symptoms include hypotension and confusion. In severe cases, Reynolds’ pentad may be observed, which includes the additional symptoms of hypotension and confusion.
To diagnose ascending cholangitis, ultrasound is typically used as a first-line investigation to look for bile duct dilation and stones. Raised inflammatory markers may also be observed. Treatment involves intravenous antibiotics and endoscopic retrograde cholangiopancreatography (ERCP) after 24-48 hours to relieve any obstruction.
Overall, ascending cholangitis is a serious condition that requires prompt diagnosis and treatment. Understanding the symptoms and risk factors associated with this condition can help individuals seek medical attention early and improve their chances of a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 20
Incorrect
-
A 55-year-old woman visits her doctor with a lump in her left breast that she noticed a month ago and believes has grown in size. She had her last menstrual period two years ago. Upon examination, a painless, firm nodule is found in her left breast. She is urgently referred for triple assessment and is diagnosed with invasive ductal carcinoma. Molecular subtyping of the cancer is performed as part of the diagnostic work-up, revealing that she is ER and PR positive, but HER2 negative. What is the most likely treatment for this woman?
Your Answer: Tamoxifen
Correct Answer: Anastrozole
Explanation:Tamoxifen is a targeted therapy used in women with ER+ve breast cancer who are pre- or perimenopausal, while aromatase inhibitors are preferred in those who are postmenopausal. As this patient is postmenopausal, she is most likely to be offered an aromatase inhibitor. Imatinib is a targeted therapy used in chronic myeloid leukaemia, while nivolumab is used in malignant melanoma and renal cell carcinoma, but not breast cancer. Tamoxifen is an oestrogen receptor modulator that inhibits the oestrogen receptor in the breast, making it useful in the targeted treatment of ER+ve breast cancer. It is preferred in pre- and perimenopausal women, while aromatase inhibitors are preferred in postmenopausal women due to the predominant mechanism of oestrogen production.
Breast cancer management varies depending on the stage of the cancer, type of tumor, and patient’s medical history. Treatment options may include surgery, radiotherapy, hormone therapy, biological therapy, and chemotherapy. Surgery is typically the first option for most patients, except for elderly patients with metastatic disease who may benefit more from hormonal therapy. Prior to surgery, an axillary ultrasound is recommended for patients without palpable axillary lymphadenopathy, while those with clinically palpable lymphadenopathy require axillary node clearance. The type of surgery offered depends on various factors, such as tumor size, location, and type. Breast reconstruction is also an option for patients who have undergone a mastectomy.
Radiotherapy is recommended after a wide-local excision to reduce the risk of recurrence, while mastectomy patients may receive radiotherapy for T3-T4 tumors or those with four or more positive axillary nodes. Hormonal therapy is offered if tumors are positive for hormone receptors, with tamoxifen being used in pre- and perimenopausal women and aromatase inhibitors like anastrozole in postmenopausal women. Tamoxifen may increase the risk of endometrial cancer, venous thromboembolism, and menopausal symptoms. Biological therapy, such as trastuzumab, is used for HER2-positive tumors but cannot be used in patients with a history of heart disorders. Chemotherapy may be used before or after surgery, depending on the stage of the tumor and the presence of axillary node disease. FEC-D is commonly used in the latter case.
-
This question is part of the following fields:
- Surgery
-
-
Question 21
Correct
-
A 72-year-old man presents to the emergency department after being referred by his primary care physician due to experiencing abdominal distension and difficulty passing stool or flatus for the past four days. The patient denies any nausea or vomiting, but reports irregular bowel movements with occasional bleeding and recent weight loss. During the examination, tinkling bowel sounds are heard and a digital rectal exam reveals the presence of hard feces. The patient also mentions that his mother had a history of recurrent bowel adhesions requiring multiple surgeries. What is the most probable cause of the patient's symptoms?
Your Answer: Large bowel obstruction
Explanation:The patient’s presentation suggests a large bowel obstruction, as indicated by the abdominal distension, inability to pass stool or flatus, and presence of hard faeces on digital rectal examination. The history of rectal bleeding and weight loss further support this diagnosis. Acute mesenteric ischemia is unlikely due to the absence of severe pain and nausea/vomiting. Paralytic ileus is a possibility, but the presence of bowel sounds suggests a mechanical obstruction. A small bowel obstruction is unlikely given the patient’s family history and lack of vomiting.
Understanding Large Bowel Obstruction
Large bowel obstruction occurs when the passage of food, fluids, and gas through the large intestines is blocked. The most common cause of this condition is a tumor, accounting for 60% of cases. Colonic malignancy is often the initial presenting complaint in approximately 30% of cases, particularly in more distal colonic and rectal tumors. Other causes include volvulus and diverticular disease.
Clinical features of large bowel obstruction include abdominal pain, distention, and absence of passing flatus or stool. Nausea and vomiting may suggest a more proximal lesion, while peritonism may be present if there is associated bowel perforation. It is important to consider the underlying causes, such as any recent symptoms suggestive of colorectal cancer.
Abdominal x-ray is still commonly used as a first-line investigation, with a diameter greater than the normal limits being diagnostic of obstruction. CT scan has a high sensitivity and specificity for identifying obstruction and its underlying cause.
Initial management includes NBM, IV fluids, and nasogastric tube with free drainage. Conservative management for up to 72 hours can be trialed if the cause of obstruction does not require surgery. Around 75% of cases will eventually require surgery. IV antibiotics will be given if perforation is suspected or surgery is planned. Emergency surgery is necessary if there is any overt peritonitis or evidence of bowel perforation, which may involve irrigation of the abdominal cavity, resection of perforated segment and ischaemic bowel, and addressing the underlying cause of the obstruction.
-
This question is part of the following fields:
- Surgery
-
-
Question 22
Incorrect
-
What condition increases the likelihood of developing colon cancer?
Your Answer: Diverticular disease
Correct Answer: Ulcerative colitis
Explanation:Factors that Increase the Risk of Colonic Cancer
Several factors can increase the risk of developing colonic cancer. These include a high-fat, low-fibre diet, being over the age of 50, having a personal history of colorectal adenoma or carcinoma (which increases the risk three-fold), having a first-degree relative with colorectal cancer (also three-fold risk), and having certain genetic conditions such as familial polyposis coli, Gardner syndrome, Turcot syndrome, Juvenile polyposis syndrome, Peutz-Jeghers syndrome, or hereditary non-polyposis colorectal cancer.
In addition, individuals with ulcerative colitis have a 30% risk of developing colonic cancer after 25 years, while those with Crohn’s disease have a four- to 10-fold increased risk. It is important to be aware of these risk factors and to undergo regular screenings for colonic cancer, especially if any of these factors apply to you. By catching the cancer early, it is more likely to be treatable and curable.
-
This question is part of the following fields:
- Surgery
-
-
Question 23
Incorrect
-
A 63-year-old man presents to his GP with a complaint of increasing blood in his urine over the past two weeks. He denies any pain or difficulty while urinating but reports feeling fatigued and possibly losing some weight over the last few months. He has a history of smoking with a 48 pack-year history. On examination, he has a heart rate of 70 bpm, blood pressure of 155/78 mmHg, oxygen saturation of 97% on air, and a temperature of 37.0ºC. There is tenderness in the left renal angle, and a palpable mass is felt on the left side. His abdomen is soft without anterior tenderness. Digital rectal exam reveals a non-enlarged and non-tender prostate. The urine dip results show leucocytes ++, blood +++, protein +, nitrites negative, glucose trace, and ketones negative. What is the most likely diagnosis?
Your Answer: Prostatitis
Correct Answer: Renal cell carcinoma
Explanation:Frank haematuria can be caused by various conditions, including cancer, stones, and infection. However, in this case, the absence of lower urinary tract symptoms and pain makes infection or stones less likely. The patient’s constitutional symptoms and absence of sepsis signs suggest an underlying malignancy. Additionally, the absence of nitrites on the dip test rules out a urinary tract infection. The presence of a ballotable mass and renal angle tenderness is more indicative of renal cell carcinoma than bladder tumour.
Understanding Renal Cell Cancer
Renal cell cancer, also known as hypernephroma, is a primary renal neoplasm that accounts for 85% of cases. It typically arises from the proximal renal tubular epithelium, with the clear cell subtype being the most common. This type of cancer is more prevalent in middle-aged men and is associated with smoking, von Hippel-Lindau syndrome, and tuberous sclerosis. While renal cell cancer is only slightly increased in patients with autosomal dominant polycystic kidney disease, it can present with a classical triad of haematuria, loin pain, and abdominal mass. Other features include pyrexia of unknown origin, endocrine effects, and paraneoplastic hepatic dysfunction syndrome.
The T category criteria for renal cell cancer are based on the size and extent of the tumour. For confined disease, a partial or total nephrectomy may be recommended depending on the tumour size. Patients with a T1 tumour are typically offered a partial nephrectomy, while those with larger tumours may require a total nephrectomy. Treatment options for renal cell cancer include alpha-interferon, interleukin-2, and receptor tyrosine kinase inhibitors such as sorafenib and sunitinib. These medications have been shown to reduce tumour size and treat patients with metastases. It is important to note that renal cell cancer can have paraneoplastic effects, such as Stauffer syndrome, which is associated with cholestasis and hepatosplenomegaly. Overall, early detection and prompt treatment are crucial for improving outcomes in patients with renal cell cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 24
Correct
-
A 62-year-old man presents to the pre-admission clinic for assessment prior to an elective prostatectomy. You find no adverse past medical history and examination is unremarkable. An electrocardiogram (ECG) is indicated in all pre-operative patients undergoing major surgery who are over the age of 60. The ECG is shown below.
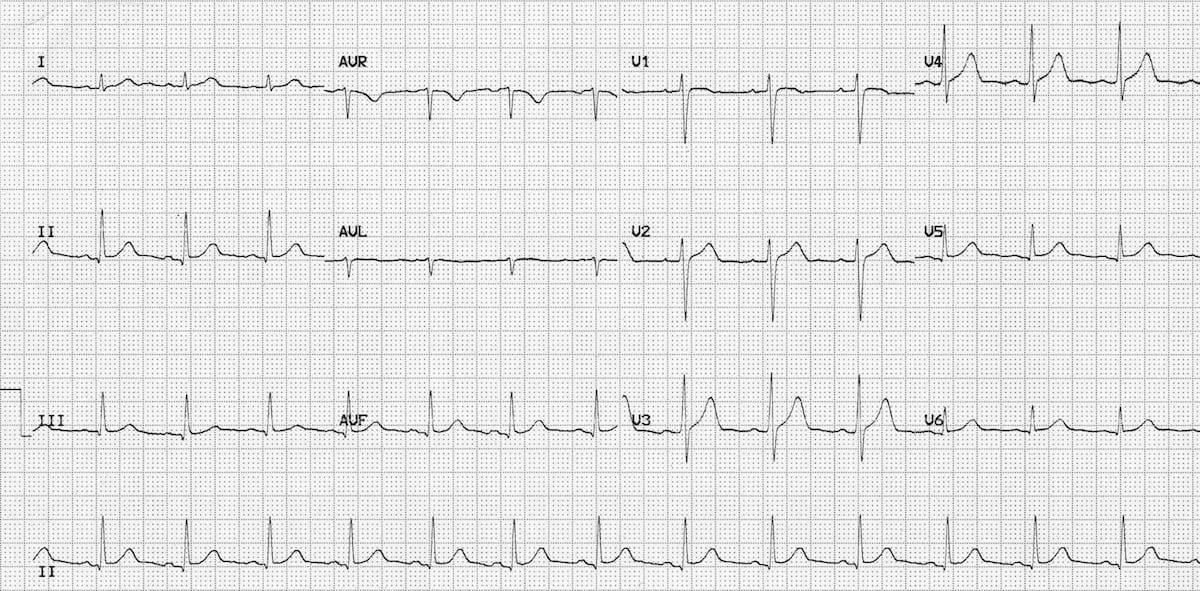 After having reviewed the ECG, what is the next best step to take with this patient?
After having reviewed the ECG, what is the next best step to take with this patient? Your Answer: No further assessment is required
Explanation:Assessing Cardiac Risk in Preoperative Patients: Common Misconceptions
There are several misconceptions when it comes to assessing cardiac risk in preoperative patients. One common mistake is assuming that all patients require extensive cardiac testing, even when there are no significant risk factors or symptoms present. For example, if a patient has no significant past medical history and their examination is unremarkable, an echocardiogram is not necessary.
On the other hand, some clinicians may be too cautious and cancel a patient’s procedure based on a perceived cardiac risk that is not supported by evidence. If the patient’s ECG is normal and there are no cardiac risk factors, cancelling the procedure would be unreasonable.
It is important to recognise that not all preoperative patients require extensive cardiac testing. Instead, clinicians should focus on identifying patients with specific cardiac conditions that require closer monitoring and management. By avoiding unnecessary testing and interventions, clinicians can improve patient outcomes and reduce healthcare costs.
-
This question is part of the following fields:
- Surgery
-
-
Question 25
Correct
-
A 50-year-old man presents with a swollen knee. Upon examination, the knee appears red, hot, and has limited range of motion. The patient has no history of prior surgeries and no significant medical history. What is the most suitable test to rule out a septic joint?
Your Answer: Joint aspiration
Explanation:Diagnosis of Joint Sepsis and Acute Gout
When diagnosing joint sepsis or acute gout, it is important to note that a neutrophilia may not always be present. Additionally, serum uric acid levels can be normal, low, or high in both conditions. While x-rays may show advanced sepsis with bony destruction, they are not always sensitive enough to detect early stages of the condition. An MRI is more sensitive, but the gold standard for diagnosis is joint aspiration. However, it is important to note that joint aspiration should not be performed outside of a theatre if the patient has a prosthetic joint. Proper diagnosis is crucial in order to provide appropriate treatment and prevent further complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 26
Incorrect
-
A 5-year-old boy presents with symptoms of right sided loin pain, lethargy and haematuria. On examination he is pyrexial and has a large mass in the right upper quadrant. What is the most probable underlying diagnosis?
Your Answer: Squamous cell carcinoma of the kidney
Correct Answer: Nephroblastoma
Explanation:Based on the symptoms presented, it is highly probable that the child has nephroblastoma, while perinephric abscess is an unlikely diagnosis. Even if an abscess were to develop, it would most likely be contained within Gerota’s fascia initially, making anterior extension improbable.
Nephroblastoma: A Childhood Cancer
Nephroblastoma, also known as Wilm’s tumours, is a type of childhood cancer that typically occurs in the first four years of life. The most common symptom is the presence of a mass, often accompanied by haematuria (blood in urine). In some cases, pyrexia (fever) may also occur in about 50% of patients. Unfortunately, nephroblastomas tend to metastasize early, usually to the lungs.
The primary treatment for nephroblastoma is nephrectomy, which involves the surgical removal of the affected kidney. The prognosis for younger children is generally better, with those under one year of age having an overall 5-year survival rate of 80%. Early detection and treatment are crucial in improving the chances of survival for children with nephroblastoma.
-
This question is part of the following fields:
- Surgery
-
-
Question 27
Incorrect
-
A 21-year-old motorcyclist is in a road traffic collision. His breathing is irregular. Upon examination, he has multiple rib fractures, including 2 fractures in the 3rd rib and 3 fractures in the 4th rib. What is the underlying condition?
Your Answer: Pneumothorax
Correct Answer: Flail chest injury
Explanation:A flail chest is identified when an individual has multiple rib fractures, with at least two fractures in more than two ribs. This condition is often accompanied by pulmonary contusion.
Thoracic Trauma: Common Conditions and Treatment
Thoracic trauma can result in various conditions that require prompt medical attention. Tension pneumothorax, for instance, occurs when pressure builds up in the thorax due to a laceration to the lung parenchyma with a flap. This condition is often caused by mechanical ventilation in patients with pleural injury. Symptoms of tension pneumothorax overlap with cardiac tamponade, but hyper-resonant percussion note is more likely. Flail chest, on the other hand, occurs when the chest wall disconnects from the thoracic cage due to multiple rib fractures. This condition is associated with pulmonary contusion and abnormal chest motion.
Pneumothorax is another common condition resulting from lung laceration with air leakage. Traumatic pneumothoraces should have a chest drain, and patients should never be mechanically ventilated until a chest drain is inserted. Haemothorax, which is most commonly due to laceration of the lung, intercostal vessel, or internal mammary artery, is treated with a large bore chest drain if it is large enough to appear on CXR. Surgical exploration is warranted if more than 1500 ml blood is drained immediately.
Cardiac tamponade is characterized by elevated venous pressure, reduced arterial pressure, and reduced heart sounds. Pulsus paradoxus may also occur with as little as 100 ml blood. Pulmonary contusion is the most common potentially lethal chest injury, and arterial blood gases and pulse oximetry are important. Early intubation within an hour is necessary if significant hypoxia is present. Blunt cardiac injury usually occurs secondary to chest wall injury, and ECG may show features of myocardial infarction. Aorta disruption, diaphragm disruption, and mediastinal traversing wounds are other conditions that require prompt medical attention.
-
This question is part of the following fields:
- Surgery
-
-
Question 28
Incorrect
-
A 25-year-old motorcyclist is brought into resus after a bike versus lorry road-traffic collision. Following a primary survey, he is believed to have multiple lower limb fractures. He is scheduled for a trauma CT scan. While preparing for transfer to the imaging department, the patient becomes agitated and lashes out at the nurse caring for him. The patient has become more confused and tries to bite the doctor who has attended to review him. A decision is made to intubate the patient to prevent them from causing further self-inflicted injuries.
What medication would be most appropriate to use?Your Answer: Nitrous oxide
Correct Answer: Suxamethonium
Explanation:Understanding Neuromuscular Blocking Drugs
Neuromuscular blocking drugs are commonly used in surgical procedures as an adjunct to anaesthetic agents. These drugs are responsible for inducing muscle paralysis, which is a necessary prerequisite for mechanical ventilation. There are two types of neuromuscular blocking drugs: depolarizing and non-depolarizing.
Depolarizing neuromuscular blocking drugs bind to nicotinic acetylcholine receptors, resulting in persistent depolarization of the motor end plate. On the other hand, non-depolarizing neuromuscular blocking drugs act as competitive antagonists of nicotinic acetylcholine receptors. Examples of depolarizing neuromuscular blocking drugs include succinylcholine (also known as suxamethonium), while examples of non-depolarizing neuromuscular blocking drugs include tubcurarine, atracurium, vecuronium, and pancuronium.
While these drugs are effective in inducing muscle paralysis, they also come with potential adverse effects. Depolarizing neuromuscular blocking drugs may cause malignant hyperthermia and transient hyperkalaemia, while non-depolarizing neuromuscular blocking drugs may cause hypotension. However, these adverse effects can be reversed using acetylcholinesterase inhibitors such as neostigmine.
It is important to note that suxamethonium is contraindicated for patients with penetrating eye injuries or acute narrow angle glaucoma, as it increases intra-ocular pressure. Additionally, suxamethonium is the muscle relaxant of choice for rapid sequence induction for intubation and may cause fasciculations. Understanding the mechanism of action and potential adverse effects of neuromuscular blocking drugs is crucial in ensuring their safe and effective use in surgical procedures.
-
This question is part of the following fields:
- Surgery
-
-
Question 29
Correct
-
A 47-year-old man is scheduled for an elective repair of a left-sided inguinal hernia under general anesthesia. What advice should he be given regarding eating and drinking before the surgery?
Your Answer: No food for 6 hours and no clear fluids for 2 hours before his operation
Explanation:To minimize the risk of pulmonary aspiration of gastric contents, the Royal College of Anaesthetists advises patients to refrain from eating for at least 6 hours prior to the administration of general anesthesia. However, patients are permitted to consume clear fluids, including water, up until 2 hours before the administration of general anesthesia.
Overview of General Anaesthetics
General anaesthetics are drugs used to induce a state of unconsciousness in patients undergoing surgical procedures. There are two main types of general anaesthetics: inhaled and intravenous. Inhaled anaesthetics, such as isoflurane, desflurane, sevoflurane, and nitrous oxide, are administered through inhalation. These drugs work by acting on various receptors in the brain, including GABAA, glycine, NDMA, nACh, and 5-HT3 receptors. Inhaled anaesthetics can cause adverse effects such as myocardial depression, malignant hyperthermia, and hepatotoxicity.
Intravenous anaesthetics, such as propofol, thiopental, etomidate, and ketamine, are administered through injection. These drugs work by potentiating GABAA receptors or blocking NDMA receptors. Intravenous anaesthetics can cause adverse effects such as pain on injection, hypotension, laryngospasm, myoclonus, and disorientation. However, they are often preferred over inhaled anaesthetics in cases of haemodynamic instability.
It is important to note that the exact mechanism of action of general anaesthetics is not fully understood. Additionally, the choice of anaesthetic depends on various factors such as the patient’s medical history, the type of surgery, and the anaesthetist’s preference. Overall, general anaesthetics play a crucial role in modern medicine by allowing for safe and painless surgical procedures.
-
This question is part of the following fields:
- Surgery
-
-
Question 30
Incorrect
-
A 35-year-old woman who is a heavy smoker presents with recurring infections in her right breast. During examination, an indurated area is found at the lateral aspect of the nipple areolar complex. Imaging reveals no mass lesions. What is the probable diagnosis?
Your Answer: Radial scar
Correct Answer: Periductal mastitis
Explanation:Recurrent infections are a common symptom of periductal mastitis in smokers, which can be treated with co-amoxiclav. Additionally, Mondor’s disease of the breast is characterized by a localized thrombophlebitis of a breast vein.
Understanding Mastitis: Inflammation of the Breast Tissue
Mastitis is a condition that refers to the inflammation of the breast tissue, which is commonly associated with breastfeeding. It affects around 1 in 10 women and is characterized by a painful, tender, and red hot breast. Other symptoms may include fever and general malaise.
The first-line management of mastitis is to continue breastfeeding, as simple measures such as analgesia and warm compresses can help alleviate the symptoms. However, if the patient is systemically unwell, has a nipple fissure, or if symptoms do not improve after 12-24 hours of effective milk removal, treatment with antibiotics may be necessary. The first-line antibiotic for mastitis is oral flucloxacillin, which should be taken for 10-14 days. This reflects the fact that the most common organism causing infective mastitis is Staphylococcus aureus.
It is important to note that breastfeeding or expressing should continue during antibiotic treatment. If left untreated, mastitis may develop into a breast abscess, which generally requires incision and drainage. Therefore, it is crucial to seek medical attention if symptoms persist or worsen. Understanding mastitis and its management can help ensure the health and well-being of both the mother and the baby.
-
This question is part of the following fields:
- Surgery
-
-
Question 31
Incorrect
-
A 59-year-old man arrives at the emergency department complaining of severe epigastric pain that is radiating to his right upper quadrant and back. He has vomited three times since the pain started this morning and has never experienced this before. On examination, there is no abdominal distention or visible jaundice. His heart rate is 98/min, respiratory rate 18/min, blood pressure 108/66 mmHg, and temperature 37.9ºC. A new medication has recently been added to his regimen. What is the most probable cause of his presentation?
Your Answer: Methotrexate
Correct Answer: Mesalazine
Explanation:Mesalazine is a potential cause of drug-induced pancreatitis. This medication is commonly prescribed for Crohn’s disease, rheumatoid arthritis, and other conditions as an immunosuppressant. The patient’s symptoms, including epigastric pain radiating to the back, vomiting, low-grade fever, and lack of jaundice, suggest an acute presentation of pancreatitis induced by mesalazine. Although the exact mechanism is unclear, toxicity has been proposed as a possible explanation for mesalazine-induced pancreatitis. While hydroxychloroquine is used to treat systemic lupus erythematosus and rheumatoid arthritis, it is unlikely to cause pancreatitis and may even reduce the risk of this condition. Lithium, a mood stabilizer used to prevent bipolar disorder, has not been associated with pancreatitis. Similarly, metformin, a first-line medication for type 2 diabetes, has not been linked to pancreatitis.
Acute pancreatitis is a condition that is mainly caused by gallstones and alcohol in the UK. A popular mnemonic to remember the causes is GET SMASHED, which stands for gallstones, ethanol, trauma, steroids, mumps, autoimmune diseases, scorpion venom, hypertriglyceridaemia, hyperchylomicronaemia, hypercalcaemia, hypothermia, ERCP, and certain drugs. CT scans of patients with acute pancreatitis show diffuse parenchymal enlargement with oedema and indistinct margins. It is important to note that pancreatitis is seven times more common in patients taking mesalazine than sulfasalazine.
-
This question is part of the following fields:
- Surgery
-
-
Question 32
Incorrect
-
A 52-year-old man presents with haematuria, lethargy, and cough. He smokes 15 cigarettes/day and has COPD.
His heart rate is 89/min, his respiratory rate is 18/min, his blood pressure is 151/93 mmHg and his oxygen saturation is 88%. There is central adiposity with purple striae on the abdomen and a painless 8 cm mass in the left flank.
The blood results are as follows:
Hb 191 Men: 135-180 g/L Women: 115-160 g/L
Na+ 148 135-145 mmol/L
K+ 3.1 3.5 - 5.0 mmol/L
Calcium 3.2 2.1-2.6 mmol/L
The chest x-ray shows areas of low density and flattening of the diaphragm.
What is the most likely diagnosis and what is the definitive treatment?Your Answer: Chemotherapy
Correct Answer: Radical nephrectomy
Explanation:Understanding Renal Cell Cancer
Renal cell cancer, also known as hypernephroma, is a primary renal neoplasm that accounts for 85% of cases. It typically arises from the proximal renal tubular epithelium, with the clear cell subtype being the most common. This type of cancer is more prevalent in middle-aged men and is associated with smoking, von Hippel-Lindau syndrome, and tuberous sclerosis. While renal cell cancer is only slightly increased in patients with autosomal dominant polycystic kidney disease, it can present with a classical triad of haematuria, loin pain, and abdominal mass. Other features include pyrexia of unknown origin, endocrine effects, and paraneoplastic hepatic dysfunction syndrome.
The T category criteria for renal cell cancer are based on the size and extent of the tumour. For confined disease, a partial or total nephrectomy may be recommended depending on the tumour size. Patients with a T1 tumour are typically offered a partial nephrectomy, while those with larger tumours may require a total nephrectomy. Treatment options for renal cell cancer include alpha-interferon, interleukin-2, and receptor tyrosine kinase inhibitors such as sorafenib and sunitinib. These medications have been shown to reduce tumour size and treat patients with metastases. It is important to note that renal cell cancer can have paraneoplastic effects, such as Stauffer syndrome, which is associated with cholestasis and hepatosplenomegaly. Overall, early detection and prompt treatment are crucial for improving outcomes in patients with renal cell cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 33
Incorrect
-
A 80-year-old woman falls during her shopping trip and sustains an injury to her left upper limb. Upon arrival at the Emergency department, an x-ray reveals a fracture of the shaft of her humerus. During the assessment, it is observed that the pulses in her forearm are weak on the side of the fracture. Which artery is most likely to have been affected by the injury?
Your Answer: Radial
Correct Answer: Brachial
Explanation:Brachial Artery Trauma in Humeral Shaft Fractures
The brachial artery, which runs around the midshaft of the humerus, can be affected by trauma when the humeral shaft is fractured. The extent of the damage can vary, from pressure occlusion to partial or complete transection, and may also involve mural contusion with secondary thrombosis. To determine the nature of the damage, an arteriogram should be performed. Appropriate surgery, in combination with fracture fixation, should then be undertaken to address the injury. It is important to promptly assess and treat brachial artery trauma in humeral shaft fractures to prevent further complications and ensure proper healing.
-
This question is part of the following fields:
- Surgery
-
-
Question 34
Incorrect
-
A 68-year-old man visits the oncology clinic after being diagnosed with ER-positive breast cancer. The doctor prescribes anastrozole, an aromatase inhibitor. What is a possible complication that may arise from this treatment?
Your Answer: Venous thromboembolism
Correct Answer: Osteoporosis
Explanation:Before and during treatment, it is important to monitor bone mineral density. AIs do not cause the side effects mentioned. Tamoxifen, a type of SERM, is used to treat ER positive breast cancer in both pre- and postmenopausal women. Adverse effects of tamoxifen include venous thromboembolism, endometrial cancer, cerebral ischaemia, and hypertriglyceridaemia.
Anti-oestrogen drugs are used in the management of oestrogen receptor-positive breast cancer. Selective oEstrogen Receptor Modulators (SERM) such as Tamoxifen act as an oestrogen receptor antagonist and partial agonist. However, Tamoxifen can cause adverse effects such as menstrual disturbance, hot flashes, venous thromboembolism, and endometrial cancer. On the other hand, aromatase inhibitors like Anastrozole and Letrozole reduce peripheral oestrogen synthesis, which is important in postmenopausal women. Anastrozole is used for ER +ve breast cancer in this group. However, aromatase inhibitors can cause adverse effects such as osteoporosis, hot flashes, arthralgia, myalgia, and insomnia. NICE recommends a DEXA scan when initiating a patient on aromatase inhibitors for breast cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 35
Incorrect
-
You are the F2 in general practice. You see a 75-year-old man who is complaining of changes in the appearance of his legs. On examination, you can see areas of brown on the legs, dry skin, and the calves appear significantly wider at the knee than the ankle.
What is the man most at risk of?Your Answer: Arterial ulcers
Correct Answer: Venous ulcers
Explanation:Chronic venous insufficiency is indicated by brown pigmentation (haemosiderin), lipodermatosclerosis (resembling champagne bottle legs), and eczema. These symptoms increase the likelihood of developing venous ulcers, which typically appear above the medial malleolus. Arterial ulcers are more commonly associated with peripheral arterial disease, while neuropathic ulcers are prevalent in individuals with diabetes.
Venous leg ulcers are the most common and are caused by venous hypertension. Arterial ulcers occur on the toes and heel and are painful without palpable pulses. Neuropathic ulcers commonly occur over the plantar surface and can lead to amputation in diabetic patients. Marjolin’s ulcers are squamous cell carcinomas that occur at sites of chronic inflammation. Pyoderma gangrenosum is associated with inflammatory bowel disease and presents as erythematosus nodules or pustules that ulcerate. Management varies depending on the type of ulcer.
-
This question is part of the following fields:
- Surgery
-
-
Question 36
Incorrect
-
A 50-year-old male is recovering on the surgical ward two days post-open inguinal hernia repair. He has no other past medical history of note.
He has not opened his bowels or passed wind for the last 48 hours. His abdomen is diffusely distended and tender. There is no rebound tenderness. There are no bowel sounds on auscultation. He is currently nil by mouth with a nasogastric tube placed.
His observations are as follows:
Respiratory rate 20 breaths per minute
Heart rate 110 beats per minute
Blood pressure 100/60 mmHg
Temperature 37.3ºC
Which of the following investigations is most likely to identify factors which are contributing to this patient's postoperative complication?Your Answer: Endoscopy
Correct Answer: U&Es
Explanation:The patient is experiencing postoperative paralytic ileus, which is evident from her inability to pass gas or have a bowel movement, as well as the absence of bowel sounds during abdominal auscultation. There are several factors that could contribute to the development of an ileus after surgery, including manipulation of the bowel during the procedure, inflammation of the intra-abdominal organs, medications used during and after surgery, and intra-abdominal sepsis. It is likely that a combination of these factors is responsible for the patient’s condition.
Although there are no signs of intra-abdominal sepsis in this patient, it is important to rule out other potential causes, such as electrolyte imbalances or underlying medical conditions. Without more information about the patient’s medical history and medication use, it is difficult to determine the exact cause of the ileus. However, it is recommended that patients with paralytic ileus receive daily monitoring of their electrolyte levels to ensure that any imbalances are promptly corrected.
Postoperative ileus, also known as paralytic ileus, is a common complication that can occur after bowel surgery, particularly if the bowel has been extensively handled. This condition is characterized by a reduction in bowel peristalsis, which can lead to pseudo-obstruction. Symptoms of postoperative ileus include abdominal distention, bloating, pain, nausea, vomiting, inability to pass flatus, and difficulty tolerating an oral diet. It is important to check for deranged electrolytes, such as potassium, magnesium, and phosphate, as they can contribute to the development of postoperative ileus.
The management of postoperative ileus typically involves starting with nil-by-mouth and gradually progressing to small sips of clear fluids. If vomiting occurs, a nasogastric tube may be necessary. Intravenous fluids are administered to maintain normovolaemia, and additives may be used to correct any electrolyte disturbances. In severe or prolonged cases, total parenteral nutrition may be required. It is important to monitor the patient closely and adjust the treatment plan as necessary to ensure a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 37
Correct
-
A 75-year-old woman complains of mild lower back pain and tenderness around the L3 vertebra. Upon conducting tests, the following results were obtained: Hemoglobin levels of 80 g/L (120-160), ESR levels of 110 mm/hr (1-10), and an albumin/globulin ratio of 1:2 (2:1). What is the probable diagnosis?
Your Answer: Multiple myeloma
Explanation:Multiple Myeloma
Multiple myeloma is a type of cancer that affects plasma cells found in the bone marrow. These plasma cells are derived from B lymphocytes, but when they become malignant, they start to divide uncontrollably, forming tumors in the bone marrow. These tumors interfere with normal cell production and erode the surrounding bone, causing soft spots and holes. Since the malignant cells are clones derived from a single plasma cell, they all produce the same abnormal immunoglobulin that is secreted into the blood.
Patients with multiple myeloma may not show any symptoms for many years, but eventually, most patients develop some evidence of the disease. This can include weakened bones, which can cause bone pain and fractures, decreased numbers of red or white blood cells, which can lead to anemia, infections, bleeding, and bruising, and kidney failure, which can cause an increase in creatinine levels. Additionally, destruction of the bone can increase the level of calcium in the blood, leading to symptoms of hypercalcemia. Pieces of monoclonal antibodies, known as light chains or Bence Jones proteins, can also lodge in the kidneys and cause permanent damage. In some cases, an increase in the viscosity of the blood may lead to headaches.
-
This question is part of the following fields:
- Surgery
-
-
Question 38
Incorrect
-
What actions can result in a transverse fracture of the medial malleolus of the tibia?
Your Answer: Dorsiflexion of foot
Correct Answer: Eversion
Explanation:Three Sequential Injuries Caused by Pronated Foot and Abducting Force
The injury mechanism that occurs when a pronated foot experiences an abducting force on the talus can result in up to three sequential injuries. The first injury is a transverse fracture of the medial malleolus, which is caused by a tense deltoid ligament. The second injury occurs when the abducting talus stresses the tibiofibular syndesmosis, resulting in a tear of the anterior tibiofibular ligament. Finally, continued abduction of the talus can lead to an oblique fracture of the distal fibula.
This sequence of injuries can be quite serious and may require medical attention. It is important to be aware of the potential risks associated with a pronated foot and to take steps to prevent injury. This may include wearing appropriate footwear, using orthotics or other supportive devices, and avoiding activities that put excessive stress on the foot and ankle. By taking these precautions, individuals can reduce their risk of experiencing these types of injuries and maintain their overall health and well-being.
-
This question is part of the following fields:
- Surgery
-
-
Question 39
Incorrect
-
A young laborer presents to the Emergency department with complaints of pain in their middle finger. Upon examination, the finger appears swollen and is held in a partially flexed position. Passive extension elicits pain and there is tenderness over the flexor sheath. What is the probable diagnosis?
Your Answer: Dupuytren's contracture
Correct Answer: Suppurative flexor tenosynovitis
Explanation:The Four Cardinal Signs of Suppurative Flexor Tenosynovitis
Suppurative flexor tenosynovitis is a serious infection that affects the tendons and synovial sheaths of the fingers. Kanavel, a renowned physician, identified four cardinal signs of this condition. The first sign is a flexed posture, which is caused by pain and swelling in the affected area. The second sign is fusiform swelling, which refers to a sausage-like swelling of the finger. The third sign is pain on passive extension, which means that the finger hurts when it is straightened. The fourth sign is flexor sheath tenderness, which is tenderness along the tendon sheath.
Deep potential space infections, such as mid palmar and thenar space infections, are made worse by flexion. This is because flexion causes the infected area to become more compressed, which can lead to further swelling and pain. It is important to recognize these cardinal signs of suppurative flexor tenosynovitis and seek medical attention immediately if they are present. Early diagnosis and treatment can help prevent serious complications, such as loss of function or even amputation.
-
This question is part of the following fields:
- Surgery
-
-
Question 40
Incorrect
-
A 39-year-old man is being evaluated on the orthopaedic ward for fever and difficulty breathing. He underwent intramedullary nail surgery to repair a fracture in his right tibia a week ago. What is the probable reason for his pyrexia that occurred more than 5 days after the operation?
Your Answer: Blood transfusion
Correct Answer: Venous thromboembolism
Explanation:Venous thromboembolism typically manifests itself between 5 to 10 days after surgery. The presence of breathlessness increases the likelihood of a diagnosis of venous thromboembolism as opposed to cellulitis or urinary tract infection. Meanwhile, pulmonary atelectasis is more prone to occur in the earlier stages following surgery.
Post-operative pyrexia, or fever, can occur after surgery and can be caused by various factors. Early causes of post-op pyrexia, which typically occur within the first five days after surgery, include blood transfusion, cellulitis, urinary tract infection, and a physiological systemic inflammatory reaction that usually occurs within a day following the operation. Pulmonary atelectasis is also often listed as an early cause, but the evidence to support this link is limited. Late causes of post-op pyrexia, which occur more than five days after surgery, include venous thromboembolism, pneumonia, wound infection, and anastomotic leak.
To remember the possible causes of post-op pyrexia, it is helpful to use the memory aid of the 4 W’s: wind, water, wound, and what did we do? (iatrogenic). This means that the causes can be related to respiratory issues (wind), urinary tract or other fluid-related problems (water), wound infections or complications (wound), or something that was done during the surgery or post-operative care (iatrogenic). It is important to identify the cause of post-op pyrexia and treat it promptly to prevent further complications. This information is based on a peer-reviewed publication available on the National Center for Biotechnology Information website.
-
This question is part of the following fields:
- Surgery
-
-
Question 41
Incorrect
-
An 81-year-old man has fallen off his bike and hit his head. His friend at the scene reports that he was unconscious for less than a minute. The man was cycling slowly on a path beside a canal. Upon initial assessment, he has some bruising on his upper and lower limbs, a Glasgow coma score (GCS) of 15, and no neurological deficit. He has not experienced vomiting or seizures since the accident and was able to describe the incident. He takes antihypertensives but has no significant medical history. What would be the most appropriate next step?
Your Answer: Discharge the patient and tell him to return if further symptoms develop
Correct Answer: Perform a CT head scan within 8 hours
Explanation:When it comes to detecting significant brain injuries in the acute setting, CT imaging of the head is currently the preferred method of investigation. MRI is not typically used due to safety concerns, logistical challenges, and resource limitations.
According to NICE guidelines, patients over the age of 65 who experience a head injury resulting in loss of consciousness or amnesia should undergo a CT head scan within 8 hours. However, if there is an indication for a CT head scan within 1 hour, that should take priority. The specific indications for CT head scans within 1 hour and 8 hours can be found below.
Reference:
NICE (2014): Head injury: assessment and early management.NICE Guidelines for Investigating Head Injuries in Adults
Head injuries can be serious and require prompt medical attention. The National Institute for Health and Care Excellence (NICE) has provided clear guidelines for healthcare professionals to determine which adult patients need further investigation with a CT head scan. Patients who require immediate CT head scans include those with a Glasgow Coma Scale (GCS) score of less than 13 on initial assessment, suspected open or depressed skull fractures, signs of basal skull fractures, post-traumatic seizures, focal neurological deficits, and more than one episode of vomiting.
For patients with any loss of consciousness or amnesia since the injury, a CT head scan within 8 hours is recommended for those who are 65 years or older, have a history of bleeding or clotting disorders, experienced a dangerous mechanism of injury, or have more than 30 minutes of retrograde amnesia of events immediately before the head injury. Additionally, patients on warfarin who have sustained a head injury without other indications for a CT head scan should also receive a scan within 8 hours of the injury.
It is important for healthcare professionals to follow these guidelines to ensure that patients receive appropriate and timely care for their head injuries. By identifying those who require further investigation, healthcare professionals can provide the necessary treatment and support to prevent further complications and improve patient outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 42
Incorrect
-
A 65-year-old male presents to the emergency department with a 2-day history of worsening upper abdominal pain, accompanied by nausea and vomiting. The pain is exacerbated by meals, and he is unable to tolerate oral intake.
Upon examination, the patient appears distressed and in pain. His vital signs are as follows:
Temperature: 38.2 ℃
Heart rate: 110 beats/minute
Respiratory rate: 20/min
Blood pressure: 130/90 mmHg
Oxygen saturation: 98% on room air
There is tenderness in the right upper quadrant of his abdomen, but no distension, guarding, or rigidity on light palpation. Murphy's sign is negative. The sclera of his eyes has a yellow tinge.
Blood lab results are as follows:
Hb 130 g/L Male: (135-180)
Female: (115 - 160)
Platelets 180 * 109/L (150 - 400)
WBC 15 * 109/L (4.0 - 11.0)
Bilirubin 30 µmol/L (3 - 17)
ALP 360 u/L (30 - 100)
ALT 40 u/L (3 - 40)
γGT 50 u/L (8 - 60)
Albumin 38 g/L (35 - 50)
An ultrasound of the right upper quadrant reveals dilated intrahepatic and extrahepatic bile ducts and multiple hyperechoic spheres within the gallbladder. The patient is started on IV antibiotics and fluid resuscitation, but his condition remains critical.
What is the most appropriate next step in management?Your Answer: Magnetic retrograde cholangiopancreatography (MRCP)
Correct Answer: Endoscopic retrograde cholangiopancreatography (ERCP)
Explanation:Ascending cholangitis patients are typically recommended to undergo ERCP within 24-48 hours of diagnosis to alleviate any obstructions. This patient displays Charcot’s triad, leukocytosis, and elevated markers of cholestasis, as well as an ultrasound confirming acute ascending cholangitis. ERCP is the preferred treatment for acute cholangitis, with elective ERCP being performed after clinical improvement in mild cases and immediate ERCP in severe cases. While MRCP can assess biliary tree obstructions, it does not provide therapeutic drainage. Laparoscopic cholecystectomy is not recommended for septic patients and is only indicated once sepsis has been resolved, as it does not remove gallstones in the common bile duct.
Understanding Ascending Cholangitis
Ascending cholangitis is a bacterial infection that affects the biliary tree, with E. coli being the most common culprit. This condition is often associated with gallstones, which can predispose individuals to the infection. Patients with ascending cholangitis may present with Charcot’s triad, which includes fever, right upper quadrant pain, and jaundice. However, this triad is only present in 20-50% of cases. Other common symptoms include hypotension and confusion. In severe cases, Reynolds’ pentad may be observed, which includes the additional symptoms of hypotension and confusion.
To diagnose ascending cholangitis, ultrasound is typically used as a first-line investigation to look for bile duct dilation and stones. Raised inflammatory markers may also be observed. Treatment involves intravenous antibiotics and endoscopic retrograde cholangiopancreatography (ERCP) after 24-48 hours to relieve any obstruction.
Overall, ascending cholangitis is a serious condition that requires prompt diagnosis and treatment. Understanding the symptoms and risk factors associated with this condition can help individuals seek medical attention early and improve their chances of a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 43
Incorrect
-
A 65-year-old woman undergoes a right hemicolectomy for colon cancer and four days later presents with vomiting, a distended abdomen, and absent bowel sounds. Her blood results show a CRP of 124 mg/l and a WBC count of 5.2 * 109/l. Nursing notes reveal no bowel movements since surgery. What is the probable cause of her clinical presentation?
Your Answer:
Correct Answer: Paralytic ileus
Explanation:Simple constipation is unlikely in this patient due to the presence of vomiting and absent bowel sounds, which suggests paralytic ileus, especially so soon after surgery. Additionally, constipation alone would not explain all of the patient’s symptoms and signs. As the patient underwent a right hemicolectomy, the caecum would have been removed, making caecal volvulus an unlikely diagnosis. The raised CRP is a normal response to surgery. While peritonitis is a possibility, it would typically present with severe abdominal pain, tenderness, guarding, and more significantly elevated inflammatory markers and fever. Hirschsprung’s disease, a congenital condition, is highly unlikely to present for the first time in a 67-year-old patient.
Postoperative ileus, also known as paralytic ileus, is a common complication that can occur after bowel surgery, particularly if the bowel has been extensively handled. This condition is characterized by a reduction in bowel peristalsis, which can lead to pseudo-obstruction. Symptoms of postoperative ileus include abdominal distention, bloating, pain, nausea, vomiting, inability to pass flatus, and difficulty tolerating an oral diet. It is important to check for deranged electrolytes, such as potassium, magnesium, and phosphate, as they can contribute to the development of postoperative ileus.
The management of postoperative ileus typically involves starting with nil-by-mouth and gradually progressing to small sips of clear fluids. If vomiting occurs, a nasogastric tube may be necessary. Intravenous fluids are administered to maintain normovolaemia, and additives may be used to correct any electrolyte disturbances. In severe or prolonged cases, total parenteral nutrition may be required. It is important to monitor the patient closely and adjust the treatment plan as necessary to ensure a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 44
Incorrect
-
A thirty-five-year-old man with ulcerative colitis is recovering on the ward 6 days following a proctocolectomy. During the morning ward round, he complains to the team looking after him that he has developed pain in his abdomen. The pain started in the left iliac fossa but is now diffuse. It came on suddenly, overnight, and has gradually been getting worse since. He ranks it 9/10. He has not opened his bowels or passed flatus since the procedure. He has had no analgesia for this.
On examination:
Blood pressure: 105/68 mmHg;
Heart rate: 118/minute, regular;
Respiratory rate: 12/minute;
Temperature: 38.2 ºC;
Oxygen saturations: 98%.
Abdominal exam: abdomen is distended and diffusely tender upon palpation and widespread guarding, indicating peritonism. No organomegaly or palpable abdominal aortic aneurysm. Kidneys are non-ballotable. No shifting dullness. Bowel sounds are absent.
There is 250 mL of feculent matter in the abdominal wound drain.
The registrar requests an abdominal CT which demonstrates an anastomotic leak. What is the most appropriate initial management of this patient?Your Answer:
Correct Answer: Call the consultant to come in and take the patient to theatre immediately
Explanation:In the case of a confirmed anastomotic leak, immediate surgical intervention is necessary and the patient must be taken back to the operating room without delay. Administering only paracetamol or intravenous antibiotics would not be sufficient as these measures do not address the underlying problem.
Complications can occur in all types of surgery and require vigilance in their detection. Anticipating likely complications and appropriate avoidance can minimize their occurrence. Understanding the anatomy of a surgical field will allow appreciation of local and systemic complications that may occur. Physiological and biochemical derangements may also occur, and appropriate diagnostic modalities should be utilized. Safe and timely intervention is the guiding principle for managing complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 45
Incorrect
-
An 80-year-old man presents to the emergency department with urinary retention. Upon examination, a catheter is inserted and 900 ml of residual urine is drained. The patient also complains of upper back pain over the spinal vertebrae. The patient has a history of metastatic prostate cancer and has recently started treatment. What type of prostate cancer treatment is the patient likely receiving?
Your Answer:
Correct Answer: Goserelin (GnRH agonist)
Explanation:Starting management for metastatic prostate cancer with GnRH agonists may lead to a phenomenon called tumour flare, which can cause bone pain, bladder obstruction, and other symptoms. This was observed in a 78-year-old man who presented with urinary retention and bone pain after recently starting treatment. GnRH agonists work by overstimulating the hormone cascade to suppress testosterone production, which initially causes an increase in testosterone levels before subsequent suppression. Bicalutamide is not the best answer as it does not cause the testosterone surge seen with GnRH agonist use. Bilateral orchidectomy is not typically associated with tumour flare as it aims to rapidly decrease testosterone levels. GnRH antagonists, such as degarelix, may be a better option as they avoid the risk of tumour flare by avoiding the testosterone surge.
Management of Prostate Cancer
Localised prostate cancer (T1/T2) can be managed through various treatment options depending on the patient’s life expectancy and preference. Conservative approaches such as active monitoring and watchful waiting can be considered, as well as radical prostatectomy and radiotherapy (external beam and brachytherapy). On the other hand, localised advanced prostate cancer (T3/T4) may require hormonal therapy, radical prostatectomy, or radiotherapy. However, patients who undergo radiotherapy may develop proctitis and are at a higher risk of bladder, colon, and rectal cancer.
For metastatic prostate cancer, the primary goal is to reduce androgen levels. A combination of approaches is often used, including anti-androgen therapy, synthetic GnRH agonist or antagonists, bicalutamide, cyproterone acetate, abiraterone, and bilateral orchidectomy. GnRH agonists such as Goserelin (Zoladex) may result in lower LH levels longer term by causing overstimulation, which disrupts endogenous hormonal feedback systems. This may cause a rise in testosterone initially for around 2-3 weeks before falling to castration levels. To prevent a rise in testosterone, anti-androgen therapy is often used initially. However, this may result in a tumour flare, which stimulates prostate cancer growth and may cause bone pain, bladder obstruction, and other symptoms. GnRH antagonists such as degarelix are being evaluated to suppress testosterone while avoiding the flare phenomenon. Chemotherapy with docetaxel may also be an option for the treatment of hormone-relapsed metastatic prostate cancer in patients who have no or mild symptoms after androgen deprivation therapy has failed, and before chemotherapy is indicated.
-
This question is part of the following fields:
- Surgery
-
-
Question 46
Incorrect
-
A 54-year-old woman presents to the Emergency Department with sudden onset upper abdominal pain radiating to the back. She reports experiencing similar pain in the past, especially after eating, but this episode is the most severe. Her medical history includes type 2 diabetes mellitus, chronic kidney disease (CKD), and hypercholesterolemia. She does not smoke or drink alcohol. On examination, there is tenderness to palpation of the epigastrium. Blood tests are ordered, and the results are as follows:
- Bilirubin: 28 µmol/L (3 - 17)
- ALP: 321 µmol/L (30 - 100)
- AST: 93 iu/L (3 - 30)
- Amylase: 1090 u/L (70 - 300)
- Calcium: 1.92 mmol/L (2.1 - 2.6)
What is the most appropriate next step in investigating the likely cause of her symptoms?Your Answer:
Correct Answer: Transabdominal ultrasound
Explanation:In cases of acute pancreatitis, early ultrasound imaging is crucial in determining the underlying cause, as this can impact the course of treatment. For instance, if the patient has gallstones or biliary obstruction, management may involve cholecystectomy to prevent future attacks of pancreatitis or biliary sepsis. In this patient’s case, her symptoms and laboratory results suggest gallstones as the likely cause of her acute pancreatitis. Therefore, an ultrasound scan is recommended as the first-line investigation to confirm the presence of gallstones and identify any biliary involvement. Blood cultures are not necessary in the absence of signs of infection or sepsis. Contrast-enhanced CT may be used if there is diagnostic uncertainty, but given the patient’s history of CKD, it may not be the most appropriate option. Endoscopic ultrasound may be considered if MRCP is inconclusive, but MRCP is only recommended if abdominal ultrasound has not detected gallstones.
Understanding Acute Pancreatitis
Acute pancreatitis is a condition that is commonly caused by alcohol or gallstones. It occurs when the pancreatic enzymes start to digest the pancreatic tissue, leading to necrosis. The main symptom of acute pancreatitis is severe epigastric pain that may radiate through to the back. Vomiting is also common, and examination may reveal epigastric tenderness, ileus, and low-grade fever. In rare cases, periumbilical discolouration (Cullen’s sign) and flank discolouration (Grey-Turner’s sign) may be present.
To diagnose acute pancreatitis, doctors typically measure the levels of serum amylase and lipase in the blood. While amylase is raised in 75% of patients, it does not correlate with disease severity. Lipase, on the other hand, is more sensitive and specific than amylase and has a longer half-life. Imaging tests, such as ultrasound and contrast-enhanced CT, may also be used to assess the aetiology of the condition.
Scoring systems, such as the Ranson score, Glasgow score, and APACHE II, are used to identify cases of severe pancreatitis that may require intensive care management. Factors that indicate severe pancreatitis include age over 55 years, hypocalcaemia, hyperglycaemia, hypoxia, neutrophilia, and elevated LDH and AST. It is important to note that the actual amylase level is not of prognostic value.
In summary, acute pancreatitis is a condition that can cause severe pain and discomfort. It is typically caused by alcohol or gallstones and can be diagnosed through blood tests and imaging. Scoring systems are used to identify cases of severe pancreatitis that require intensive care management.
-
This question is part of the following fields:
- Surgery
-
-
Question 47
Incorrect
-
A 58-year-old male presents to the emergency department with a sudden and severe occipital headache accompanied by two episodes of vomiting within the last hour. Despite a normal CT scan, a lumbar puncture taken 12 hours later reveals xanthochromia, leading to a diagnosis of subarachnoid hemorrhage (SAH). Urgent neurosurgical consultation is requested, and a CT cerebral angiography confirms a posterior communicating artery aneurysm as the underlying cause of the SAH. The patient is otherwise healthy. What is the most suitable treatment option for the aneurysm?
Your Answer:
Correct Answer: Coiling by an interventional neuroradiologist
Explanation:After a subarachnoid haemorrhage, urgent intervention is necessary for intracranial aneurysms due to the risk of rebleeding. The most common treatment for this is coiling by an interventional neuroradiologist, which involves inserting soft metallic coils into the aneurysm to exclude it from intracranial circulation. This is less invasive than surgical clipping. While nimodipine is used to reduce vasospasm following a SAH, it is not sufficient on its own and additional intervention is required. Typically, nimodipine is administered for 21 days and targets the brain vasculature by inhibiting calcium channels.
A subarachnoid haemorrhage (SAH) is a type of bleeding that occurs within the subarachnoid space of the meninges in the brain. It can be caused by head injury or occur spontaneously. Spontaneous SAH is often caused by an intracranial aneurysm, which accounts for around 85% of cases. Other causes include arteriovenous malformation, pituitary apoplexy, and mycotic aneurysms. The classic symptoms of SAH include a sudden and severe headache, nausea and vomiting, meningism, coma, seizures, and ECG changes.
The first-line investigation for SAH is a non-contrast CT head, which can detect acute blood in the basal cisterns, sulci, and ventricular system. If the CT is normal within 6 hours of symptom onset, a lumbar puncture is not recommended. However, if the CT is normal after 6 hours, a lumbar puncture should be performed at least 12 hours after symptom onset to check for xanthochromia and other CSF findings consistent with SAH. If SAH is confirmed, referral to neurosurgery is necessary to identify the underlying cause and provide urgent treatment.
Management of aneurysmal SAH involves supportive care, such as bed rest, analgesia, and venous thromboembolism prophylaxis. Vasospasm is prevented with oral nimodipine, and intracranial aneurysms require prompt intervention to prevent rebleeding. Most aneurysms are treated with a coil by interventional neuroradiologists, but some require a craniotomy and clipping by a neurosurgeon. Complications of aneurysmal SAH include re-bleeding, hydrocephalus, vasospasm, and hyponatraemia. Predictive factors for SAH include conscious level on admission, age, and amount of blood visible on CT head.
-
This question is part of the following fields:
- Surgery
-
-
Question 48
Incorrect
-
What is the probable diagnosis for a 24-year-old man who twisted his knee during a football match, continued to play, but now experiences increasing pain, swelling, and intermittent locking two days later?
Your Answer:
Correct Answer: Medial meniscus tear
Explanation:Meniscus Injuries
The meniscus is a type of cartilage that serves as a cushion between the bones in the knee joint. It helps absorb shock and prevents the bones from rubbing against each other. However, it is susceptible to injury, usually caused by a collision or deep knee bends. Symptoms of a meniscus tear include pain along the joint line or throughout the knee, as well as an inability to fully extend the knee. This can cause the knee to feel like it is locking and may also result in swelling.
While some minor meniscus tears may heal on their own with rest, more serious injuries often require surgery. It is important to note that a meniscus tear may also be associated with other knee injuries, such as an anterior cruciate ligament (ACL) or medial collateral ligament injury.
-
This question is part of the following fields:
- Surgery
-
-
Question 49
Incorrect
-
A 65-year-old man visited his doctor complaining of painless haematuria that had been occurring on and off for three months. He has a past medical history of COPD and IHD, and has smoked 25 packs of cigarettes per year for the past 40 years. Upon examination, no abnormalities were found. However, a urine dipstick test revealed 3+ blood. What is the probable diagnosis?
Your Answer:
Correct Answer: Bladder transitional cell carcinoma
Explanation:Bladder cancer typically presents with painless haematuria, which requires referral to a urology haematuria clinic. Approximately 5-10% of microscopic haematuria and 20-25% of frank haematuria will have a urogenital malignancy. Tests carried out in the haematuria clinic include urine analysis, cytology, cystoscopy, and ultrasound. Transitional cell carcinoma is the most common type of bladder cancer, and smoking increases the risk by threefold. Bladder stones and urinary tract infections may also cause bladder irritation and haematuria.
-
This question is part of the following fields:
- Surgery
-
-
Question 50
Incorrect
-
A 25-year-old male patient visits his GP with concerns about a lump in his right testicle. He reports no other symptoms and has no significant medical or family history. Upon examination, a firm, distinct nodule is detected on the lateral aspect of the right testicle that does not trans-illuminate, while the left testicle appears normal. The physician suspects testicular cancer and orders serological tumour markers and an ultrasound investigation. What is a possible association with the probable diagnosis?
Your Answer:
Correct Answer: Gynaecomastia
Explanation:The most common tumor marker for testicular cancer is alpha-fetoprotein (AFP), which is elevated in non-seminomas and may be normal or elevated in seminomas. However, it is not typically decreased in any type of tumor. Galactorrhea is not a typical symptom of testicular cancer, although gynecomastia is often associated with it.
Understanding Testicular Cancer
Testicular cancer is a type of cancer that commonly affects men between the ages of 20 and 30. Germ-cell tumors are the most common type of testicular cancer, accounting for around 95% of cases. These tumors can be divided into seminomas and non-seminomas, which include embryonal, yolk sac, teratoma, and choriocarcinoma. Other types of testicular cancer include Leydig cell tumors and sarcomas. Risk factors for testicular cancer include infertility, cryptorchidism, family history, Klinefelter’s syndrome, and mumps orchitis.
The most common symptom of testicular cancer is a painless lump, although some men may experience pain. Other symptoms may include hydrocele and gynaecomastia, which occurs due to an increased oestrogen:androgen ratio. Tumor markers such as hCG, AFP, and beta-hCG may be elevated in germ cell tumors. Ultrasound is the first-line diagnostic tool for testicular cancer.
Treatment for testicular cancer depends on the type and stage of the tumor. Orchidectomy, chemotherapy, and radiotherapy may be used. Prognosis for testicular cancer is generally excellent, with a 5-year survival rate of around 95% for seminomas and 85% for teratomas if caught at Stage I. It is important for men to perform regular self-examinations and seek medical attention if they notice any changes or abnormalities in their testicles.
-
This question is part of the following fields:
- Surgery
-
00
Correct
00
Incorrect
00
:
00
:
0
00
Session Time
00
:
00
Average Question Time (
Mins)