-
Question 1
Incorrect
-
Which one of the following statements regarding fetal blood pH is correct?
Your Answer: pH 6.9 is considered to be normal
Correct Answer: Can be measured during labour
Explanation:A sample for fetal blood pH can be taken during the labour. The mother should be lying in a left lateral position.
-
This question is part of the following fields:
- Physiology
-
-
Question 2
Correct
-
A 21 year old married gravida 1 para 1 has not used her oral contraceptives for 6 months. She comes to your office for evaluation because her menstrual period is 2 weeks late. Her menses had been regular since discontinuing the oral contraceptives. A urine hCG is negative. Which one of the following is true regarding this situation?
Your Answer: It is unlikely that she is pregnant
Explanation:With the high level of sensitivity and specificity of current tests to measure hCG in serum and urine, pregnancy can now be diagnosed before the time of the first missed menstrual period- For current serum hCG assays, the low threshold for detection is 10-25 IU/L, while for urine assays it is 25-50 IU/L, which corresponds to approximately the seventh day after conception. Because the levels of hCG in the blood and urine are very similar, the tests are equivalent. Urine testing may reveal a positive result as early as 3-4 days after implantation. By the time of the expected menstrual period, the test will be positive 98% of the time- If a test is negative more than 1 week after the expected time of the menstrual period, it is almost certain the patient is not pregnant. To cover these rare instances where a woman has a low hCG and conceived later than expected, the test should be repeated in 1 week for a definitive result.
Since ectopic pregnancy is not a life-threatening problem for the mother until 2 months after conception, a patient with a negative urine hCG does not require ultrasonography to exclude ectopic pregnancy. Patients with a suspected ectopic pregnancy and a negative urine hCG should be followed closely, as early laparoscopic intervention can improve the chances of future fertility.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 3
Correct
-
A 61 year old patient undergoes laparotomy for a suspicious left sided ovarian mass. Following histology the patient is diagnosed with a stage 1A ovarian epithelial cancer. What is the 5 year survival for stage 1 ovarian cancers?
Your Answer: 90%
Explanation:The five year survival of stage 1 ovarian cancer is 70-90%
-
This question is part of the following fields:
- Epidemiology
-
-
Question 4
Correct
-
A 28 year old patient presents to clinic with a maculopapular rash to the hands and soles of the feet. Examination reveals wart like lesions on the vagina and a diagnosis of condyloma latum is made. What stage of syphilis infection is this?
Your Answer: Secondary
Explanation:Condylomas are warty neoplasms of the vulvar area. The most common type are condyloma acuminatum which occur due to HPV 6 or 11. Condyloma latum are also known as secondary syphilis are less common. Both of these are sexually transmitted.
Stages of Syphilis:
– Primary 3-90 days
Chancre and lymphadenopathy
– Secondary 4-10 weeks
Widespread rash typically affecting hands and soles of feet.
Wart lesions (condyloma latum) of mucus membranes
– Latent Early <1 yr. after secondary stage
– Late >2 yr. after secondary stage
Asymptomatic
– Tertiary 3+ years after primary infection
Gummas or
Neurosyphilis or
Cardiovascular syphilis -
This question is part of the following fields:
- Clinical Management
-
-
Question 5
Incorrect
-
A 30-year-old female patient visits you for a cervical cancer screening. You inform her that while Pap smears are no longer performed, Cervical Screening tests are done five times a year. She has a cervical screening test, which reveals that she has non-16/18 HPV and low-grade cytology alterations. What's would you do next?
Your Answer: Repeat cervical screening test in 5 years
Correct Answer: Repeat cervical screening test in 12 months
Explanation:An LSIL Pap test shows mild cellular changes. The risk of a high-grade cervical precancer or cancer after an LSIL Pap test is as high as 19 percent.
As with an ASC-US Pap test, an LSIL Pap test is evaluated differently depending upon age. For women ages 25 or older, follow-up depends upon the results of human papillomavirus (HPV) testing:
– Women who test positive for HPV or who have not been tested for HPV should have colposcopy.
– Women who test negative for HPV can be followed up with a Pap test and HPV test in one year.Referral to an oncologist is not necessary since there is no established diagnosis of malignancy. All other options are unacceptable.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 6
Incorrect
-
A 30-year-old primigravida woman presented to the clinic for her first antenatal check-up. Upon interview, it was noted that she was taking folic acid along with some other nutritional supplements as medication. All of the following are considered correct regarding neural tube defects and folate before and during pregnancy, except:
Your Answer: Women with a family history of neural tube defects need more folate before and during pregnancy
Correct Answer: Prevalence of neural tube defects among non-indigenous population is almost double than that in Aboriginal and Torres Strait Islander babies
Explanation:Neural tube defects (NTDs) are common complex congenital malformations resulting from failure of the neural tube closure during embryogenesis. It is established that folic acid supplementation decreases the prevalence of NTDs, which has led to national public health policies regarding folic acid.
Neural tube defects (NTD) were 43% more common in Indigenous than in non-Indigenous infants in Western Australia in the 1980s, and there has been a fall in NTD overall in Western Australia since promotion of folate and voluntary fortification of food has occurred.
Women should take 5 mg/d of folic acid for the 2 months before conception and during the first trimester.
Women planning pregnancy might be exposed to medications with known antifolate activities affecting different parts of the folic acid metabolic cascade. A relatively large number of epidemiologic studies have shown an increased risk of NTDs among babies exposed in early gestation to antiepileptic drugs (carbamazepine, valproate, barbiturates), sulphonamides, or methotrexate. Hence, whenever women use these medications, or have used them near conception, they should take 5 mg/d of folic acid until the end of the first trimester of pregnancy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 7
Incorrect
-
What is the typical weight of a non-pregnant premenopausal uterus?
Your Answer: 1200g
Correct Answer: 40g
Explanation:Uterine blood flow increases 40-fold to approximately 700 mL/min at term, with 80 per cent of the blood. The uterus is 50–60 g prior to pregnancy and 1000 g by term. The volume increases from 10 ml to 5000ml approx. It is around 40g at menopause.
-
This question is part of the following fields:
- Physiology
-
-
Question 8
Correct
-
A 26-year-old pregnant female in her first trimester was brought to the labour room with complaints of painless vaginal bleeding. On examination, her abdomen was non-tender and os was closed. Which of the following is the most likely diagnosis?
Your Answer: Threatened miscarriage
Explanation:Threatened miscarriage is a term used to describe any abnormal vaginal bleeding that occurs in first trimester, sometime associated with abdominal cramps. The cervix remains closed and the pregnancy may continue as normal.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 9
Incorrect
-
A 22-year-old nulliparous otherwise healthy woman presents with lower abdominal pain at 16 weeks of gestation. Her body temperature is 37.8 degrees Celsius. She appears to be in good health and is eating properly. Her uterus had been discovered to be retroverted but of normal size at her prior antenatal check at 11 weeks of pregnancy. Which of the following diagnoses is the most likely?
Your Answer: Impaction of a retroverted gravid uterus.
Correct Answer: Urinary tract infection.
Explanation:Lower abdominal pain can be caused by any of the conditions listed in the answers.
A urinary tract infection is the most likely cause.
Unless it was an abdominal ectopic or an interstitial pregnancy, an ectopic pregnancy.
will almost definitely have shown up before the 15th week of pregnancy.
A retroverted gravid uterus may impinge at 15 weeks of pregnancy, however, this is unlikely to be linked to a temperature of 37.8°C.
It’s also possible that it’s the source of acute urine retention.
Complications of the corpus luteum cyst normally manifest themselves considerably earlier in pregnancy, and severe appendicitis is far less likely to be the source of discomfort than a urinary tract infection. -
This question is part of the following fields:
- Obstetrics
-
-
Question 10
Incorrect
-
Question 11
Incorrect
-
A pregnant patient with a chest infection is worried about the radiation risk of a chest X Ray. How many days of natural background radiation is equivalent to a chest X Ray?
Your Answer: 7
Correct Answer: 2.5
Explanation:X-rays carry low levels of risk during pregnancy and are not a significant cause for concern if the total exposure to ionising radiation is less than 5 rads throughout the pregnancy; a chest X-ray is about 0.00007 rads. The amount of radiation generated from a chest X-ray is equivalent to 2.4 days of natural background radiation. Non-urgent radiological tests should, however, be avoided between 10-17 weeks gestation as there is a higher risk of central nervous system teratogenesis during this time.
-
This question is part of the following fields:
- Biophysics
-
-
Question 12
Correct
-
Which one of the following statements regarding the fetal head is true?
Your Answer: Considered to be engaged when the biparietal diameter passes the level of the pelvic inlet
Explanation:The fetal head is engaged when the head of the foetus or the presenting part enters the pelvic inlet or pelvic brim. It usually occurs at 38 weeks of gestation.
The Spalding sign refers to the overlapping of the fetal skull bones caused by collapse of the fetal brain. It appears usually a week or more after fetal death in utero.
In brow presentation the scalp is deflexed as the foetus is looking upward. Normally the head is inflexed such that the chin is touching the chest. -
This question is part of the following fields:
- Anatomy
-
-
Question 13
Correct
-
You are asked to speak to a 27 year old patient who is pregnant for the first time. She is concerned as her friend recently gave birth and the baby was found to have profound hearing loss. Her friend was told this was due to an infection whilst she was pregnant. What is the most common infective cause of congenital hearing loss?
Your Answer: Cytomegalovirus
Explanation:CMV is the most common congenital infection causing sensorineural deafness.
10-15% of infected infants will be symptomatic at birth. A further 10-15% who are asymptomatic at birth will develop symptoms later in life. Transmission can also be via breastmilk and the incubation period for CMV is 3-12 weeks. Diagnosis of fetal CMV infection is via amniocentesis however this should not be performed for at least 6 weeks after maternal infection and not until the 21st week of gestation -
This question is part of the following fields:
- Microbiology
-
-
Question 14
Correct
-
Regarding ectopic pregnancy, where is the most common site of implantation?
Your Answer: Ampullary tubal
Explanation:Ectopic pregnancies can quickly become a gynaecological emergency if left untreated. The majority of ectopic pregnancies (95-97%) are tubal occurring in the fallopian tube as opposed to the abdomen, ovary or cervix. In tubal ectopics, the most common site of occurrence is in the ampulla (70%), followed by the isthmus, fimbria, and the cornua.
-
This question is part of the following fields:
- Epidemiology
-
-
Question 15
Incorrect
-
You're delivering contraception counselling to a young couple. They chose the 'rhythm approach' after hearing about several methods (calendar calculation). Menstrual periods last between 26 and 29 days for the woman. Which of the following abstinence durations is the most appropriate?
Your Answer: From day 12 to day 17
Correct Answer: From day 6 to day 17
Explanation:Luteal phase is always fixed to 14 days. In this patient, ovulation will occur between days 12-15. Sexual encounter must be ceased until 24-36 hours before day 15 (day 17). The start date of abstinence, calculated by decreasing 6 days (life span of the sperm) from the earliest possible day of ovulation (12-6=6). Hence from day 6-17, sexual encounter must be avoided.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 16
Incorrect
-
Question 17
Correct
-
Looking at the picture below what is the diagnosis?
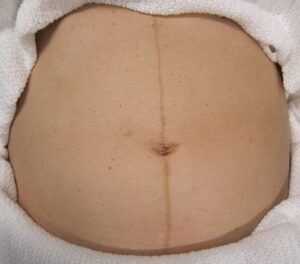
Your Answer: Linea Nigra
Explanation:This is Linea Nigra. It occurs in 3/4 of pregnancies and is due to increased melanocyte-stimulating hormone production by the placenta. This also causes melasma and darkening of the nipples.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 18
Correct
-
Question 19
Correct
-
Which of the following drugs is associated with reduced milk production whilst breastfeeding?
Your Answer: Cabergoline
Explanation:Domperidone and metoclopramide are D2 dopamine receptor antagonists. They are primarily used to promote gastric motility. They are also known as galactagogues and they promote the production of milk. Cabergoline and bromocriptine are prolactin inhibitors and they reduce milk production.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 20
Correct
-
Regarding CTG (cardiotocography) analysis what is the normal range for variability?
Your Answer: 5-25 bpm
Explanation:Fetal hypoxia may cause absent, increased or decreased variability. Other causes of decreased variability include: normal fetal sleep-wake pattern, prematurity and following maternal administration of certain drugs including opioids.
Variability Range:
Normal – 5 bpm – 25bpm
Increased – >25 bpm
Decreased – <5 bpm
Absent – <2 bpm -
This question is part of the following fields:
- Data Interpretation
-
-
Question 21
Incorrect
-
A 40 year old women has a transvaginal ultrasound reported as showing a 6cm x 5cm cystic mass of the right ovary with multiple septa noted and varying degrees of echogenicity within locules. What is the likely diagnosis?
Your Answer: Endometrioma
Correct Answer: Mucinous cystadenoma
Explanation:The characteristics of the mucinous cystic adenoma of the ovaries is the presence of a large tumour which is multicystic and the penetration of the peritoneum into the cavities forming septas. The serous tumours can only be differentiated on the bases of the contents.
-
This question is part of the following fields:
- Data Interpretation
-
-
Question 22
Incorrect
-
In normal pregnancy, levels of all of the following hormones increases, EXCEPT:
Your Answer: Oestradiol
Correct Answer: Parathyroid hormone (PTH) in the 2nd & 3rd trimesters
Explanation:In order to maintain fetal bone growth, the maternal compartment undergoes adjustments that provide a net transfer of sufficient calcium to the foetus. Maternal compartment changes that permit calcium accumulation include increases in maternal dietary intake, increases in maternal 1, 25-dihydroxyvitamin D3 levels, and increases in parathyroid hormone (PTH) levels. The levels of total calcium and phosphorus decline in maternal serum, but ionized calcium levels remain unchanged. During pregnancy, the placenta forms a calcium pump in which a gradient of calcium and phosphorus is established which favours the foetus. Thus, circulating fetal calcium and phosphorus levels increase steadily throughout gestation. Furthermore, fetal levels of total and ionized calcium, as well as phosphorus, exceed maternal levels at term. By 10-12 weeks’ gestation, the fetal parathyroid glands secrete PTH. Fetal plasma levels of PTH are low during gestation, but increase after delivery.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 23
Incorrect
-
Regarding lymph drainage of the fallopian tubes where does the majority of lymph drain to?
Your Answer: Internal iliac nodes
Correct Answer: Para-aortic nodes
Explanation:Lymphatic vessels from the ovaries, joined by vessels from the uterine tubes and most from the fundus of the uterus, follow the ovarian veins as they ascend to the right and left lumbar (caval/aortic) lymph nodes.
-
This question is part of the following fields:
- Anatomy
-
-
Question 24
Incorrect
-
What are the branches of the pudendal nerves in females?
Your Answer: Perineal, superior rectal and posterior nerve of clitoris
Correct Answer: Perineal, inferior rectal and dorsal nerve of clitoris
Explanation:The pudendal nerve provides sensory and motor innervation to regions of the anus, the perineum, the labia and the clitoris in women. The nerve is formed from the ventral rami of the S2-S4 sacral spinal nerves. The nerve is paired, each innervating the left and the right side of the body. The nerve gives the following branches in females: the inferior anal nerve, the perineal nerve and the dorsal nerve of the clitoris.
-
This question is part of the following fields:
- Anatomy
-
-
Question 25
Correct
-
A 32 year old woman who is 14 weeks pregnant presents to the clinic with yellow, frothy vaginal discharge and vaginal soreness. Trichomoniasis is confirmed after microscopy on a wet smear. Which of the following is the most appropriate treatment?
Your Answer: Metronidazole 400mg TDS 7 days
Explanation:Trichomoniasis is considered a sexually transmitted infection found both in men and women caused by the flagellate protozoan Trichomonas vaginalis. The organism is mainly found in the vagina and the urethra. Though many infected women can be asymptomatic, they can also present with yellow frothy vaginal discharge, itching and vaginitis, dysuria or an offensive odour.
For the diagnosis of t. vaginalis in women, a swab is taken from the posterior fornix during speculum examination and the flagellates are detected under light-field microscopy.
The recommended treatment for t. vaginalis during pregnancy and breastfeeding is 400-500mg of metronidazole twice daily for 5 -7 days. High dose metronidazole as a 2g single dose tablet is not advised during pregnancy. All sexual partners should also be treated, and screening for other STIs should be carried out.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 26
Incorrect
-
A 35-year-old African female presents with a history of heavy menstrual bleeding and dysmenorrhoea for 4 months. Which of the following could be the most likely cause for this presentation?
Your Answer: Endometriosis
Correct Answer: Fibroid
Explanation:History of heavy menstrual bleeding and amenorrhoea favour the diagnosis of a fibroid uterus. All the given responses are causes for subfertility. Ectopic pregnancy presents with abdominal pain has an acute presentation. Endometriosis and adenomyosis usually don’t present with amenorrhoea or heavy bleeding respectively. PID presents with chronic pelvic pain and is not related to menstruation.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 27
Correct
-
Spinnbarkheit is a term which means:
Your Answer: Threading of the cervical mucous
Explanation:Spinnability (or Spinnbarkeit), which measures the capacity of fluids to be drawn into threads, represents an indirect measurement of the adhesive and elastic properties of mucus.
-
This question is part of the following fields:
- Physiology
-
-
Question 28
Correct
-
Engagement of the foetus can be defined as:
Your Answer: When the greatest biparietal diameter of the fetal head passes the pelvic inlet
Explanation:Engagement means when the fetal head enters the pelvic brim/inlet and it usually takes place 2 weeks before the estimated delivery date i.e. at 38 weeks of pregnancy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 29
Correct
-
Which of the following Oestrogens (Oestrogens) becomes the predominant circulating oestrogen during pregnancy?
Your Answer: Estriol
Explanation:The 3 main oestrogens are Estrone (E1) Oestradiol (E2) and Estriol (E3). Oestradiol is the predominant oestrogen during female reproductive years except during the early follicular phase when Estrone predominates. During pregnancy Estriol levels rise significantly and this becomes the dominant oestrogen during pregnancy. Ethinylestradiol and Mestranol are oestrogen found in COCP’s
-
This question is part of the following fields:
- Endocrinology
-
-
Question 30
Correct
-
A 20-year-old nulligravid woman comes to the office for a routine checkup, as she is concerned about having gained 4.5 kg over the last year. She believes that the gain is related to her oral contraceptive pills. Patient takes low-dose ethinyl estradiol orethindrone daily.Prior to starting the pills, she had regular but heavy periods lasting for 4-5 days. Patient used to miss her school every month, on the first day of her period, due to severe cramping. Her pain symptoms resolved 3 months after starting the pills and she takes no other medications. Patient's coitarche was at the age of 18 and she has had 2 partners since then.Patient and her current partner use condoms inconsistently. On examination her vital signs are normal, with a BMI of 27 kg/m2 and physical examination is unremarkable. Among the following which is the most appropriate advice for this patient?
Your Answer: Reassure that the weight gain is not related to combined OCPs
Explanation:Breakthrough bleeding, breast tenderness, nausea, bloating, amenorrhea, hypertension, venous thromboembolic disease, increased risk of cervical cancer with decreased risk of ovarian & endometrial cancer, liver disorders like hepatic adenoma and increase in triglycerides due to estrogen component are the common side effects & risks of using combination oral contraceptives.
Patient in the given case mentioned symptoms of primary dysmenorrhea, which is recurrent lower abdominal pain associated with menstruation. Combination estrogen-progestin oral contraceptive pills (OCPs) are considered as the first-line treatment for dysmenorrhea in sexually active patients as OCPs help to reduce pain by thinning the endometrial lining, reducing prostaglandin release and by decreasing uterine contractions.
Nausea, bloating and breast tenderness, are considered as the early side effects of OCPs and will usually improve with continued use. The most common side effect is breakthrough bleeding which is usually associated with lower estrogen doses and other adverse effects caused by the pills include hypertension, increased risk of cervical cancer and venous thromboembolism. Although common perception considers weight gain as a side effect, several studies have shown that no significant weight gain is associated with OCPs, particularly with low-dose formulations. Considering this, the patient should be reassured that her weight gain is not associated with regular use of OCPs.In patients who are not sexually active, nonsteroidal anti-inflammatory drugs are considered as the first-line treatment for primary dysmenorrhea. As stopping contraception will increase this Patient’s risk of unintended pregnancy this is not advisable to her.
Switching the patient to a copper intrauterine device (IUD) will decrease systemic side effects, but as its inflammatory reaction in the uterus may increase pain symptoms, copper IUD is not recommended for patients with dysmenorrhea.
As Medroxyprogesterone will increase body fat and decrease lean muscle mass resulting in weight gain is not a good option for this patient. Also medroxyprogesterone due to its risk of significant loss of bone mineral density, is not recommended for adolescents or young women. So it can be used in this age group only if other options are unacceptable.
Presence of estrogen component is the main reason behind the side effects of combination OCPs. Progesterone-only pills have relatively fewer side effects but as they do not inhibit ovulation, they are less effective for treating dysmenorrhea and for contraception.
Combination oral contraceptive pills are the first-line therapy for primary dysmenorrhea in sexually active patients. Its side effects include breakthrough bleeding, hypertension, and increased risk of venous thromboembolism. Researches proves that weight gain is usually not an adverse effect of OCPs.
-
This question is part of the following fields:
- Obstetrics
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)