-
Question 1
Incorrect
-
A 42-year-old teacher from Manchester presents to her GP with a 3 month history of nonspecific upper right quadrant pain and nausea. The pain is constant, not radiating, and not affected by food. She denies any changes in bowel habits, weight loss, or fever. She drinks approximately 8 units of alcohol per week, is a non-smoker, and has no significant medical history. The GP orders blood tests and a liver ultrasound, with the following results:
Full blood count, electrolytes, liver function tests, and clotting profile are all within normal limits.
HBs antigen is negative.
Anti-HBs is positive.
Anti-HBc is negative.
IgM anti-HBc is negative.
Ultrasound reveals a single 11cm x 8 cm hyperechoic lesion in the right lobe of the liver, without other abnormalities detected and no biliary tree abnormalities noted.
What is the most likely cause of this patient's symptoms?Your Answer: Hepatocellular carcinoma
Correct Answer: Hepatic haemangioma
Explanation:Haemangiomas are benign liver growths that are usually small and do not increase in size over time. However, larger growths can cause symptoms by pressing on nearby structures, such as the stomach or biliary tree. Symptoms may include early satiety, nausea, obstructive jaundice, and right upper quadrant pain. Hepatic haemangiomas are more common than hepatocellular carcinomas in Western populations without risk factors. The presence of anti-HBs indicates previous hepatitis immunisation or immunity, which is likely for a UK phlebotomist. Symptoms of biliary colic and peptic ulcer disease typically vary with food intake, and ultrasound can detect biliary pathology such as gallbladder thickening or the presence of stones.
Benign liver lesions are non-cancerous growths that can occur in the liver. One of the most common types of benign liver tumors is a haemangioma, which is a reddish-purple hypervascular lesion that is typically separated from normal liver tissue by a ring of fibrous tissue. Liver cell adenomas are another type of benign liver lesion that are usually solitary and can be linked to the use of oral contraceptive pills. Mesenchymal hamartomas are congenital and benign, and usually present in infants. Liver abscesses can also occur, and are often caused by biliary sepsis or infections in structures drained by the portal venous system. Amoebic abscesses are a type of liver abscess that are caused by amoebiasis, and are typically seen in the right lobe of the liver. Hydatid cysts are another type of benign liver lesion that are caused by Echinococcus infection, and can grow up to 20 cm in size. Polycystic liver disease is a condition that is usually associated with polycystic kidney disease, and can cause symptoms as a result of capsular stretch. Cystadenomas are rare benign liver lesions that have malignant potential and are usually solitary multiloculated lesions. Surgical resection is often indicated for the treatment of these lesions.
-
This question is part of the following fields:
- Surgery
-
-
Question 2
Correct
-
Which one of the following scenarios is the most common presentation of testicular cancer?
Your Answer: Painless testicular lump in a 27-year-old man
Explanation:Understanding Testicular Cancer
Testicular cancer is a type of cancer that commonly affects men between the ages of 20 and 30. Germ-cell tumors are the most common type of testicular cancer, accounting for around 95% of cases. These tumors can be divided into seminomas and non-seminomas, which include embryonal, yolk sac, teratoma, and choriocarcinoma. Other types of testicular cancer include Leydig cell tumors and sarcomas. Risk factors for testicular cancer include infertility, cryptorchidism, family history, Klinefelter’s syndrome, and mumps orchitis.
The most common symptom of testicular cancer is a painless lump, although some men may experience pain. Other symptoms may include hydrocele and gynaecomastia, which occurs due to an increased oestrogen:androgen ratio. Tumor markers such as hCG, AFP, and beta-hCG may be elevated in germ cell tumors. Ultrasound is the first-line diagnostic tool for testicular cancer.
Treatment for testicular cancer depends on the type and stage of the tumor. Orchidectomy, chemotherapy, and radiotherapy may be used. Prognosis for testicular cancer is generally excellent, with a 5-year survival rate of around 95% for seminomas and 85% for teratomas if caught at Stage I. It is important for men to perform regular self-examinations and seek medical attention if they notice any changes or abnormalities in their testicles.
-
This question is part of the following fields:
- Surgery
-
-
Question 3
Correct
-
A 38-year-old overweight female has just undergone an elective laparoscopic cholecystectomy for gallstone disease. On the first day after the surgery, the nurse in charge asks you to review her as she is complaining of severe pain in the right upper quadrant. Upon examination, you find that she is tachycardic but normotensive and apyrexial. The patient's right upper quadrant is tender to palpation, but there is no evidence of jaundice. Additionally, the intra-abdominal drain in-situ has a small volume of green liquid draining from it. What is the most likely postoperative complication?
Your Answer: Biliary leak
Explanation:If a patient experiences tenderness in the right upper quadrant and bilious fluid is present in the intra-abdominal drain after a cholecystectomy, it may indicate a bile leak. However, since the patient is not running a fever and has normal blood pressure, it is unlikely that they have an intra-abdominal collection or hemorrhage. Although a laparoscopic cholecystectomy can result in perforation, the patient would typically develop peritonitis rather than localized tenderness in the right upper quadrant. Lastly, an ileus would not cause pain in the right upper quadrant or the presence of bilious fluid in the drain.
Complications can occur in all types of surgery and require vigilance in their detection. Anticipating likely complications and appropriate avoidance can minimize their occurrence. Understanding the anatomy of a surgical field will allow appreciation of local and systemic complications that may occur. Physiological and biochemical derangements may also occur, and appropriate diagnostic modalities should be utilized. Safe and timely intervention is the guiding principle for managing complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 4
Incorrect
-
A 21-year-old man is assaulted outside a nightclub and struck with a baseball bat on the left side of his head. He is taken to the emergency department and placed under observation. As his Glasgow coma score (GCS) declines, he falls into a coma. What is the most probable haemodynamic parameter that he will exhibit?
Your Answer: Hypotension and bradycardia
Correct Answer: Hypertension and bradycardia
Explanation:Before coning, hypertension and bradycardia are observed. The brain regulates its own blood supply by managing the overall blood pressure.
Types of Traumatic Brain Injury
Traumatic brain injury can result in primary and secondary brain injury. Primary brain injury can be focal or diffuse. Diffuse axonal injury occurs due to mechanical shearing, which causes disruption and tearing of axons. intracranial haematomas can be extradural, subdural, or intracerebral, while contusions may occur adjacent to or contralateral to the side of impact. Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory processes are disrupted following trauma rendering the brain more susceptible to blood flow changes and hypoxia. The Cushings reflex often occurs late and is usually a pre-terminal event.
Extradural haematoma is bleeding into the space between the dura mater and the skull. It often results from acceleration-deceleration trauma or a blow to the side of the head. The majority of epidural haematomas occur in the temporal region where skull fractures cause a rupture of the middle meningeal artery. Subdural haematoma is bleeding into the outermost meningeal layer. It most commonly occurs around the frontal and parietal lobes. Risk factors include old age, alcoholism, and anticoagulation. Subarachnoid haemorrhage classically causes a sudden occipital headache. It usually occurs spontaneously in the context of a ruptured cerebral aneurysm but may be seen in association with other injuries when a patient has sustained a traumatic brain injury. Intracerebral haematoma is a collection of blood within the substance of the brain. Causes/risk factors include hypertension, vascular lesion, cerebral amyloid angiopathy, trauma, brain tumour, or infarct. Patients will present similarly to an ischaemic stroke or with a decrease in consciousness. CT imaging will show a hyperdensity within the substance of the brain. Treatment is often conservative under the care of stroke physicians, but large clots in patients with impaired consciousness may warrant surgical evacuation.
-
This question is part of the following fields:
- Surgery
-
-
Question 5
Incorrect
-
A hospital trust is comparing the incidence of deep vein thrombosis (DVT) in patients admitted to various departments in the hospital over the past five years.
In which one of the following age groups is the risk of developing a DVT at its highest?Your Answer: Patients admitted with severe pneumonia on a general medical ward
Correct Answer: Patients undergoing total hip replacements on orthopaedic wards
Explanation:Reducing the Risk of Deep Vein Thrombosis in Hospitalized Patients
Hospitalized patients, particularly those undergoing major orthopaedic and lower limb surgery, are at a high risk of developing deep vein thrombosis (DVT). Patients with additional risk factors such as cancer and immobility are also at an increased risk. To prevent DVT, all admitted patients should undergo a risk assessment and receive necessary prophylaxis such as thromboembolic deterrent stockings (TEDS) and/or prophylactic low-molecular-weight heparin. While patients undergoing gynaecological surgery are at risk of DVT, they are not the highest risk category. Patients who have suffered from an acute stroke are also at risk, albeit less so than those undergoing major surgery. Strategies to reduce the risk of DVT should be employed for all hospitalized patients.
-
This question is part of the following fields:
- Surgery
-
-
Question 6
Incorrect
-
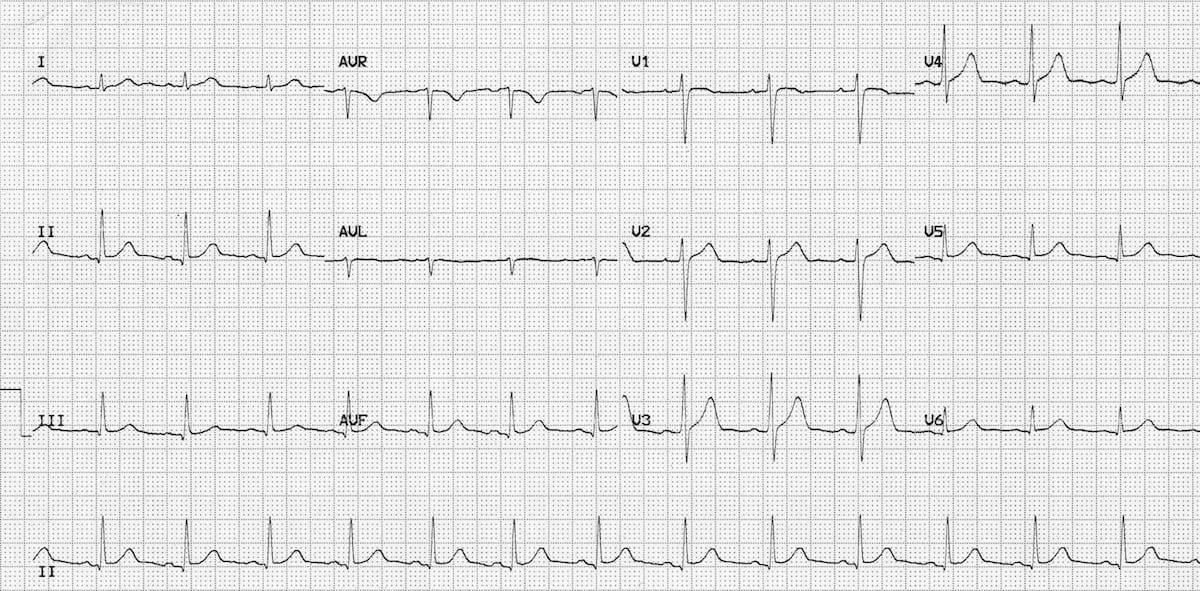
A 67-year-old man undergoes a subtotal colectomy and suffers iatrogenic injury to both ureters. He experiences renal failure and his serum potassium level is elevated at 6.9 mmol/L. An ECG is conducted, what is the probable result?
Your Answer: Increased PR interval
Correct Answer: Peaked T waves
Explanation:The initial and prevalent indication of hyperkalaemia is the presence of elevated T waves.
Hyperkalaemia is a condition that can be detected through an electrocardiogram (ECG). The ECG findings associated with hyperkalaemia include tall and pointed T waves, which are the first signs of the condition. Additionally, there may be a loss of P waves, broad QRS complexes, and a sinusoidal wave pattern. In severe cases, ventricular fibrillation may also occur. These ECG findings can help diagnose hyperkalaemia and guide appropriate treatment.
-
This question is part of the following fields:
- Surgery
-
-
Question 7
Correct
-
A 50-year-old woman presents to the surgical assessment unit with worsening upper right abdominal pain after dining out with friends. She reports experiencing this pain for the past few months, but it has never been this severe. The pain tends to worsen after dinner, especially with fast food, and occasionally radiates to her right shoulder. Upon examination, you note an increase in body weight. Her abdomen is soft and non-tender, and bowel sounds are present. She is currently not running a fever. What is the definitive treatment for this condition?
Your Answer: Elective laparoscopic cholecystectomy
Explanation:Elective laparoscopic cholecystectomy is the preferred treatment for biliary colic.
Biliary colic is typically characterized by worsening pain after eating, but the patient is generally in good health, has no fever, and has a soft abdomen. In contrast, cholecystitis is associated with signs of infection, such as fever and tachycardia, and may involve palpable gallbladder and positive Murphy’s sign. If the patient is clinically stable and a good candidate for surgery, elective cholecystectomy is the appropriate management option. Cholecystostomy is reserved for cases of acute cholecystitis with pus accumulation, while ERCP is used to remove obstructing gallstones in patients with jaundice or risk of ascending cholangitis. MRCP is a diagnostic tool and not a treatment option.
Biliary colic is a condition that occurs when gallstones pass through the biliary tree. The risk factors for this condition are commonly referred to as the ‘4 F’s’, which include being overweight, female, fertile, and over the age of forty. Other risk factors include diabetes, Crohn’s disease, rapid weight loss, and certain medications. Biliary colic occurs due to an increase in cholesterol, a decrease in bile salts, and biliary stasis. The pain associated with this condition is caused by the gallbladder contracting against a stone lodged in the cystic duct. Symptoms include right upper quadrant abdominal pain, nausea, and vomiting. Diagnosis is typically made through ultrasound. Elective laparoscopic cholecystectomy is the recommended treatment for biliary colic. However, around 15% of patients may have gallstones in the common bile duct at the time of surgery, which can result in obstructive jaundice. Other possible complications of gallstone-related disease include acute cholecystitis, ascending cholangitis, acute pancreatitis, gallstone ileus, and gallbladder cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 8
Incorrect
-
A 25-year-old woman presents to her GP with a lump on her left breast. She has no family history of breast cancer. Upon examination, a smooth, rubbery, mobile mass measuring 4 cm in diameter with clearly defined edges is found. An ultrasound of her breasts reveals a single round solid mass of 4 cm diameter, which is well circumscribed and lobulated. Core biopsy confirms the presence of epithelial and stromal elements consistent with a fibroadenoma. The lump is causing her moderate discomfort and she expresses a desire to have it removed. What is the most appropriate advice to give this patient?
A) The lump will regress by itself so no need to remove.
B) The lump is non-cancerous and hence cannot be removed, but she should return if it changes or grows.
C) Refer her for excision biopsy to remove the mass.
D) Prescribe her ibuprofen for the pain, and advise her that she does not require removal of the lump.
E) Refer her for a breast mammogram to assess the lump.
Explanation:
As the lump has examination, ultrasound, and histological findings consistent with a fibroadenoma and is causing moderate discomfort, surgical excision should be recommended. It is important to obtain histological evidence to confirm the diagnosis of fibroadenoma if excision is required. Observation and simple advice would be sufficient if the fibroadenoma were less than 3 cm, but the size and discomfort of this lump make that option incorrect. A breast mammogram is usually ineffective for a younger woman due to dense breasts. Prescribing ibuprofen is generally the treatment for fibroadenosis, which is a different condition where women experience painful breasts generally around their periods. It would not be a solution for the discomfort caused by the mass effect of the fibroadenoma.Your Answer: Prescribe her ibuprofen for the pain, and advise her that she does not require removal of the lump
Correct Answer: Refer her for excision biopsy to remove the mass
Explanation:Surgical excision is the recommended course of action for a breast fibroadenoma that is over 3 cm in size and causing moderate discomfort, based on examination, ultrasound, and histological findings. It is important to confirm the diagnosis of fibroadenoma through histological evidence before proceeding with excision. While some fibroadenomas may disappear without treatment, this is not the case for larger ones causing discomfort. Observation and simple advice are only appropriate for fibroadenomas that are less than 3 cm in size. A breast mammogram is generally not effective for younger women with dense breasts. Prescribing ibuprofen is not a solution for the discomfort caused by the fibroadenoma, as this is a different condition from fibroadenosis, which causes painful breasts around the time of menstruation.
Understanding Breast Fibroadenoma
Breast fibroadenoma is a type of breast mass that develops from a whole lobule. It is characterized by a mobile, firm, and smooth lump in the breast, which is often referred to as a breast mouse. Fibroadenoma accounts for about 12% of all breast masses and is more common in women under the age of 30.
Fortunately, fibroadenomas are usually benign and do not increase the risk of developing breast cancer. In fact, over a two-year period, up to 30% of fibroadenomas may even get smaller on their own. However, if the lump is larger than 3 cm, surgical excision is typically recommended.
In summary, breast fibroadenoma is a common type of breast mass that is usually benign and does not increase the risk of breast cancer. While it may cause concern for some women, it is important to remember that most fibroadenomas do not require treatment and may even resolve on their own.
-
This question is part of the following fields:
- Surgery
-
-
Question 9
Correct
-
Which one of the following statements regarding lidocaine is accurate?
Your Answer: Preparations mixed with adrenaline should not be used for minor surgery involving the finger
Explanation:Minor Surgery: Local Anaesthetic and Suture Material
Minor surgery often requires the use of local anaesthetic (LA) to numb the area being operated on. Lidocaine is the most commonly used LA due to its fast-acting properties and short duration of anaesthesia. The maximum safe dose of lidocaine is 3 mg/kg, with the recommended dose being 200mg (or 500 mg if mixed with adrenaline) for a 66 kg patient. This equates to 20 ml of 1% solution or 10 ml of 2% solution. Lidocaine mixed with adrenaline can also help reduce blood loss by constricting blood vessels, but should not be used near extremities to avoid the risk of ischaemia.
Suture material is also an important consideration in minor surgery. Non-absorbable sutures, such as silk, Prolene, and Ethilon, need to be removed after 7-14 days depending on the location of the wound. Absorbable sutures, such as Vicryl, Dexon, and PDS, dissolve on their own after 7-10 days. The removal times for non-absorbable sutures vary depending on the area of the body, with the face requiring removal after 3-5 days, the scalp, limbs, and chest after 7-10 days, and the hand, foot, and back after 10-14 days. Proper use of LA and suture material can help ensure a successful and safe minor surgery procedure.
-
This question is part of the following fields:
- Surgery
-
-
Question 10
Correct
-
A 56-year-old man comes to your GP office and expresses his anxiety about developing an abdominal aortic aneurysm (AAA) after his friend, who seemed healthy, passed away due to a ruptured AAA. During the physical examination, the patient's vital signs are all normal, and his body mass index is 24 kg/m². Although you can feel his abdominal pulse, it is not expansile. As a result, you decide to educate the patient about the abdominal aortic aneurysm screening program.
What information would you provide to the patient during this discussion?Your Answer: A single abdominal ultrasound for those aged 65-years-old
Explanation:A single abdominal ultrasound is offered to all males aged 65 in England for screening of an abdominal aortic aneurysm (AAA). This is because the risk of getting an AAA is much smaller in women, men under 65, and those who have already been treated for an AAA. The screening is performed as an individual scan initially, and subsequent scans may be required depending on the size of the AAA. Therefore, options such as abdominal ultrasound every 3 or 5 years between 60 and 75-years-old are incorrect. Similarly, a single abdominal ultrasound for those aged 55 or 60-years-old is also incorrect as the screening is specifically for those aged 65.
Abdominal aortic aneurysm (AAA) is a condition that often develops without any symptoms. However, a ruptured AAA can be fatal, which is why it is important to screen patients for this condition. Screening involves a single abdominal ultrasound for males aged 65. The results of the screening are interpreted based on the width of the aorta. If the width is less than 3 cm, no further action is needed. If it is between 3-4.4 cm, the patient should be rescanned every 12 months. For a width of 4.5-5.4 cm, the patient should be rescanned every 3 months. If the width is 5.5 cm or more, the patient should be referred to vascular surgery within 2 weeks for probable intervention.
For patients with a low risk of rupture, which includes those with a small or medium aneurysm (i.e. aortic diameter less than 5.5 cm) and no symptoms, abdominal US surveillance should be conducted on the time-scales outlined above. Additionally, cardiovascular risk factors should be optimized, such as quitting smoking. For patients with a high risk of rupture, which includes those with a large aneurysm (i.e. aortic diameter of 5.5 cm or more) or rapidly enlarging aneurysm (more than 1 cm/year) or those with symptoms, they should be referred to vascular surgery within 2 weeks for probable intervention. Treatment for these patients may involve elective endovascular repair (EVAR) or open repair if EVAR is not suitable. EVAR involves placing a stent into the abdominal aorta via the femoral artery to prevent blood from collecting in the aneurysm. However, a complication of EVAR is an endo-leak, which occurs when the stent fails to exclude blood from the aneurysm and usually presents without symptoms on routine follow-up.
-
This question is part of the following fields:
- Surgery
-
-
Question 11
Correct
-
A 55-year-old woman presents to the clinic with a 9-month history of rectal bleeding and pain. Her physician decides to perform a proctoscopy. The results show an erythematous ulcerated plaque near the pectinate line, and biopsy results suggest squamous cell carcinoma. What is the most significant risk factor for this diagnosis?
Your Answer: HPV infection
Explanation:The strongest risk factor for anal cancer is HPV infection, specifically the HPV16 or HPV18 subtypes that cause SCCs of the anus. While HIV infection, immunosuppressant drugs, and a past medical history of cervical cancer are also risk factors, HPV infection is the most significant.
Understanding Anal Cancer: Definition, Epidemiology, and Risk Factors
Anal cancer is a type of malignancy that occurs exclusively in the anal canal, which is bordered by the anorectal junction and the anal margin. The majority of anal cancers are squamous cell carcinomas, but other types include melanomas, lymphomas, and adenocarcinomas. The incidence of anal cancer is relatively rare, with an annual rate of about 1.5 in 100,000 in the UK. However, the incidence is increasing, particularly among men who have sex with men, due to widespread infection by human papillomavirus (HPV).
There are several risk factors associated with anal cancer, including HPV infection, anal intercourse, a high lifetime number of sexual partners, HIV infection, immunosuppressive medication, a history of cervical cancer or cervical intraepithelial neoplasia, and smoking. Patients typically present with symptoms such as perianal pain, perianal bleeding, a palpable lesion, and faecal incontinence.
To diagnose anal cancer, T stage assessment is conducted, which includes a digital rectal examination, anoscopic examination with biopsy, and palpation of the inguinal nodes. Imaging modalities such as CT, MRI, endo-anal ultrasound, and PET are also used. The T stage system for anal cancer is described by the American Joint Committee on Cancer and the International Union Against Cancer. It includes TX primary tumour cannot be assessed, T0 no evidence of primary tumour, Tis carcinoma in situ, T1 tumour 2 cm or less in greatest dimension, T2 tumour more than 2 cm but not more than 5 cm in greatest dimension, T3 tumour more than 5 cm in greatest dimension, and T4 tumour of any size that invades adjacent organ(s).
In conclusion, understanding anal cancer is crucial in identifying the risk factors and symptoms associated with this type of malignancy. Early diagnosis and treatment can significantly improve the prognosis and quality of life for patients.
-
This question is part of the following fields:
- Surgery
-
-
Question 12
Incorrect
-
A 35-year-old woman in her second pregnancy has given birth to a live male baby. She has no significant medical history. Suddenly, ten minutes after delivery, she experiences a severe headache at the back of her head, accompanied by vomiting. Photophobia is evident upon examination. She loses consciousness shortly after and has a Glasgow coma score of 8. A CT scan reveals blood in the basal cisterns, sulci, and fissures. What is the probable diagnosis?
Your Answer: Sheehan's syndrome
Correct Answer: Subarachnoid haemorrhage
Explanation:A thunderclap headache and meningitis symptoms are key clinical features of a subarachnoid haemorrhage (SAH), which is a type of stroke caused by bleeding from a berry aneurysm in the Circle of Willis. The headache typically reaches maximum severity within seconds to minutes.
A subarachnoid haemorrhage (SAH) is a type of bleeding that occurs within the subarachnoid space of the meninges in the brain. It can be caused by head injury or occur spontaneously. Spontaneous SAH is often caused by an intracranial aneurysm, which accounts for around 85% of cases. Other causes include arteriovenous malformation, pituitary apoplexy, and mycotic aneurysms. The classic symptoms of SAH include a sudden and severe headache, nausea and vomiting, meningism, coma, seizures, and ECG changes.
The first-line investigation for SAH is a non-contrast CT head, which can detect acute blood in the basal cisterns, sulci, and ventricular system. If the CT is normal within 6 hours of symptom onset, a lumbar puncture is not recommended. However, if the CT is normal after 6 hours, a lumbar puncture should be performed at least 12 hours after symptom onset to check for xanthochromia and other CSF findings consistent with SAH. If SAH is confirmed, referral to neurosurgery is necessary to identify the underlying cause and provide urgent treatment.
Management of aneurysmal SAH involves supportive care, such as bed rest, analgesia, and venous thromboembolism prophylaxis. Vasospasm is prevented with oral nimodipine, and intracranial aneurysms require prompt intervention to prevent rebleeding. Most aneurysms are treated with a coil by interventional neuroradiologists, but some require a craniotomy and clipping by a neurosurgeon. Complications of aneurysmal SAH include re-bleeding, hydrocephalus, vasospasm, and hyponatraemia. Predictive factors for SAH include conscious level on admission, age, and amount of blood visible on CT head.
-
This question is part of the following fields:
- Surgery
-
-
Question 13
Incorrect
-
A 62-year-old man presents to the pre-admission clinic for assessment prior to an elective prostatectomy. You find no adverse past medical history and examination is unremarkable. An electrocardiogram (ECG) is indicated in all pre-operative patients undergoing major surgery who are over the age of 60. The ECG is shown below.
 After having reviewed the ECG, what is the next best step to take with this patient?
After having reviewed the ECG, what is the next best step to take with this patient? Your Answer: Discuss the patient with the list anaesthetist
Correct Answer: No further assessment is required
Explanation:Assessing Cardiac Risk in Preoperative Patients: Common Misconceptions
There are several misconceptions when it comes to assessing cardiac risk in preoperative patients. One common mistake is assuming that all patients require extensive cardiac testing, even when there are no significant risk factors or symptoms present. For example, if a patient has no significant past medical history and their examination is unremarkable, an echocardiogram is not necessary.
On the other hand, some clinicians may be too cautious and cancel a patient’s procedure based on a perceived cardiac risk that is not supported by evidence. If the patient’s ECG is normal and there are no cardiac risk factors, cancelling the procedure would be unreasonable.
It is important to recognise that not all preoperative patients require extensive cardiac testing. Instead, clinicians should focus on identifying patients with specific cardiac conditions that require closer monitoring and management. By avoiding unnecessary testing and interventions, clinicians can improve patient outcomes and reduce healthcare costs.
-
This question is part of the following fields:
- Surgery
-
-
Question 14
Incorrect
-
A 35-year-old female presents to the emergency department with persistent right upper quadrant pain and jaundiced sclera, three weeks after undergoing laparoscopic cholecystectomy. She is anxious about the possibility of a surgical complication requiring revision surgery.
What is the probable cause of her symptoms?Your Answer: Failure of surgical anastomosis
Correct Answer: Gallstones present in the common bile duct causing symptoms
Explanation:The correct answer to the multiple-choice question is CBD gallstones. While gallbladder stump gallstones can occur after laparoscopic cholecystectomies, they are less common than CBD gallstones. Additionally, it is important to note that the patient in the vignette is presenting 3 weeks after the operation, whereas gallbladder stump gallstones typically present over 9 months following incomplete gallbladder removal (although in rare cases, it can take up to 25 years postoperatively).
Biliary colic is a condition that occurs when gallstones pass through the biliary tree. The risk factors for this condition are commonly referred to as the ‘4 F’s’, which include being overweight, female, fertile, and over the age of forty. Other risk factors include diabetes, Crohn’s disease, rapid weight loss, and certain medications. Biliary colic occurs due to an increase in cholesterol, a decrease in bile salts, and biliary stasis. The pain associated with this condition is caused by the gallbladder contracting against a stone lodged in the cystic duct. Symptoms include right upper quadrant abdominal pain, nausea, and vomiting. Diagnosis is typically made through ultrasound. Elective laparoscopic cholecystectomy is the recommended treatment for biliary colic. However, around 15% of patients may have gallstones in the common bile duct at the time of surgery, which can result in obstructive jaundice. Other possible complications of gallstone-related disease include acute cholecystitis, ascending cholangitis, acute pancreatitis, gallstone ileus, and gallbladder cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 15
Correct
-
A 5-week-old girl is brought to the pediatrician by her father. He is worried about a 'lump' in the left side of her scrotum that has developed over the past week. The baby has been eating well, has not had any diarrhea or cold symptoms, and does not seem to be in any discomfort.
During the examination, a swelling is detected on the left side of the scrotum. It is possible to get above the swelling. The left testicle is easily palpable, but the right testicle is difficult to feel due to the swelling. On transillumination, the left hemiscrotum lights up.
What is the most appropriate course of action based on the given information?Your Answer: Reassure that it is not sinister and will likely resolve by 1 year
Explanation:This young boy is showing signs of a hydrocele, which may not have been noticed at birth. Hydroceles tend to become more visible as fluid accumulates. Aspiration is not recommended as it is invasive and unnecessary in this case. Specialist intervention is also not required unless the hydrocele persists beyond 18 months to 2 years of age. It is not expected to resolve within a week, but this is not a cause for concern. Hydroceles are typically self-resolving and do not cause any immediate complications. Therefore, the mother does not need to return unless the hydrocele persists beyond this time. Expectant management and reassurance are appropriate as hydroceles are not painful and generally do not cause complications. Ultrasound is not necessary as the diagnosis is clinical, but it may be considered if there is any doubt on history or examination, such as to rule out an inguinal hernia.
A hydrocele is a condition where fluid accumulates within the tunica vaginalis. There are two types of hydroceles: communicating and non-communicating. Communicating hydroceles occur when the processus vaginalis remains open, allowing peritoneal fluid to drain into the scrotum. This type of hydrocele is common in newborn males and usually resolves within a few months. Non-communicating hydroceles occur when there is excessive fluid production within the tunica vaginalis. Hydroceles can develop secondary to conditions such as epididymo-orchitis, testicular torsion, or testicular tumors.
The main feature of a hydrocele is a soft, non-tender swelling of the hemi-scrotum that is usually located anterior to and below the testicle. The swelling is confined to the scrotum and can be transilluminated with a pen torch. If the hydrocele is large, the testis may be difficult to palpate. Diagnosis can be made clinically, but ultrasound is necessary if there is any doubt about the diagnosis or if the underlying testis cannot be palpated.
Management of hydroceles depends on the severity of the presentation. Infantile hydroceles are generally repaired if they do not resolve spontaneously by the age of 1-2 years. In adults, a conservative approach may be taken, but further investigation, such as an ultrasound, is usually warranted to exclude any underlying cause, such as a tumor.
-
This question is part of the following fields:
- Surgery
-
-
Question 16
Correct
-
A 50-year-old woman has been referred to the Surgical Assessment Unit by her doctor after an ultrasound scan revealed biliary dilation and subsequent imaging confirmed the presence of gallstones. She woke up this morning with severe pain in the right upper quadrant, accompanied by sweating and her husband noticed her skin appeared more yellow than usual. What is the probable diagnosis?
Your Answer: Ascending cholangitis
Explanation:The presence of fever, jaundice and right upper quadrant pain in this patient indicates Charcot’s cholangitis triad, which strongly suggests the possibility of ascending cholangitis, particularly given the history of confirmed gallstones. The recommended course of action is to administer intravenous antibiotics.
Understanding Ascending Cholangitis
Ascending cholangitis is a bacterial infection that affects the biliary tree, with E. coli being the most common culprit. This condition is often associated with gallstones, which can predispose individuals to the infection. Patients with ascending cholangitis may present with Charcot’s triad, which includes fever, right upper quadrant pain, and jaundice. However, this triad is only present in 20-50% of cases. Other common symptoms include hypotension and confusion. In severe cases, Reynolds’ pentad may be observed, which includes the additional symptoms of hypotension and confusion.
To diagnose ascending cholangitis, ultrasound is typically used as a first-line investigation to look for bile duct dilation and stones. Raised inflammatory markers may also be observed. Treatment involves intravenous antibiotics and endoscopic retrograde cholangiopancreatography (ERCP) after 24-48 hours to relieve any obstruction.
Overall, ascending cholangitis is a serious condition that requires prompt diagnosis and treatment. Understanding the symptoms and risk factors associated with this condition can help individuals seek medical attention early and improve their chances of a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 17
Incorrect
-
Mrs. Johnson is a 36-year-old woman who complains of nausea, vomiting, high-pitched bowel sounds, and worsening abdominal pain. She reports a history of abdominal surgery due to a ruptured appendix a few years ago. What is the definitive diagnostic test to determine the cause of her symptoms?
Your Answer: Abdominal x-ray (AXR)
Correct Answer: Abdominal CT
Explanation:The definitive diagnostic investigation for small bowel obstruction is CT abdomen, while AXR is the first-line investigation for suspected bowel obstruction. Although AXR may provide information, it is not a definitive diagnostic tool.
Small bowel obstruction occurs when the small intestines are blocked, preventing the passage of food, fluids, and gas. The most common cause of this condition is adhesions, which can develop after previous surgeries, followed by hernias. Symptoms of small bowel obstruction include diffuse, central abdominal pain, nausea and vomiting (often bilious), constipation, and abdominal distension. Tinkling bowel sounds may also be present in early stages of obstruction. Abdominal x-ray is typically the first-line imaging for suspected small bowel obstruction, showing distended small bowel loops with fluid levels. CT is more sensitive and considered the definitive investigation, particularly in early obstruction. Management involves initial steps such as NBM, IV fluids, and nasogastric tube with free drainage. Some patients may respond to conservative management, but others may require surgery.
-
This question is part of the following fields:
- Surgery
-
-
Question 18
Correct
-
A 38-year-old construction worker complains of sudden onset groin pain on the left side that radiates from the flank. The pain is intermittent but excruciating when it occurs and is not related to movement. The patient's examination, observations, and blood tests are normal, but a urine dip reveals ++ blood. The patient reports that his job involves heavy lifting and he rarely takes breaks. What is the probable diagnosis?
Your Answer: Ureteric calculus
Explanation:The young man is experiencing pain on his right side, from his lower back to his groin, and has microscopic blood in his urine. It is suggested that he may be frequently dehydrated due to his job. Based on these symptoms, it is highly likely that he has a kidney stone on his right side, which is causing the colicky pain. Although his job involves heavy lifting, there is no indication of a visible lump during examination, making a hernia unlikely.
The management of renal stones involves initial medication and investigations, including an NSAID for analgesia and a non-contrast CT KUB for imaging. Stones less than 5mm may pass spontaneously, but more intensive treatment is needed for ureteric obstruction or renal abnormalities. Treatment options include shockwave lithotripsy, ureteroscopy, and percutaneous nephrolithotomy. Prevention strategies include high fluid intake, low animal protein and salt diet, and medication such as thiazides diuretics for hypercalciuria and allopurinol for uric acid stones.
-
This question is part of the following fields:
- Surgery
-
-
Question 19
Correct
-
A 68-year-old man presents with a three-month history of typical dyspepsia symptoms, including epigastric pain and a 2-stone weight loss. Despite treatment with a proton pump inhibitor, he has not experienced any relief. He now reports difficulty eating solids and frequent post-meal vomiting. On examination, a palpable mass is found in the epigastrium. His full blood count shows a haemoglobin level of 85 g/L (130-180). What is the probable diagnosis?
Your Answer: Carcinoma of stomach
Explanation:Alarm Symptoms of Foregut Malignancy
The presence of alarm symptoms in patients over 55 years old, such as weight loss, bleeding, dysphagia, vomiting, blood loss, and a mass, are indicative of a malignancy of the foregut. It is crucial to refer these patients for urgent endoscopy, especially if dysphagia is a new onset symptom. However, it is unfortunate that patients with alarm symptoms are often treated with PPIs instead of being referred for further evaluation. Although PPIs may provide temporary relief, they only delay the diagnosis of the underlying tumor.
The patient’s symptoms should not be ignored, and prompt referral for endoscopy is necessary to rule out malignancy. Early detection and treatment of foregut malignancy can significantly improve patient outcomes. Therefore, it is essential to recognize the alarm symptoms and refer patients for further evaluation promptly. Healthcare providers should avoid prescribing PPIs as a first-line treatment for patients with alarm symptoms and instead prioritize timely referral for endoscopy.
-
This question is part of the following fields:
- Surgery
-
-
Question 20
Correct
-
Which of the following interventions is most likely to decrease the occurrence of intra-abdominal adhesions?
Your Answer: Use of a laparoscopic approach over open surgery
Explanation:Adhesion formation can be reduced by opting for laparoscopy over traditional surgery. The use of talc-coated surgical gloves, which was a major contributor to adhesion formation, has been discontinued. The outdated Nobles plication procedure does not aid in preventing adhesion formation. While the use of an anastomotic stapling device does not directly affect adhesion development, it is important to avoid anastomotic leaks as they can lead to increased adhesion formation.
Complications can occur in all types of surgery and require vigilance in their detection. Anticipating likely complications and appropriate avoidance can minimize their occurrence. Understanding the anatomy of a surgical field will allow appreciation of local and systemic complications that may occur. Physiological and biochemical derangements may also occur, and appropriate diagnostic modalities should be utilized. Safe and timely intervention is the guiding principle for managing complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 21
Incorrect
-
A 35-year-old woman presents to the emergency department with abdominal pain and nausea. She has a medical history of gallstones and alcohol dependence. Upon examination, she has a tender right epigastrium and a temperature of 38.3ºC. Despite this, she is hemodynamically stable. Her blood results show a raised white cell count and C-reactive protein, but her liver profile and serum amylase/lipase results are normal. The sepsis protocol is initiated, and she is started on intravenous antibiotics. What is the most appropriate next step in managing this patient's likely diagnosis?
Your Answer: Open cholecystectomy once inflammation has subsided
Correct Answer: Laparoscopic cholecystectomy within 1 week of diagnosis
Explanation:The recommended treatment for acute cholecystitis is intravenous antibiotics followed by laparoscopic cholecystectomy within 1 week of diagnosis. Conservative management is not recommended as it may lead to chronic disease and recurrence of infection. Delaying treatment and opting for open cholecystectomy once inflammation has subsided is also not recommended as it has been associated with increased rates of sepsis, jaundice, and cancer. Laparoscopic cholecystectomy is preferred over open cholecystectomy as it is associated with lower postoperative morbidity, mortality, and reduced length of stay in the hospital.
Acute cholecystitis is a condition where the gallbladder becomes inflamed. This is usually caused by gallstones, which are present in 90% of cases. The remaining 10% of cases are known as acalculous cholecystitis and are typically seen in severely ill patients who are hospitalized. The pathophysiology of acute cholecystitis is multifactorial and can be caused by gallbladder stasis, hypoperfusion, and infection. In immunosuppressed patients, it may develop due to Cryptosporidium or cytomegalovirus. This condition is associated with high morbidity and mortality rates.
The main symptom of acute cholecystitis is right upper quadrant pain, which may radiate to the right shoulder. Patients may also experience fever and signs of systemic upset. Murphy’s sign, which is inspiratory arrest upon palpation of the right upper quadrant, may be present. Liver function tests are typically normal, but deranged LFTs may indicate Mirizzi syndrome, which is caused by a gallstone impacted in the distal cystic duct, causing extrinsic compression of the common bile duct.
Ultrasound is the first-line investigation for acute cholecystitis. If the diagnosis remains unclear, cholescintigraphy (HIDA scan) may be used. In this test, technetium-labelled HIDA is injected IV and taken up selectively by hepatocytes and excreted into bile. In acute cholecystitis, there is cystic duct obstruction, and the gallbladder will not be visualized.
The treatment for acute cholecystitis involves intravenous antibiotics and cholecystectomy. NICE now recommends early laparoscopic cholecystectomy, within 1 week of diagnosis. Previously, surgery was delayed for several weeks until the inflammation had subsided. Pregnant women should also proceed to early laparoscopic cholecystectomy to reduce the chances of maternal-fetal complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 22
Incorrect
-
A 45-year-old man comes to the Emergency Department complaining of severe retrosternal pain that has been ongoing for 3 hours. He reports having consumed a large amount of alcohol yesterday, resulting in significant regurgitation. On palpation of the chest wall, crepitus is detected. His ECG reveals sinus tachycardia. What test should be conducted to confirm the probable diagnosis?
Your Answer: Transoesophageal echocardiogram
Correct Answer: CT contrast swallow
Explanation:The preferred investigation for suspected Boerhaave’s syndrome is a CT contrast swallow. This syndrome is characterized by the spontaneous rupture of the oesophagus, often caused by repeated vomiting/retching, and can be fatal if not diagnosed early. A history of binge drinking is a common risk factor. The CT contrast swallow typically shows pneumomediastinum, pneumothorax, pleural effusion, and oral contrast leaking into the mediastinum, which can cause crepitus on palpation due to subcutaneous emphysema. Blood alcohol concentration testing is not necessary unless there is a suspicion of ongoing intoxication. Endoscopy carries the risk of further perforation and is not the preferred investigation for Boerhaave’s syndrome. A transoesophageal echocardiogram is used for assessing suspected aortic dissection in unstable patients or for monitoring during cardiothoracic surgery and is not relevant for Boerhaave’s syndrome.
Boerhaave’s Syndrome: A Dangerous Rupture of the Oesophagus
Boerhaave’s syndrome is a serious condition that occurs when the oesophagus ruptures due to repeated episodes of vomiting. This rupture is typically located on the left side of the oesophagus and can cause sudden and severe chest pain. Patients may also experience subcutaneous emphysema, which is the presence of air under the skin of the chest wall.
To diagnose Boerhaave’s syndrome, a CT contrast swallow is typically performed. Treatment involves thoracotomy and lavage, with primary repair being feasible if surgery is performed within 12 hours of onset. If surgery is delayed beyond 12 hours, a T tube may be inserted to create a controlled fistula between the oesophagus and skin. However, delays beyond 24 hours are associated with a very high mortality rate.
Complications of Boerhaave’s syndrome can include severe sepsis, which occurs as a result of mediastinitis.
-
This question is part of the following fields:
- Surgery
-
-
Question 23
Correct
-
A 28-year-old man suddenly developed a severe headache and was diagnosed with a condition that caused increased attenuation of certain areas in his brain. He underwent surgery and has been receiving IV fluids since admission. On the third day of his hospital stay, his routine blood tests showed hyponatremia. What is the probable cause of his low sodium levels?
Your Answer: Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
Explanation:The syndrome of inappropriate antidiuretic hormone secretion (SIADH) involves the continued secretion or action of arginine vasopressin (AVP) despite normal or increased plasma volume. The resulting impairment of water secretion and consequent water retention produces the hyponatremia. The etiology of SIADH is divided into four main clinical categories: malignancy, pulmonary, pharmacologic, and neurologic causes.
SIADH is also commonly associated with intracranial diseases, particularly traumatic brain injury, where almost all cases resolve spontaneously with recovery from brain injury. Over 50% of patients with subarachnoid hemorrhage develop hyponatremia in the first week following the bleed, and 80% of these are due to SIADH.
A subarachnoid haemorrhage (SAH) is a type of bleed that occurs within the subarachnoid space of the meninges in the brain. It can be caused by head injury or occur spontaneously. Spontaneous SAH is often caused by an intracranial aneurysm, which accounts for around 85% of cases. Other causes include arteriovenous malformation, pituitary apoplexy, and mycotic aneurysms. The classic symptoms of SAH include a sudden and severe headache, nausea and vomiting, meningism, coma, seizures, and ECG changes.
The first-line investigation for SAH is a non-contrast CT head, which can detect acute blood in the basal cisterns, sulci, and ventricular system. If the CT is normal within 6 hours of symptom onset, a lumbar puncture is not recommended. However, if the CT is normal after 6 hours, a lumbar puncture should be performed at least 12 hours after symptom onset to check for xanthochromia and other CSF findings consistent with SAH. If SAH is confirmed, referral to neurosurgery is necessary to identify the underlying cause and provide urgent treatment.
Management of aneurysmal SAH involves supportive care, such as bed rest, analgesia, and venous thromboembolism prophylaxis. Vasospasm is prevented with oral nimodipine, and intracranial aneurysms require prompt intervention to prevent rebleeding. Most aneurysms are treated with a coil by interventional neuroradiologists, but some require a craniotomy and clipping by a neurosurgeon. Complications of aneurysmal SAH include re-bleeding, hydrocephalus, vasospasm, and hyponatraemia. Hyponatremia following subarachnoid hemorrhage occurs due to the inappropriate secretion of antidiuretic hormone (SIADH). However; it is also associated with certain dehydration states.
Predictive factors for SAH include conscious level on admission, age, and amount of blood visible on CT head.
-
This question is part of the following fields:
- Surgery
-
-
Question 24
Incorrect
-
A 65-year-old man comes in for his annual check-up without new complaints or symptoms. Routine blood tests and a urine dip are performed, revealing the following results:
- Hb: 150 g/L (Male: 135-180)
- Platelets: 200 * 109/L (150-400)
- WBC: 11.8 * 109/L (4.0-11.0)
- Na+: 140 mmol/L (135-145)
- K+: 4.2 mmol/L (3.5-5.0)
- Urea: 7.2 mmol/L (2.0-7.0)
- Creatinine: 98 µmol/L (55-120)
- CRP: 3 mg/L (<5)
- Urine Appearance: Clear
- Blood: +++
- Protein: -
- Nitrites: -
- Leucocytes: +
What should be the GP's next course of action for this patient?Your Answer: Send a urine sample away for microscopy, culture and sensitivity
Correct Answer: 2-week wait referral using the suspected cancer pathway
Explanation:A patient who is 60 years or older and presents with unexplained non-visible haematuria along with either dysuria or a raised white cell count on a blood test should be referred using the suspected cancer pathway within 2 weeks to rule out bladder cancer. Therefore, the correct answer is a 2-week wait referral. Prescribing treatment for a urinary tract infection is not appropriate as the patient does not exhibit any symptoms of a UTI. Similarly, repeating U&Es in 4 weeks is not necessary as the patient’s U&Es are normal. Screening for diabetes is also not indicated as there are no symptoms suggestive of diabetes at present.
Bladder cancer is the second most common urological cancer, with males aged between 50 and 80 years being the most commonly affected. Smoking and exposure to hydrocarbons such as 2-Naphthylamine increase the risk of the disease. Chronic bladder inflammation from Schistosomiasis infection is a common cause of squamous cell carcinomas in countries where the disease is endemic. Benign tumors of the bladder, including inverted urothelial papilloma and nephrogenic adenoma, are uncommon.
Urothelial (transitional cell) carcinoma is the most common type of bladder malignancy, accounting for over 90% of cases. Squamous cell carcinoma and adenocarcinoma are less common. Urothelial carcinomas may be solitary or multifocal, with up to 70% having a papillary growth pattern. Superficial tumors have a better prognosis, while solid growths are more prone to local invasion and may be of higher grade, resulting in a worse prognosis. TNM staging is used to determine the extent of the tumor and the presence of nodal or distant metastasis.
Most patients with bladder cancer present with painless, macroscopic hematuria. Incidental microscopic hematuria may also indicate malignancy in up to 10% of females over 50 years old. Diagnosis is made through cystoscopy and biopsies or transurethral resection of bladder tumor (TURBT), with pelvic MRI and CT scanning used to determine locoregional spread and distant disease. Treatment options include TURBT, intravesical chemotherapy, radical cystectomy with ileal conduit, or radical radiotherapy, depending on the extent and grade of the tumor. Prognosis varies depending on the stage of the tumor, with T1 having a 90% survival rate and any T with N1-N2 having a 30% survival rate.
-
This question is part of the following fields:
- Surgery
-
-
Question 25
Incorrect
-
A 45-year-old patient presents to their GP with a 3-month history of worsening dyspepsia, epigastric pain, and drenching night sweats on a background of recurrent gastric ulcers. The GP urgently refers the patient for investigation. Following a gastroscopy with biopsies taken, a low grade gastric MALT lymphoma is diagnosed, and the presence of H. pylori was also noted on the biopsy report. The patient has no significant past medical history. What treatment plan is the doctor likely to recommend?
Your Answer: Partial gastrectomy
Correct Answer: Omeprazole, amoxicillin and clarithromycin
Explanation:The recommended treatment for gastric MALT lymphoma associated with H. pylori infection is a combination of omeprazole, amoxicillin, and clarithromycin. This is because the majority of cases are linked to H. pylori, as suggested by the patient’s history of gastric ulcers. Low-grade cases can be treated with H. pylori eradication alone, but high-grade or atypical cases may require chemotherapy and/or radiotherapy. The answer choice of lansoprazole, clarithromycin, and doxycycline is incorrect, as doxycycline is not used in H. pylori eradication. Active monitoring may be an option in some cases, but when a clear cause like H. pylori is identified, treatment is recommended. Partial gastrectomy is not a standard treatment for gastric MALT lymphoma.
Gastric MALT Lymphoma: A Brief Overview
Gastric MALT lymphoma is a type of lymphoma that is commonly associated with H. pylori infection, which is present in 95% of cases. The good news is that this type of lymphoma has a good prognosis, especially if it is low grade. In fact, about 80% of patients with low-grade gastric MALT lymphoma respond well to H. pylori eradication.
One potential feature of gastric MALT lymphoma is the presence of paraproteinaemia, which is an abnormal protein in the blood. However, this is not always present and may not be a reliable indicator of the disease. Overall, gastric MALT lymphoma is a treatable form of lymphoma with a high likelihood of successful treatment.
-
This question is part of the following fields:
- Surgery
-
-
Question 26
Incorrect
-
A 26-year-old male is brought to the emergency department following a car accident where he sustained injuries to his cervical spine and left tibia. Upon assessment, his airway is open, but he is experiencing difficulty breathing. However, his chest is clear upon auscultation, and he has a respiratory rate of 18 breaths/min with an oxygen saturation of 96% in air. He appears flushed and warm to the touch, with a heart rate of 60 beats/min and blood pressure of 75/45 mmHg. What is the appropriate treatment for the likely cause of his presentation?
Your Answer: Fresh frozen plasma (FFP)
Correct Answer: Vasopressors
Explanation:After trauma, a spinal cord transection can result in neurogenic shock, which is consistent with the patient’s presentation. The injury to the cervical spine puts the patient at risk of this type of shock, which is characterized by hypotension due to massive vasodilation caused by decreased sympathetic or increased parasympathetic tone. As a result, the patient cannot produce a tachycardic response to the hypotension, and vasopressors are needed to reverse the vasodilation and address the underlying cause of shock. While IV fluids may be given in the interim, they do not address the root cause of the presentation. Haemorrhagic shock is a differential diagnosis, but it is less likely given the evidence of vasodilation and lack of tachycardia. Packed red cells and FFP are not appropriate treatments in this case. IM adrenaline would be suitable for anaphylactic shock, but this is not indicated in this patient.
Understanding Shock: Aetiology and Management
Shock is a condition that occurs when there is inadequate tissue perfusion. It can be caused by various factors, including sepsis, haemorrhage, neurogenic injury, cardiogenic events, and anaphylaxis. Septic shock is a major concern, with a mortality rate of over 40% in patients with severe sepsis. Haemorrhagic shock is often seen in trauma patients, and the severity is classified based on the amount of blood loss and associated physiological changes. Neurogenic shock occurs following spinal cord injury, leading to decreased peripheral vascular resistance and cardiac output. Cardiogenic shock is commonly caused by ischaemic heart disease or direct myocardial trauma. Anaphylactic shock is a severe hypersensitivity reaction that can be life-threatening.
The management of shock depends on the underlying cause. In septic shock, prompt administration of antibiotics and haemodynamic stabilisation are crucial. In haemorrhagic shock, controlling bleeding and maintaining circulating volume are essential. In neurogenic shock, peripheral vasoconstrictors are used to restore vascular tone. In cardiogenic shock, supportive treatment and surgery may be required. In anaphylactic shock, adrenaline is the most important drug and should be given as soon as possible.
Understanding the aetiology and management of shock is crucial for healthcare professionals to provide timely and appropriate interventions to improve patient outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 27
Incorrect
-
A 45-year-old man comes to you with a chronic inguinal hernia. During the examination, you notice a small, direct inguinal hernia. He asks about the likelihood of strangulation if he chooses not to have surgery within the next year. What is the estimated risk of strangulation over the next 12 months?
Your Answer: <5%
Correct Answer:
Explanation:Indirect hernias are more likely to cause bowel obstruction, which can be life-threatening if not treated promptly. Elective repair of hernias is generally safe, but emergency repair carries a higher risk of mortality, especially in older patients.
Understanding Inguinal Hernias
Inguinal hernias are the most common type of abdominal wall hernias, with 75% of cases falling under this category. They are more prevalent in men, with a 25% lifetime risk of developing one. The main feature of an inguinal hernia is a lump in the groin area, which is located superior and medial to the pubic tubercle. This lump disappears when pressure is applied or when the patient lies down. Discomfort and aching are common symptoms, which can worsen with activity, but severe pain is rare. Strangulation, a serious complication, is uncommon.
The clinical management of inguinal hernias involves treating medically fit patients, even if they are asymptomatic. A hernia truss may be an option for patients who are not fit for surgery, but it has little role in other patients. Mesh repair is the preferred method of treatment, as it is associated with the lowest recurrence rate. Unilateral hernias are generally repaired with an open approach, while bilateral and recurrent hernias are repaired laparoscopically. Patients can return to non-manual work after 2-3 weeks following an open repair and after 1-2 weeks following laparoscopic repair, according to the Department for Work and Pensions.
Complications of inguinal hernias include early bruising and wound infection, as well as late chronic pain and recurrence. While traditional textbooks describe the anatomical differences between indirect and direct hernias, this is not relevant to clinical management. Overall, understanding the features, management, and complications of inguinal hernias is crucial for proper diagnosis and treatment.
-
This question is part of the following fields:
- Surgery
-
-
Question 28
Incorrect
-
A 50-year-old man presents to the emergency department with sudden onset pain in his loin-to-groin region. He reports having experienced similar pain in the past, but never to this extent. Upon arrival, the following observations are recorded:
- Blood pressure: 110/85 mmHg
- Heart rate: 119 bpm
- Temperature: 38.6ºC
- Oxygen saturation: 98% on air
- Respiratory rate: 22/min
What is the most likely diagnosis and what is the definitive management?Your Answer: Ensure adequate fluid resuscitation and then manage in the community
Correct Answer: IV antibiotics and urgent renal decompression
Explanation:The patient’s symptoms and observations suggest that they are suffering from ureteric colic caused by urinary calculi, which may be accompanied by an infection leading to sepsis. In such cases, urgent renal decompression and IV antibiotics are necessary. While fluid resuscitation may help manage ureteric colic, it is not sufficient when there are signs of infection, and inpatient management is required. Although oral fluids, IV antibiotics, and analgesia may provide some relief, urgent renal decompression is the definitive treatment. While NSAIDs may be helpful in managing ureteric colic, they cannot be the sole treatment when there is an infection. Rectal diclofenac is often the preferred NSAID. An urgent nephrectomy is not necessary for this condition.
The management of renal stones involves initial medication and investigations, including an NSAID for analgesia and a non-contrast CT KUB for imaging. Stones less than 5mm may pass spontaneously, but more intensive treatment is needed for ureteric obstruction or renal abnormalities. Treatment options include shockwave lithotripsy, ureteroscopy, and percutaneous nephrolithotomy. Prevention strategies include high fluid intake, low animal protein and salt diet, and medication such as thiazides diuretics for hypercalciuria and allopurinol for uric acid stones.
-
This question is part of the following fields:
- Surgery
-
-
Question 29
Incorrect
-
A 65-year-old man with a history of atrial fibrillation and prostate cancer is undergoing a laparotomy for small bowel obstruction. His temperature during the operation is recorded at 34.8 ºC and his blood pressure is 98/57 mmHg. The surgeon observes that the patient is experiencing more bleeding than anticipated. What could be causing the excessive bleeding?
Your Answer: Use of intra-operative tranexamic acid
Correct Answer: Intra-operative hypothermia
Explanation:During the perioperative period, thermoregulation is hindered due to various factors such as the use of unwarmed intravenous fluids, exposure to a cold theatre environment, cool skin preparation fluids, and muscle relaxants that prevent shivering. Additionally, spinal or epidural anesthesia can lead to increased heat loss at the peripheries by reducing sympathetic tone and preventing peripheral vasoconstriction. The consequences of hypothermia can be significant, as it can affect the function of proteins and enzymes in the body, leading to slower metabolism of anesthetic drugs and reduced effectiveness of platelets, coagulation factors, and the immune system. Tranexamic acid, an anti-fibrinolytic medication used in trauma and major hemorrhage, can prevent the breakdown of fibrin. Intraoperative hypertension may cause excess bleeding, while active malignancy can lead to a hypercoagulable state. However, tumors may also have friable vessels due to neovascularization, which can result in excessive bleeding if cut erroneously. To prevent excessive bleeding, warfarin is typically stopped prior to surgery.
Managing Patient Temperature in the Perioperative Period
Thermoregulation in the perioperative period involves managing a patient’s temperature from one hour before surgery until 24 hours after the surgery. The focus is on preventing hypothermia, which is more common than hyperthermia. Hypothermia is defined as a temperature of less than 36.0ºC. NICE has produced a clinical guideline for suggested management of patient temperature. Patients are more likely to become hypothermic while under anesthesia due to the effects of anesthesia drugs and the fact that they are often wearing little clothing with large body areas exposed.
There are several risk factors for perioperative hypothermia, including ASA grade of 2 or above, major surgery, low body weight, large volumes of unwarmed IV infusions, and unwarmed blood transfusions. The pre-operative phase starts one hour before induction of anesthesia. The patient’s temperature should be measured, and if it is lower than 36.0ºC, active warming should be commenced immediately. During the intra-operative phase, forced air warming devices should be used for any patient with an anesthetic duration of more than 30 minutes or for patients at high risk of perioperative hypothermia regardless of anesthetic duration.
In the post-operative phase, the patient’s temperature should be documented initially and then repeated every 15 minutes until transfer to the ward. Patients should not be transferred to the ward if their temperature is less than 36.0ºC. Complications of perioperative hypothermia include coagulopathy, prolonged recovery from anesthesia, reduced wound healing, infection, and shivering. Managing patient temperature in the perioperative period is essential to ensure good outcomes, as even slight reductions in temperature can have significant effects.
-
This question is part of the following fields:
- Surgery
-
-
Question 30
Incorrect
-
A 50-year-old woman is planning to undergo a total hip replacement surgery in 3 months. She has a medical history of hypothyroidism, hypertension, and menopausal symptoms. Her current medications include Femoston (estradiol and dydrogesterone), levothyroxine, labetalol, and amlodipine. What recommendations should be provided to her regarding her medication regimen prior to the surgery?
Your Answer: No change necessary
Correct Answer: Stop Femoston 4 weeks before surgery
Explanation:Women who are taking hormone replacement therapy, such as Femoston, should discontinue its use four weeks prior to any elective surgeries. This is because the risk of venous thromboembolism increases with the use of HRT. It is important to note that no changes are necessary for medications such as labetalol and amlodipine, as they are safe to continue taking before and on the day of surgery. Additionally, levothyroxine is also safe to take before and on the day of surgery, so there is no need to discontinue its use one week prior to the procedure.
Venous thromboembolism (VTE) is a serious condition that can lead to severe health complications and even death. However, it is preventable. The National Institute for Health and Care Excellence (NICE) has updated its guidelines for 2018 to provide recommendations for the assessment and management of patients at risk of VTE in hospital. All patients admitted to the hospital should be assessed individually to identify risk factors for VTE development and bleeding risk. The department of health’s VTE risk assessment tool is recommended for medical and surgical patients. Patients with certain risk factors, such as reduced mobility, surgery, cancer, and comorbidities, are at increased risk of developing VTE. After assessing a patient’s VTE risk, healthcare professionals should compare it to their risk of bleeding to decide whether VTE prophylaxis should be offered. If indicated, VTE prophylaxis should be started as soon as possible.
There are two types of VTE prophylaxis: mechanical and pharmacological. Mechanical prophylaxis includes anti-embolism stockings and intermittent pneumatic compression devices. Pharmacological prophylaxis includes fondaparinux sodium, low molecular weight heparin (LMWH), and unfractionated heparin (UFH). The choice of prophylaxis depends on the patient’s individual risk factors and bleeding risk.
In general, medical patients deemed at risk of VTE after individual assessment are started on pharmacological VTE prophylaxis, provided that the risk of VTE outweighs the risk of bleeding and there are no contraindications. Surgical patients at low risk of VTE are treated with anti-embolism stockings, while those at high risk are treated with a combination of stockings and pharmacological prophylaxis.
Patients undergoing certain surgical procedures, such as hip and knee replacements, are recommended to receive pharmacological VTE prophylaxis to reduce the risk of VTE developing post-surgery. For fragility fractures of the pelvis, hip, and proximal femur, LMWH or fondaparinux sodium is recommended for a month if the risk of VTE outweighs the risk of bleeding.
Healthcare professionals should advise patients to stop taking their combined oral contraceptive pill or hormone replacement therapy four weeks before surgery and mobilize them as soon as possible after surgery. Patients should also ensure they are hydrated. By following these guidelines, healthcare professionals can help prevent VTE and improve patient outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 31
Correct
-
A 5-day-old neonate presents with sudden onset bilious vomiting. These episodes of vomiting are occurring frequently. On examination, he has a swollen, firm abdomen, is pale and appears dehydrated. He has not passed stool in the last 24 hours. He was born at term and there were no complications around the time of his delivery.
What is the probable diagnosis in this case?Your Answer: Malrotation
Explanation:Malrotation is most commonly seen in neonates within the first 30 days of life, and it often presents with bilious vomiting. The abdomen may initially be soft and non-tender, but if left untreated, it can lead to gut strangulation. In this scenario, the child’s distended and firm abdomen and lack of stool suggest this complication.
Appendicitis is rare in neonates and becomes more common in children over 3 years old. Symptoms of appendicitis in children typically include right-sided abdominal pain, fever, anorexia, and vomiting. Bilious vomiting, as seen in this case, would be unusual unless the condition had been present for a long time.
Necrotising enterocolitis usually presents in neonates with abdominal pain, swelling, diarrhoea with bloody stool, green/yellow vomit, lethargy, refusal to eat, and lack of weight gain. It is more common in premature babies and tends to have a more gradual onset, rather than presenting as an acutely unwell and dehydrated neonate.
Vomiting associated with pyloric stenosis is typically non-bilious and projectile, and it usually occurs between 4-8 weeks of age. Weight loss and dehydration are common at presentation, and visible peristalsis and a palpable olive-sized pyloric mass may be felt during a feed. Lack of ability to pass stool and a distended abdomen are not typical features of this condition.
Causes and Treatments for Bilious Vomiting in Neonates
Bilious vomiting in neonates can be caused by various disorders, including duodenal atresia, malrotation with volvulus, jejunal/ileal atresia, meconium ileus, and necrotising enterocolitis. Duodenal atresia occurs in 1 in 5000 births and is more common in babies with Down syndrome. It typically presents a few hours after birth and can be diagnosed through an abdominal X-ray that shows a double bubble sign. Treatment involves duodenoduodenostomy. Malrotation with volvulus is usually caused by incomplete rotation during embryogenesis and presents between 3-7 days after birth. An upper GI contrast study or ultrasound can confirm the diagnosis, and treatment involves Ladd’s procedure. Jejunal/ileal atresia is caused by vascular insufficiency in utero and occurs in 1 in 3000 births. It presents within 24 hours of birth and can be diagnosed through an abdominal X-ray that shows air-fluid levels. Treatment involves laparotomy with primary resection and anastomosis. Meconium ileus occurs in 15-20% of babies with cystic fibrosis and presents in the first 24-48 hours of life with abdominal distension and bilious vomiting. Diagnosis involves an abdominal X-ray that shows air-fluid levels, and a sweat test can confirm cystic fibrosis. Treatment involves surgical decompression, and segmental resection may be necessary for serosal damage. Necrotising enterocolitis occurs in up to 2.4 per 1000 births, with increased risks in prematurity and inter-current illness. It typically presents in the second week of life and can be diagnosed through an abdominal X-ray that shows dilated bowel loops, pneumatosis, and portal venous air. Treatment involves conservative and supportive measures for non-perforated cases, while laparotomy and resection are necessary for perforated cases or ongoing clinical deterioration.
-
This question is part of the following fields:
- Surgery
-
-
Question 32
Incorrect
-
An 80-year-old man was diagnosed with prostate cancer two years ago. He had radiotherapy. His prostate specific antigen level (PSA) had been normal until it began to rise four months ago.
He is well informed and asks if he should be on hormone treatment.
When should hormone treatment be initiated in this case?Your Answer: If he has a PSA doubling time of less than 6 months
Correct Answer: If he has a PSA doubling time of less than 3 months
Explanation:Hormonal Therapy for Biochemical Relapse in Prostate Cancer
According to NICE guidance, a biochemical relapse in prostate cancer, indicated by a rising PSA level, should not always lead to an immediate change in treatment. Hormonal therapy is not typically recommended for men with prostate cancer who experience a biochemical relapse unless they have symptomatic local disease progression, proven metastases, or a PSA doubling time of less than three months. In other words, if the cancer has not spread beyond the prostate and is not causing any symptoms, hormonal therapy may not be necessary. However, if the cancer has spread or is progressing rapidly, hormonal therapy may be recommended to slow down the cancer’s growth and improve the patient’s quality of life. It is important for patients to discuss their individual circumstances with their healthcare provider to determine the best course of action.
-
This question is part of the following fields:
- Surgery
-
-
Question 33
Incorrect
-
A 30-year-old woman is preparing for an elective laparoscopic cholecystectomy with general anesthesia and inquires about when she should discontinue her combined oral contraceptive pill. What is the best recommendation?
Your Answer: 2 weeks prior
Correct Answer: 4 weeks prior
Explanation:Stopping the combined oral contraceptive pill four weeks before the operation is recommended due to a higher likelihood of venous thromboembolism.
Preparation for surgery varies depending on whether the patient is undergoing an elective or emergency procedure. For elective cases, it is important to address any medical issues beforehand through a pre-admission clinic. Blood tests, urine analysis, and other diagnostic tests may be necessary depending on the proposed procedure and patient fitness. Risk factors for deep vein thrombosis should also be assessed, and a plan for thromboprophylaxis formulated. Patients are advised to fast from non-clear liquids and food for at least 6 hours before surgery, and those with diabetes require special management to avoid potential complications. Emergency cases require stabilization and resuscitation as needed, and antibiotics may be necessary. Special preparation may also be required for certain procedures, such as vocal cord checks for thyroid surgery or bowel preparation for colorectal cases.
-
This question is part of the following fields:
- Surgery
-
-
Question 34
Correct
-
An 80-year-old man presents to the surgical assessment unit for evaluation before an elective Hartmann's procedure in a week due to bowel cancer. He has a medical history of hypertension, atrial fibrillation, and a previous cerebrovascular accident. The registrar requests you to assess him before his surgery next week. During your review, you observe that he is currently on warfarin, and his INR is 2.6 today. All other blood tests are normal. What is the most appropriate approach to manage his anticoagulation during the peri-operative period?
Your Answer: Stop his warfarin and commence treatment dose low molecular weight heparin
Explanation:Managing anticoagulation during the peri-operative period can be difficult and depends on the type of anticoagulant used and the reasons for its use. It is important to assess each patient’s risk of venous thromboembolism and bleeding. In this case, the patient has a high risk of both thromboembolic disease and bleeding due to previous CVA, known AF, and major abdominal surgery. Therefore, the best approach would be to use a shorter-acting anticoagulant such as low molecular weight heparin at a treatment dose, while withholding warfarin. The low molecular weight heparin would be stopped the night before surgery, and mechanical prophylaxis would be used.
Venous thromboembolism (VTE) is a serious condition that can lead to severe health complications and even death. However, it is preventable. The National Institute for Health and Care Excellence (NICE) has updated its guidelines for 2018 to provide recommendations for the assessment and management of patients at risk of VTE in hospital. All patients admitted to the hospital should be assessed individually to identify risk factors for VTE development and bleeding risk. The department of health’s VTE risk assessment tool is recommended for medical and surgical patients. Patients with certain risk factors, such as reduced mobility, surgery, cancer, and comorbidities, are at increased risk of developing VTE. After assessing a patient’s VTE risk, healthcare professionals should compare it to their risk of bleeding to decide whether VTE prophylaxis should be offered. If indicated, VTE prophylaxis should be started as soon as possible.
There are two types of VTE prophylaxis: mechanical and pharmacological. Mechanical prophylaxis includes anti-embolism stockings and intermittent pneumatic compression devices. Pharmacological prophylaxis includes fondaparinux sodium, low molecular weight heparin (LMWH), and unfractionated heparin (UFH). The choice of prophylaxis depends on the patient’s individual risk factors and bleeding risk.
In general, medical patients deemed at risk of VTE after individual assessment are started on pharmacological VTE prophylaxis, provided that the risk of VTE outweighs the risk of bleeding and there are no contraindications. Surgical patients at low risk of VTE are treated with anti-embolism stockings, while those at high risk are treated with a combination of stockings and pharmacological prophylaxis.
Patients undergoing certain surgical procedures, such as hip and knee replacements, are recommended to receive pharmacological VTE prophylaxis to reduce the risk of VTE developing post-surgery. For fragility fractures of the pelvis, hip, and proximal femur, LMWH or fondaparinux sodium is recommended for a month if the risk of VTE outweighs the risk of bleeding.
Healthcare professionals should advise patients to stop taking their combined oral contraceptive pill or hormone replacement therapy four weeks before surgery and mobilize them as soon as possible after surgery. Patients should also ensure they are hydrated. By following these guidelines, healthcare professionals can help prevent VTE and improve patient outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 35
Correct
-
A patient is having an emergency laparotomy for a likely sigmoid perforation secondary to diverticular disease. She is 84, has known ischaemic heart disease under medical management, and was in new atrial fibrillation (AF) pre-operatively. You find that she has two quadrant peritonitis and despite fluid resuscitation her blood pressure is becoming low. You start Noradrenaline. She is going to intensive care unit (ICU) postoperatively.
Which scoring system is generally used in this context to predict outcome?Your Answer: P-POSSUM
Explanation:Scoring Systems Used in Critical Care: An Overview
In critical care, various scoring systems are used to assess patient outcomes and predict mortality and morbidity. The most commonly used systems include POSSUM, P-POSSUM, APACHE, SOFA, SAPS, and TISS.
POSSUM (Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity) is a scoring system that utilizes surgical data to predict outcomes in emergency abdominal surgery. P-POSSUM is a modification of POSSUM that is more accurate in predicting outcomes.
APACHE (Acute Physiology and Chronic Health Evaluation) is an ICU scoring system that is based on physiology. SOFA (Sequential Organ Failure Assessment) and SAPS (Simplified Acute Physiology Score) are also ICU scoring systems that are based on physiology.
TISS (Therapeutic Intervention Scoring System) is a scoring system that measures patient interventions in the ICU. It is used to measure ICU workload and cost, rather than patient outcome.
In critical care, these scoring systems are essential tools for assessing patient outcomes and predicting mortality and morbidity. Each system has its own strengths and limitations, and healthcare professionals must choose the most appropriate system for each patient.
-
This question is part of the following fields:
- Surgery
-
-
Question 36
Incorrect
-
A 50-year-old man is involved in a high-speed car accident and suffers from severe injuries. During the initial assessment, it is discovered that he has free fluid in his abdominal cavity on FAST scan. Due to his unstable condition, he is taken to the operating theatre for laparotomy. The surgeons identify the main sources of bleeding in the mesentery of the small bowel and tie them off. The injured sections of the small bowel are stapled off but not reanastamosed. However, there are multiple tiny areas of bleeding, especially in the wound edges, which the surgeons refer to as a general ooze. The abdomen is closed, and the patient is admitted to the intensive care unit. The surgeons plan to return to the theatre to repair the small bowel 24 hours later when the patient is more stable. What is the principle of damage control laparotomy?
Your Answer: Laparotomy performed to stop bleeding
Correct Answer: Laparotomy performed to restore normal physiology
Explanation:Damage Control Laparotomy: A Life-Saving Procedure
Damage control laparotomy is a surgical procedure performed when prolonged surgery would further deteriorate the patient’s physiology. Patients who require this procedure often present with a triad of acidosis, hypothermia, and coagulopathy. The primary goal of this procedure is to stop life-threatening bleeding and reduce contamination, rather than reconstructing damaged tissue and reanastomosing the bowel. For instance, the surgeon may staple off a perforated bowel to prevent further contamination.
After the abbreviated laparotomy for damage control, the patient is transferred to the intensive care unit for resuscitation. The medical team focuses on correcting the patient’s abnormal physiology, such as warming up the patient and correcting coagulopathy. The patient is closely monitored until their physiology is closer to normal, which usually takes 24 to 48 hours.
Once the patient’s physiology has improved, the surgeon performs an operation to reconstruct the anatomy. This approach allows the patient to recover from the initial surgery and stabilize before undergoing further procedures. Damage control laparotomy is a life-saving procedure that can prevent further deterioration of the patient’s condition and increase their chances of survival.
-
This question is part of the following fields:
- Surgery
-
-
Question 37
Incorrect
-
A 72-year-old male is recovering from carotid endarterectomy for an 80% stenosis of the carotid artery. After a smooth recovery period, the registrar examined the patient's cranial nerves. Upon requesting the patient to protrude his tongue, it was observed that the tongue deviated towards the right side of the patient. Which nerve has been impacted?
Your Answer: Facial
Correct Answer: Right hypoglossal
Explanation:During a carotid endarterectomy, there is a significant chance of damaging the hypoglossal nerve on the same side as the procedure. This nerve is responsible for providing motor function to the tongue and muscles that depress the hyoid bone. Additionally, the accessory nerve is responsible for supplying the sternocleidomastoid and trapezius muscles.
Nerve Lesions in Surgery: Risks and Procedures
During surgical procedures, there is a risk of iatrogenic nerve injury, which can have significant consequences for patients and lead to legal issues. Several operations are associated with specific nerve lesions, including posterior triangle lymph node biopsy and accessory nerve lesion, Lloyd Davies stirrups and common peroneal nerve, thyroidectomy and laryngeal nerve, anterior resection of rectum and hypogastric autonomic nerves, axillary node clearance and long thoracic nerve, thoracodorsal nerve, and intercostobrachial nerve, inguinal hernia surgery and ilioinguinal nerve, varicose vein surgery and sural and saphenous nerves, posterior approach to the hip and sciatic nerve, and carotid endarterectomy and hypoglossal nerve.
To minimize the incidence of nerve lesions, surgeons must have a sound anatomical understanding of the tissue planes involved in commonly performed procedures. Nerve injuries often occur when surgeons operate in unfamiliar tissue planes or use haemostats blindly, which is not recommended. By being aware of the risks and taking appropriate precautions, surgeons can reduce the likelihood of nerve injuries during surgery.
-
This question is part of the following fields:
- Surgery
-
-
Question 38
Incorrect
-
An 80-year-old man comes to the clinic with a complaint of worsening voiding-predominant lower urinary tract symptoms for the past year, including poor flow, hesitancy, and terminal dribbling. There are no red flag features. The patient's international prostate symptom score is 15, and prostate examination reveals a slightly enlarged, smooth prostate. Urine dipstick results are normal, and blood tests show normal renal function and a normal prostate-specific antigen level.
What is the most appropriate class of medication to consider starting for this patient?Your Answer: GnRH analogues
Correct Answer: Alpha-1 antagonists
Explanation:For patients with troublesome symptoms of benign prostatic hyperplasia, alpha-1 antagonists are the first-line medication to consider. This is particularly true for patients with predominantly voiding symptoms, such as the patient in this case who has an IPPS of 15. Alpha-1 agonists like tamsulosin and alfuzosin are recommended for patients with moderate-to-severe voiding symptoms (IPSS ≥ 8) and are likely to provide relief for this patient’s symptoms.
On the other hand, 5-alpha reductase inhibitors are only indicated for patients with significantly enlarged prostates, which is not the case for this patient. Therefore, they are not appropriate for him at this time. Similarly, anti-muscarinic medication is only recommended for patients with a combination of storage and voiding symptoms that persist after treatment with an alpha-blocker alone. Since this patient only reports voiding symptoms and is not currently on any treatment, this class of medication is not indicated for him.
Finally, GnRH analogues are commonly used in prostate cancer treatment, but they have been found to have a poor side effect profile when used for benign prostatic hypertrophy. As a result, they are not appropriate for this patient.
Benign prostatic hyperplasia (BPH) is a common condition that affects older men, with around 50% of 50-year-old men showing evidence of BPH and 30% experiencing symptoms. The risk of BPH increases with age, with around 80% of 80-year-old men having evidence of the condition. BPH typically presents with lower urinary tract symptoms (LUTS), which can be categorised into voiding symptoms (obstructive) and storage symptoms (irritative). Complications of BPH can include urinary tract infections, retention, and obstructive uropathy.
Assessment of BPH may involve dipstick urine tests, U&Es, and PSA tests. A urinary frequency-volume chart and the International Prostate Symptom Score (IPSS) can also be used to assess the severity of LUTS and their impact on quality of life. Management options for BPH include watchful waiting, alpha-1 antagonists, 5 alpha-reductase inhibitors, combination therapy, and surgery. Alpha-1 antagonists are considered first-line treatment for moderate-to-severe voiding symptoms, while 5 alpha-reductase inhibitors may be indicated for patients with significantly enlarged prostates and a high risk of progression. Combination therapy and antimuscarinic drugs may also be used in certain cases. Surgery, such as transurethral resection of the prostate (TURP), may be necessary in severe cases.
-
This question is part of the following fields:
- Surgery
-
-
Question 39
Incorrect
-
A 30-year-old male visits his general practitioner (GP) complaining of swelling in his testicles. He reports a soft sensation on the top of his left testicle but denies any pain or issues with urination or erections. The GP orders an ultrasound, and the results show a mild varicocele on the left side without other abnormalities detected. What is the recommended next step in managing this patient?
Your Answer: Recommend semen cryopreservation
Correct Answer: Reassure and observe
Explanation:Common Scrotal Problems and Their Features
Epididymal cysts, hydroceles, and varicoceles are the most common scrotal problems seen in primary care. Epididymal cysts are usually found posterior to the testicle and are separate from the body of the testicle. They may be associated with conditions such as polycystic kidney disease, cystic fibrosis, and von Hippel-Lindau syndrome. Diagnosis is confirmed by ultrasound, and management is usually supportive, although surgical removal or sclerotherapy may be attempted for larger or symptomatic cysts.
Hydroceles, on the other hand, describe the accumulation of fluid within the tunica vaginalis. They may be communicating or non-communicating, and may develop secondary to conditions such as epididymo-orchitis, testicular torsion, or testicular tumors. Hydroceles are usually soft, non-tender swellings of the hemi-scrotum that transilluminate with a pen torch. Diagnosis may be clinical, but ultrasound is required if there is any doubt about the diagnosis or if the underlying testis cannot be palpated. Management depends on the severity of the presentation, with infantile hydroceles generally repaired if they do not resolve spontaneously by the age of 1-2 years.
Varicoceles, on the other hand, are abnormal enlargements of the testicular veins that are usually asymptomatic but may be associated with subfertility. They are much more common on the left side and are classically described as a bag of worms. Diagnosis is confirmed by ultrasound with Doppler studies, and management is usually conservative, although surgery may be required if the patient is troubled by pain. There is ongoing debate regarding the effectiveness of surgery to treat infertility.
-
This question is part of the following fields:
- Surgery
-
-
Question 40
Incorrect
-
A young laborer presents to the Emergency department with complaints of pain in their middle finger. Upon examination, the finger appears swollen and is held in a partially flexed position. Passive extension elicits pain and there is tenderness over the flexor sheath. What is the probable diagnosis?
Your Answer: Midpalmar space infection
Correct Answer: Suppurative flexor tenosynovitis
Explanation:The Four Cardinal Signs of Suppurative Flexor Tenosynovitis
Suppurative flexor tenosynovitis is a serious infection that affects the tendons and synovial sheaths of the fingers. Kanavel, a renowned physician, identified four cardinal signs of this condition. The first sign is a flexed posture, which is caused by pain and swelling in the affected area. The second sign is fusiform swelling, which refers to a sausage-like swelling of the finger. The third sign is pain on passive extension, which means that the finger hurts when it is straightened. The fourth sign is flexor sheath tenderness, which is tenderness along the tendon sheath.
Deep potential space infections, such as mid palmar and thenar space infections, are made worse by flexion. This is because flexion causes the infected area to become more compressed, which can lead to further swelling and pain. It is important to recognize these cardinal signs of suppurative flexor tenosynovitis and seek medical attention immediately if they are present. Early diagnosis and treatment can help prevent serious complications, such as loss of function or even amputation.
-
This question is part of the following fields:
- Surgery
-
-
Question 41
Incorrect
-
A 5-year-old boy is scheduled for surgery to remove a sebaceous cyst on his neck. During examination, a sebaceous cystic swelling measuring 2 cm in diameter is found in the left anterior neck triangle near the midline, with a punctum on top. The surgeon makes an elliptical incision around the cyst and removes the skin with the central punctum. The cyst is then removed to a depth of 1 cm. You have been tasked with closing the skin wound. What is the best option?
Your Answer: Staples
Correct Answer: Monocryl
Explanation:Choosing the Right Suture Material for Skin Closure
When it comes to closing a skin defect, several factors need to be considered, including the location of the wound, required tensile strength, cosmesis, and ease of stitch removal, especially in children. Monocryl, a monofilament absorbable suture, is the best choice for achieving optimal cosmetic results. Nylon, another monofilament suture, is also a reasonable option, but Monocryl’s absorbable nature eliminates the need for stitch removal, making it more practical for children. Steri-strips may not provide enough strength to keep the wound closed, while staples are more likely to cause scarring. Silk, a multi-filament non-absorbable suture, is not ideal for achieving optimal cosmesis. Therefore, choosing the right suture material is crucial for achieving the best possible outcome in skin closure.
-
This question is part of the following fields:
- Surgery
-
-
Question 42
Incorrect
-
A 28-year-old woman comes to the clinic with a lump in her left breast that has appeared suddenly over the past month. She is very concerned about it and describes it as being located below the nipple. Additionally, she has noticed mild tenderness to the lump. She cannot recall any triggers or trauma that may have caused it. During the examination, a well-defined, 2 cm mobile mass is palpated in the left breast. There is no skin discoloration or discharge present. What is the most probable diagnosis?
Your Answer: Breast abscess
Correct Answer: Fibroadenoma
Explanation:If a female under 30 years old has a lump that is non-tender, discrete, and mobile, it is likely a fibroadenoma. This type of lump can sometimes be tender. Fibroadenosis, on the other hand, is more common in older women and is described as painful and lumpy, especially around menstruation. Ductal carcinoma is also more common in older women and can present with a painless lump, nipple changes, nipple discharge, and changes in the skin’s contour. Fat necrosis lumps tend to be hard and irregular, while an abscess would show signs of inflammation such as redness, fever, and pain.
Breast Disorders: Common Features and Characteristics
Breast disorders are a common occurrence among women of all ages. The most common breast disorders include fibroadenoma, fibroadenosis, breast cancer, Paget’s disease of the breast, mammary duct ectasia, duct papilloma, fat necrosis, and breast abscess. Fibroadenoma is a non-tender, highly mobile lump that is common in women under the age of 30. Fibroadenosis, on the other hand, is characterized by lumpy breasts that may be painful, especially before menstruation. Breast cancer is a hard, irregular lump that may be accompanied by nipple inversion or skin tethering. Paget’s disease of the breast is associated with a reddening and thickening of the nipple/areola, while mammary duct ectasia is characterized by dilation of the large breast ducts, which may cause a tender lump around the areola and a green nipple discharge. Duct papilloma is characterized by local areas of epithelial proliferation in large mammary ducts, while fat necrosis is more common in obese women with large breasts and may mimic breast cancer. Breast abscess, on the other hand, is more common in lactating women and is characterized by a red, hot, and tender swelling. Lipomas and sebaceous cysts may also develop around the breast tissue.
Common Features and Characteristics of Breast Disorders
Breast disorders are a common occurrence among women of all ages. The most common breast disorders include fibroadenoma, fibroadenosis, breast cancer, Paget’s disease of the breast, mammary duct ectasia, duct papilloma, fat necrosis, and breast abscess. Each of these disorders has its own unique features and characteristics that can help identify them. Understanding these features and characteristics can help women identify potential breast disorders and seek appropriate medical attention. It is important to note that while some breast disorders may be benign, others may be malignant or premalignant, and further investigation is always warranted. Regular breast exams and mammograms can also help detect breast disorders early, increasing the chances of successful treatment.
-
This question is part of the following fields:
- Surgery
-
-
Question 43
Incorrect
-
A 25-year-old man is in a car accident and initially has a GCS of 15. However, upon arrival at the hospital and being monitored in a side room, he is later found to have a GCS of 3 and a blown right pupil. What is the most likely cause of this sudden deterioration?
Your Answer: Subarachnoid haemorrhage
Correct Answer: Transtentorial herniation
Explanation:A blown right pupil is indicative of compression of the third cranial nerve, which is most commonly caused by an extradural bleed. However, as this option is not available, the process of transtentorial herniation would be the most appropriate answer. While intraventricular bleeds are more prevalent in premature neonates, deterioration due to hydrocephalus is a more gradual process.
Types of Traumatic Brain Injury
Traumatic brain injury can result in primary and secondary brain injury. Primary brain injury can be focal or diffuse. Diffuse axonal injury occurs due to mechanical shearing, which causes disruption and tearing of axons. intracranial haematomas can be extradural, subdural, or intracerebral, while contusions may occur adjacent to or contralateral to the side of impact. Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory processes are disrupted following trauma rendering the brain more susceptible to blood flow changes and hypoxia. The Cushings reflex often occurs late and is usually a pre-terminal event.
Extradural haematoma is bleeding into the space between the dura mater and the skull. It often results from acceleration-deceleration trauma or a blow to the side of the head. The majority of epidural haematomas occur in the temporal region where skull fractures cause a rupture of the middle meningeal artery. Subdural haematoma is bleeding into the outermost meningeal layer. It most commonly occurs around the frontal and parietal lobes. Risk factors include old age, alcoholism, and anticoagulation. Subarachnoid haemorrhage classically causes a sudden occipital headache. It usually occurs spontaneously in the context of a ruptured cerebral aneurysm but may be seen in association with other injuries when a patient has sustained a traumatic brain injury. Intracerebral haematoma is a collection of blood within the substance of the brain. Causes/risk factors include hypertension, vascular lesion, cerebral amyloid angiopathy, trauma, brain tumour, or infarct. Patients will present similarly to an ischaemic stroke or with a decrease in consciousness. CT imaging will show a hyperdensity within the substance of the brain. Treatment is often conservative under the care of stroke physicians, but large clots in patients with impaired consciousness may warrant surgical evacuation.
-
This question is part of the following fields:
- Surgery
-
-
Question 44
Incorrect
-
A 65-year-old man is scheduled for a cystoscopy for symptoms of nocturia and urinary frequency with poor stream (terminal dribbling). On examination, on the day of surgery, you notice he has an ejection systolic murmur radiating to the carotids and he describes getting very breathless on stairs.
How would you proceed?Your Answer: Proceed with surgery, but give a dose of prophylactic antibiotics
Correct Answer: Defer surgery until he is seen by Cardiology and an echocardiography report is available
Explanation:Preoperative Management of Patients with Aortic Stenosis
Explanation:
Patients with aortic stenosis require careful preoperative management to minimize the risk of cardiac complications during non-cardiac surgery. Before proceeding with any elective procedure, it is essential to evaluate the severity of the stenosis and the functional status of the heart. This can be done through an echocardiogram and a cardiology opinion.
If the patient is symptomatic, such as having shortness of breath on exertion or an ejection systolic murmur on auscultation, it is not advisable to proceed with the operation until an up-to-date echocardiogram has been performed and a cardiology opinion offered. Severe stenosis can become a problem in situations of stress, such as exercise or intraoperatively, where the heart cannot increase the cardiac output to meet the increased demands. This puts patients with aortic stenosis at a high risk of cardiac complications during non-cardiac surgery.
There is no evidence to suggest antibiotic prophylaxis for endocarditis in patients with valvular disease undergoing surgery. Aortic or mitral stenosis are relative contraindications to spinal anesthesia, and other relative contraindications include neurological disease and systemic sepsis. Absolute contraindications to spinal anesthesia include localized sepsis at the site where a spinal anesthetic would be sited, anticoagulated patient, and patient refusal.
In conclusion, preoperative management of patients with aortic stenosis requires careful evaluation of the severity of the stenosis and the functional status of the heart. It is essential to postpone the operation until an echocardiogram has been performed to assess the severity of the stenosis and the functional status of the heart. The patient will need to be reviewed/discussed with Cardiology once the echocardiography results become available to advise on the safety of the operation.
-
This question is part of the following fields:
- Surgery
-
-
Question 45
Incorrect
-
A 48-year-old woman visits her GP with worries about a lump she has discovered on her right breast accompanied by a green discharge from her nipple. During the examination, a tender lump is found on her right breast near the areola. The lump is not discoloured or warm to the touch. What is the most probable cause of this presentation?
Your Answer: Fibroadenosis
Correct Answer: Duct ectasia
Explanation:The patient is displaying symptoms consistent with duct ectasia, a benign breast condition that often occurs during breast involution and is characterized by thick green nipple discharge and a lump around the peri-areolar area. This condition is common among women going through menopause and is caused by the widening and shortening of the terminal breast ducts near the nipple.
Breast abscesses are more frequently observed in lactating women and are typically accompanied by redness and warmth in the affected area. Duct papillomas, on the other hand, tend to affect larger mammary ducts and result in nipple discharge that is tinged with blood. Fibroadenosis, which can cause breast pain and lumps, is also common among middle-aged women. Fibroadenomas, which are non-tender, highly mobile lumps, are typically found in women under the age of 30.
Understanding Duct Ectasia
Duct ectasia is a condition that affects the terminal breast ducts located within 3 cm of the nipple. It is a common condition that becomes more prevalent as women age. The condition is characterized by the dilation and shortening of the ducts, which can cause nipple retraction and creamy nipple discharge. It is important to note that duct ectasia can be mistaken for periductal mastitis, which is more common in younger women who smoke. Periductal mastitis typically presents with infections around the periareolar or subareolar areas and may recur.
When dealing with troublesome nipple discharge, treatment options may include microdochectomy for younger patients or total duct excision for older patients.
-
This question is part of the following fields:
- Surgery
-
-
Question 46
Incorrect
-
A 50-year-old woman visited her doctor with complaints of intense pain in the anal area. She recalled that the pain began after straining during a bowel movement. She had been constipated for the past week and had been using over-the-counter laxatives. During the examination, the doctor noticed a painful, firm, blue-black lump at the edge of the anus. What is the probable cause of her symptoms?
Your Answer: External haemorrhoid
Correct Answer: Thrombosed haemorrhoid
Explanation:Thrombosed haemorrhoids are characterized by severe pain and the presence of a tender lump. Upon examination, a purplish, swollen, and tender subcutaneous perianal mass can be observed. If the patient seeks medical attention within 72 hours of onset, referral for excision may be necessary. However, if the condition has progressed beyond this timeframe, patients can typically manage their symptoms with stool softeners, ice packs, and pain relief medication. Symptoms usually subside within 10 days.
-
This question is part of the following fields:
- Surgery
-
-
Question 47
Incorrect
-
A 53-year-old man presents to the emergency department with a 4-day history of left-sided scrotal pain and swelling with associated dysuria and increased frequency. He has had unprotected sexual intercourse with his wife, who uses hormonal contraception and is his only partner. The patient has a past medical history of type 2 diabetes.
On examination, the left hemiscrotum is erythematosus and diffusely swollen. Elevating the testis alleviates the pain.
What would be the most appropriate next step in managing this patient, considering the likely diagnosis?Your Answer: Arrange urethral swab sample for microscopy and culture
Correct Answer: Arrange mid-stream urine sample for microscopy and culture
Explanation:Epididymo-orchitis is likely caused by enteric organisms, such as E. coli, in individuals with a low risk of sexually-transmitted infections (STIs), such as married men in their 50s with a single long-term partner. Therefore, the most appropriate next step would be to arrange a mid-stream urine sample for microscopy and culture to guide antibiotic treatment. This patient has subacute onset of testicular pain and swelling with associated dysuria, and his pain is relieved when elevating the testis (positive Prehn’s sign), making a diagnosis of testicular torsion less likely. A urethral swab sample for microscopy and culture is no longer the initial investigation of choice, and a urine sample for nucleic acid amplification tests (NAAT) is not appropriate in this case. Urgent referral for a same-day testicular ultrasound scan is also not necessary as testicular torsion is rare in patients over 35 years of age and does not present with dysuria.
Epididymo-orchitis is a condition where the epididymis and/or testes become infected, leading to pain and swelling. It is commonly caused by infections spreading from the genital tract or bladder, with Chlamydia trachomatis and Neisseria gonorrhoeae being the usual culprits in sexually active younger adults, while E. coli is more commonly seen in older adults with a low-risk sexual history. Symptoms include unilateral testicular pain and swelling, with urethral discharge sometimes present. Testicular torsion, which can cause ischaemia of the testicle, is an important differential diagnosis and needs to be excluded urgently, especially in younger patients with severe pain and an acute onset.
Investigations are guided by the patient’s age, with sexually transmitted infections being assessed in younger adults and a mid-stream urine (MSU) being sent for microscopy and culture in older adults with a low-risk sexual history. Management guidelines from the British Association for Sexual Health and HIV (BASHH) recommend ceftriaxone 500 mg intramuscularly as a single dose, plus doxycycline 100 mg orally twice daily for 10-14 days if the organism causing the infection is unknown. Further investigations are recommended after treatment to rule out any underlying structural abnormalities.
-
This question is part of the following fields:
- Surgery
-
-
Question 48
Incorrect
-
You are conducting an annual health review for a 60-year-old man who has hypertension, a history of myocardial infarction 18 months ago, and depression. He is currently taking amlodipine, ramipril, sertraline, atorvastatin, and aspirin. The patient reports feeling generally well, but he is experiencing erectile dysfunction since starting his medications after his heart attack. Which medication is most likely responsible for this symptom?
Your Answer: Aspirin
Correct Answer: Sertraline
Explanation:Erectile dysfunction is a side-effect that is considered uncommon for amlodipine and ramipril, according to the BNF. However, SSRIs are a frequent cause of sexual dysfunction, making them the most probable medication to result in ED.
Erectile dysfunction (ED) is a condition where a man is unable to achieve or maintain an erection that is sufficient for sexual activity. It is not a disease but a symptom that can be caused by organic, psychogenic, or mixed factors. It is important to differentiate between the causes of ED, with gradual onset of symptoms, lack of tumescence, and normal libido favoring an organic cause, while sudden onset of symptoms, decreased libido, and major life events favoring a psychogenic cause. Risk factors for ED include cardiovascular disease, alcohol use, and certain medications.
To assess for ED, it is recommended to measure lipid and fasting glucose serum levels to calculate cardiovascular risk, as well as free testosterone levels in the morning. If free testosterone is low or borderline, further assessment may be needed. PDE-5 inhibitors, such as sildenafil, are the first-line treatment for ED and should be prescribed to all patients regardless of the cause. Vacuum erection devices can be used as an alternative for those who cannot or will not take PDE-5 inhibitors.
For young men who have always had difficulty achieving an erection, referral to urology is appropriate. Additionally, people with ED who cycle for more than three hours per week should be advised to stop. Overall, ED is a common condition that can be effectively managed with appropriate treatment.
-
This question is part of the following fields:
- Surgery
-
-
Question 49
Correct
-
A 75-year-old woman presents to the oncology clinic with a breast lump that was confirmed to be malignant through a biopsy. Cancer receptor testing reveals the presence of oestrogen receptors, and as she is postmenopausal, the plan is to start her on an aromatase inhibitor. However, due to potential adverse effects of the medication, a DEXA scan is conducted before initiating treatment. What is the name of the drug that the patient is supposed to start taking?
Your Answer: Anastrozole
Explanation:Anastrozole and letrozole are drugs that inhibit aromatase, reducing the production of oestrogen in the body. They are commonly used to treat oestrogen receptor-positive breast cancer in postmenopausal women, as aromatisation is the primary source of oestrogen in this group.
Docetaxel is a taxane drug that is often added to chemotherapy regimens for breast cancer treatment. It works by destroying fast-replicating cancer cells and does not affect aromatisation.
Levonorgestrel is a progestin that mimics the effects of progesterone. It is used in combination with oestrogen for birth control and menopausal hormone therapy, but has no role in the management of breast cancer. In fact, research suggests that its use may slightly increase the risk of malignancy.
Tamoxifen is a selective oestrogen receptor modulator (SERM) that directly blocks cancer oestrogen receptors, inhibiting their growth. It is commonly used to treat oestrogen receptor-positive breast cancer.
Anti-oestrogen drugs are used in the management of oestrogen receptor-positive breast cancer. Selective oEstrogen Receptor Modulators (SERM) such as Tamoxifen act as an oestrogen receptor antagonist and partial agonist. However, Tamoxifen can cause adverse effects such as menstrual disturbance, hot flashes, venous thromboembolism, and endometrial cancer. On the other hand, aromatase inhibitors like Anastrozole and Letrozole reduce peripheral oestrogen synthesis, which is important in postmenopausal women. Anastrozole is used for ER +ve breast cancer in this group. However, aromatase inhibitors can cause adverse effects such as osteoporosis, hot flashes, arthralgia, myalgia, and insomnia. NICE recommends a DEXA scan when initiating a patient on aromatase inhibitors for breast cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 50
Incorrect
-
A 68-year-old man is undergoing investigation for iron deficiency anaemia. He has no notable symptoms except for mild hypertension. An outpatient CT scan of his abdomen and pelvis reveals no cause for anaemia but incidentally discovers an abnormal dilation of the abdominal aorta measuring 4.4 cm in diameter. The patient reports having undergone an ultrasound scan of his abdomen 6 months ago as part of the national AAA screening program, which showed a dilation of 3 cm in diameter. What is the best course of action for management?
Your Answer: Antihypertensive medication
Correct Answer: Urgent endovascular aneurysm repair
Explanation:Patients with rapidly enlarging abdominal aortic aneurysms should undergo surgical repair, preferably with endovascular aneurysm repair. Hypertension is not the cause of the aneurysm and antihypertensive medication is not the appropriate management. Open repair as an emergency is not necessary as the patient is stable and asymptomatic. Intravenous iron infusion is not necessary as the patient’s iron deficiency anaemia is not causing any problems and oral supplementation is more appropriate. Monitoring with a re-scan in 3 months is not appropriate as rapidly enlarging aneurysms should be repaired.
Abdominal aortic aneurysm (AAA) is a condition that often develops without any symptoms. However, a ruptured AAA can be fatal, which is why it is important to screen patients for this condition. Screening involves a single abdominal ultrasound for males aged 65. The results of the screening are interpreted based on the width of the aorta. If the width is less than 3 cm, no further action is needed. If it is between 3-4.4 cm, the patient should be rescanned every 12 months. For a width of 4.5-5.4 cm, the patient should be rescanned every 3 months. If the width is 5.5 cm or more, the patient should be referred to vascular surgery within 2 weeks for probable intervention.
For patients with a low risk of rupture, which includes those with a small or medium aneurysm (i.e. aortic diameter less than 5.5 cm) and no symptoms, abdominal US surveillance should be conducted on the time-scales outlined above. Additionally, cardiovascular risk factors should be optimized, such as quitting smoking. For patients with a high risk of rupture, which includes those with a large aneurysm (i.e. aortic diameter of 5.5 cm or more) or rapidly enlarging aneurysm (more than 1 cm/year) or those with symptoms, they should be referred to vascular surgery within 2 weeks for probable intervention. Treatment for these patients may involve elective endovascular repair (EVAR) or open repair if EVAR is not suitable. EVAR involves placing a stent into the abdominal aorta via the femoral artery to prevent blood from collecting in the aneurysm. However, a complication of EVAR is an endo-leak, which occurs when the stent fails to exclude blood from the aneurysm and usually presents without symptoms on routine follow-up.
-
This question is part of the following fields:
- Surgery
-
-
Question 51
Correct
-
A 50-year-old male with a history of heavy alcohol consumption presents with sudden onset epigastric pain that spreads to the right side. During examination, his sclera appear yellow, and he experiences tenderness in the right upper quadrant of his abdomen with localized guarding. His vital signs are as follows: heart rate 95/min, blood pressure 80/50 mmHg, saturation 99% on 2L, temperature 39.5ºC, and Glasgow coma score 14/15 (confused speech). Which of the following diagnoses could account for these symptoms?
Your Answer: Ascending cholangitis
Explanation:Charcot’s cholangitis triad consists of three symptoms: fever, jaundice, and right upper quadrant pain. Meanwhile, Reynolds Pentad, which includes jaundice, right upper quadrant pain, fever/rigors, shock, and altered mental status, is linked to ascending cholangitis. Before conducting further investigations on the biliary tree, such as ultrasound or magnetic resonance cholangiopancreatography for common bile duct stones, or endoscopic retrograde cholangiopancreatography, the patient must first receive adequate resuscitation.
Understanding Ascending Cholangitis
Ascending cholangitis is a bacterial infection that affects the biliary tree, with E. coli being the most common culprit. This condition is often associated with gallstones, which can predispose individuals to the infection. Patients with ascending cholangitis may present with Charcot’s triad, which includes fever, right upper quadrant pain, and jaundice. However, this triad is only present in 20-50% of cases. Other common symptoms include hypotension and confusion. In severe cases, Reynolds’ pentad may be observed, which includes the additional symptoms of hypotension and confusion.
To diagnose ascending cholangitis, ultrasound is typically used as a first-line investigation to look for bile duct dilation and stones. Raised inflammatory markers may also be observed. Treatment involves intravenous antibiotics and endoscopic retrograde cholangiopancreatography (ERCP) after 24-48 hours to relieve any obstruction.
Overall, ascending cholangitis is a serious condition that requires prompt diagnosis and treatment. Understanding the symptoms and risk factors associated with this condition can help individuals seek medical attention early and improve their chances of a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 52
Incorrect
-
A 27-year-old cyclist is struck by a bus traveling at 30mph. Despite not wearing a helmet, he is conscious upon arrival with a GCS of 3/15 and is intubated. A CT scan reveals evidence of cerebral contusion, but there are no localizing clinical signs. What is the best course of action?
Your Answer: Administration of intravenous mannitol
Correct Answer: Insertion of intracranial pressure monitoring device
Explanation:Intracranial pressure monitoring will aid in the management of this patient who is at risk of developing elevated ICP in the coming days.
Patients with head injuries should be managed according to ATLS principles and extracranial injuries should be managed alongside cranial trauma. There are different types of traumatic brain injuries, including extradural hematoma, subdural hematoma, and subarachnoid hemorrhage. Primary brain injury may be focal or diffuse, and secondary brain injury can occur due to cerebral edema, ischemia, infection, or herniation. Management may include IV mannitol/furosemide, decompressive craniotomy, and ICP monitoring. Pupillary findings can provide information on the location and severity of the injury.
-
This question is part of the following fields:
- Surgery
-
-
Question 53
Incorrect
-
A 22-year-old female comes to the emergency department complaining of lower abdominal pain. The pain began in the middle and is now concentrated on the right side. She reports that the pain is an 8 out of 10 on the pain scale. She is sexually active and not using any contraception except for condoms. During the examination, she experiences pain in the right iliac fossa and rebound tenderness. What initial tests should be conducted during admission to exclude a possible diagnosis?
Your Answer: Trans-vaginal ultrasound scan
Correct Answer: Urine human chorionic gonadotropin
Explanation:When a woman experiences pain in the right iliac fossa, it is important to consider gynecological issues as a possible cause of acute abdomen. One potential cause is an ectopic pregnancy, which can manifest in various ways, including abdominal pain. It is important to inquire about the woman’s menstrual cycle, but vaginal bleeding does not necessarily rule out an ectopic pregnancy, as it can be mistaken for a period.
To aid in diagnosis and management, a pregnancy test should be conducted. Even if a woman presents with non-specific symptoms, NICE guidelines recommend offering a pregnancy test if pregnancy is a possibility. A urine human chorionic gonadotropin (hCG) test is a safe and non-invasive way to confirm or rule out an ectopic or intrauterine pregnancy.
Serum hCG is used to determine management in cases of unknown pregnancy location and is commonly used as a pregnancy test. Further investigations, such as ultrasound or CT scans of the abdomen and pelvis, may be necessary depending on the results of the pregnancy test.
Possible Causes of Right Iliac Fossa Pain
Right iliac fossa pain can be caused by various conditions, and it is important to differentiate between them to provide appropriate treatment. One of the most common causes is appendicitis, which is characterized by pain radiating to the right iliac fossa, anorexia, and a short history. On the other hand, Crohn’s disease often has a long history, signs of malnutrition, and a change in bowel habit, especially diarrhea. Mesenteric adenitis, which mainly affects children, is caused by viruses and bacteria and is associated with a higher temperature than appendicitis. Diverticulitis, both left and right-sided, may present with right iliac fossa pain, and a CT scan may help in refining the diagnosis.
Other possible causes of right iliac fossa pain include Meckel’s diverticulitis, perforated peptic ulcer, incarcerated right inguinal or femoral hernia, bowel perforation secondary to caecal or colon carcinoma, gynecological causes such as pelvic inflammatory disease and ectopic pregnancy, urological causes such as ureteric colic and testicular torsion, and other conditions like TB, typhoid, herpes zoster, AAA, and situs inversus.
It is important to consider the patient’s clinical history, physical examination, and diagnostic tests to determine the underlying cause of right iliac fossa pain. Prompt diagnosis and treatment can prevent complications and improve outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 54
Incorrect
-
A 23-year-old man is in a car accident and is diagnosed with a pelvic fracture. The nursing staff reports that he is experiencing lower abdominal pain. Upon examination, a distended and tender bladder is found. What is the probable diagnosis?
Your Answer: Prostate rupture
Correct Answer: Urethral injury
Explanation:When a person experiences a pelvic fracture, it can result in a tear in the urethra. The common signs of this injury include difficulty in urinating, blood at the opening of the urethra, and an elevated prostate gland during a rectal examination.
Lower Genitourinary Tract Trauma: Types of Injury and Management
Lower genitourinary tract trauma can occur due to blunt trauma, with most bladder injuries associated with pelvic fractures. However, these injuries can easily be overlooked during trauma assessment. In fact, up to 10% of male pelvic fractures are associated with urethral or bladder injuries.
Urethral injuries are mainly found in males and can be identified by blood at the meatus in 50% of cases. There are two types of urethral injury: bulbar rupture and membranous rupture. Bulbar rupture is the most common and is caused by straddle-type injuries, such as those from bicycles. The triad signs of urinary retention, perineal hematoma, and blood at the meatus are indicative of this type of injury. Membranous rupture, on the other hand, can be extra or intraperitoneal and is commonly due to pelvic fractures. Penile or perineal edema/hematoma and a displaced prostate upwards are also signs of this type of injury. An ascending urethrogram is the recommended investigation, and management involves surgical placement of a suprapubic catheter.
External genitalia injuries, such as those to the penis and scrotum, can be caused by penetration, blunt trauma, continence- or sexual pleasure-enhancing devices, and mutilation.
Bladder injuries can be intra or extraperitoneal and present with haematuria or suprapubic pain. A history of pelvic fracture and inability to void should always raise suspicion of bladder or urethral injury. Inability to retrieve all fluid used to irrigate the bladder through a Foley catheter is also indicative of bladder injury. An IVU or cystogram is the recommended investigation, and management involves laparotomy if intraperitoneal and conservative treatment if extraperitoneal.
In summary, lower genitourinary tract trauma can have various types of injuries, and prompt diagnosis and management are crucial to prevent further complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 55
Incorrect
-
An 80-year-old woman presents with a 3-month history of worsening pain when walking. Upon examination of her right leg, her leg was cold to touch and her medial tibial pulse was difficult to palpate. She also complained of severe calf pain which was also present at rest. The patient underwent intra-arterial thrombolysis for peripheral arterial disease and is now ready to be discharged.
Considering her past medical history of aortic stenosis, blood pressure of 123/72 mmHg, and peptic ulcer disease, what regular medication should be offered to the patient in light of her new diagnosis?Your Answer: Amlodipine
Correct Answer: Atorvastatin and clopidogrel
Explanation:For patients with peripheral arterial disease, it is recommended that they undergo secondary prevention measures. This includes lifestyle modifications such as quitting smoking, improving diet, and exercising regularly. Additionally, all patients with established cardiovascular disease should be prescribed a statin, with the appropriate dose of atorvastatin being 80mg for secondary prevention and 20 mg for primary prevention. Aspirin may be used as an anti-platelet option, but it is not suitable for patients with a history of peptic ulcer disease. In such cases, clopidogrel is recommended as a first-line treatment. The use of phosphodiesterase III inhibitors is currently not advised by NICE. Blood pressure management is also important, with calcium channel blockers being the drug of choice for patients above the age of 55. However, in this patient’s case, amlodipine is not necessary as she does not have a history of high blood pressure and her current blood pressure is normal. GTN may be considered for its vasodilator effects, but it is contraindicated in certain conditions such as aortic stenosis, cardiac tamponade, and hypotensive conditions. Warfarin is not indicated for the secondary prevention of PAD.
Peripheral arterial disease (PAD) is a condition that is strongly associated with smoking. Therefore, patients who still smoke should be provided with assistance to quit smoking. It is also important to treat any comorbidities that the patient may have, such as hypertension, diabetes mellitus, and obesity. All patients with established cardiovascular disease, including PAD, should be taking a statin, with Atorvastatin 80 mg being the recommended dosage. In 2010, NICE published guidance recommending the use of clopidogrel as the first-line treatment for PAD patients instead of aspirin. Exercise training has also been shown to have significant benefits, and NICE recommends a supervised exercise program for all PAD patients before other interventions.
For severe PAD or critical limb ischaemia, there are several treatment options available. Endovascular revascularization and percutaneous transluminal angioplasty with or without stent placement are typically used for short segment stenosis, aortic iliac disease, and high-risk patients. On the other hand, surgical revascularization, surgical bypass with an autologous vein or prosthetic material, and endarterectomy are typically used for long segment lesions, multifocal lesions, lesions of the common femoral artery, and purely infrapopliteal disease. Amputation should only be considered for patients with critical limb ischaemia who are not suitable for other interventions such as angioplasty or bypass surgery.
There are also drugs licensed for use in PAD, including naftidrofuryl oxalate, a vasodilator sometimes used for patients with a poor quality of life. Cilostazol, a phosphodiesterase III inhibitor with both antiplatelet and vasodilator effects, is not recommended by NICE.
-
This question is part of the following fields:
- Surgery
-
-
Question 56
Incorrect
-
A 60-year-old man comes to the Emergency Department complaining of fever and pain in his perineum and scrotum. He has been experiencing dysuria and urinary frequency for the past three days. Upon examination, he appears stable and does not show any signs of sepsis. The digital rectal examination reveals a tender, boggy prostate. The patient is given appropriate treatment and discharged.
A week later, the patient visits his GP. He has been symptom-free for two days but is concerned about his risk of developing prostate cancer, especially since his father had it. He requests a prostate-specific antigen (PSA) test to ensure that he is cancer-free. The patient does not exercise regularly, has not had a digital rectal examination since his hospital visit, and ejaculated 24 hours ago. What should the GP do in this situation?Your Answer: Explain risks and benefits then measure his PSA
Correct Answer: Explain risks and benefits, wait for a month then measure his PSA
Explanation:PSA measurement should be postponed for a month after prostatitis. It is crucial to be aware of the factors that can affect PSA levels, such as vigorous exercise, ejaculation, and digital rectal examination, which can all increase PSA levels. Therefore, measurement should be delayed for at least 48 hours after any of these activities. The clinical description at the beginning indicates acute prostatitis, which elevates PSA levels. As a result, PSA measurement should be postponed for at least a month after prostatitis. It is also important to note that while there is no national screening program for prostate cancer, it is still acceptable and common to measure PSA levels when a patient requests it. However, patients should be informed about the risk of false positives and negatives and the potential consequences before doing so.
Understanding PSA Testing for Prostate Cancer
Prostate specific antigen (PSA) is an enzyme produced by the prostate gland, and it has become an important marker for prostate cancer. However, there is still much debate about its usefulness as a screening tool. The NHS Prostate Cancer Risk Management Programme (PCRMP) has published guidelines on how to handle requests for PSA testing in asymptomatic men. The National Screening Committee has decided not to introduce a prostate cancer screening programme yet, but rather allow men to make an informed choice.
Age-adjusted upper limits for PSA have been recommended by the PCRMP, with levels varying depending on age. PSA levels may also be raised by other factors such as benign prostatic hyperplasia (BPH), prostatitis, urinary tract infection, ejaculation, vigorous exercise, urinary retention, and instrumentation of the urinary tract. However, PSA testing has poor specificity and sensitivity, with around 33% of men with a PSA of 4-10 ng/ml found to have prostate cancer, and around 20% of men with prostate cancer having a normal PSA.
Various methods are used to try and add greater meaning to a PSA level, including age-adjusted upper limits and monitoring changes in PSA level over time. However, the debate continues about the usefulness of PSA testing as a screening tool for prostate cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 57
Incorrect
-
A 28-year-old male patient visits their GP complaining of abdominal pain and bloody diarrhoea that began six weeks ago. He has never experienced anything like this before and believes he may have lost some weight in the past three months. When asked about his family history, he mentions that his father was diagnosed with bowel cancer at the age of 30, and he remembers his grandfather having a stoma before he passed away when the patient was a child. The GP suspects bowel cancer and is concerned about a potential genetic abnormality. During colonoscopy, a large tumour is discovered in the ascending colon near the hepatic flexure, but the rest of the colonic mucosa appears normal. What is the most probable underlying genetic issue?
Your Answer: Li-Fraumeni Syndrome (LFS)
Correct Answer: Lynch Syndrome
Explanation:Familial adenomatous polyposis (FAP) has a mutation in the APC gene and is characterized by over 100 colonic adenomas and a 100% cancer risk. MYH-associated polyposis has a biallelic mutation of the MYH gene and is associated with multiple colonic polyps and a 100% cancer risk by age 60. Peutz-Jeghers syndrome has a mutation in the STK11 gene and is characterized by multiple benign intestinal hamartomas and an increased risk of GI cancers. Cowden disease has a mutation in the PTEN gene and is associated with multiple intestinal hamartomas and an 89% risk of cancer at any site. HNPCC (Lynch syndrome) has germline mutations of DNA mismatch repair genes and is associated with a high risk of colorectal and endometrial cancer. Screening and management strategies vary for each syndrome.
-
This question is part of the following fields:
- Surgery
-
-
Question 58
Incorrect
-
A 52-year-old man is shot in the abdomen and suffers a significant intra-abdominal injury. He undergoes a laparotomy, bowel resection, and end colostomy, and requires a 6-unit blood transfusion due to an associated vascular injury. After a prolonged recovery, he is paralyzed and ventilated for 2 weeks in the intensive care unit. He is given total parenteral nutrition and eventually weaned off the ventilator and transferred to the ward. During a routine blood test, the following results are observed:
Full blood count
Hb 11.3 g/dl
Platelets 267 x 109/l
WBC 10.1 x109/l
Urea and electrolytes
Na+ 131 mmol/l
K+ 4.6 mmol/l
Urea 2.3 mmol/l
Creatinine 78 µmol/l
Liver function tests
Bilirubin 25 µmol/l
ALP 445 u/l
ALT 89 u/l
γGT 103 u/l
What is the most probable underlying cause for the noted abnormalities?Your Answer: Anastomotic leak
Correct Answer: Total parenteral nutrition
Explanation:Liver function tests are often affected by TPN, which can cause cholestasis but it is unlikely to lead to the formation of gallstones as seen in the image. While blood transfusion reactions may cause hepatitis, they usually present earlier and with changes in haemoglobin, which is rare in modern times.
Understanding Total Parenteral Nutrition
Total parenteral nutrition is a commonly used method of providing nutrition to surgical patients who are nutritionally compromised. The bags used in this method contain a combination of glucose, lipids, and essential electrolytes, with the exact composition being determined by the patient’s nutritional requirements. While it is possible to infuse this nutrition peripherally, doing so may result in thrombophlebitis. As such, longer-term infusions should be administered into a central vein, preferably via a PICC line.
Complications associated with total parenteral nutrition are related to sepsis, refeeding syndromes, and hepatic dysfunction. It is important to monitor patients closely for any signs of these complications and adjust the nutrition accordingly. By understanding the basics of total parenteral nutrition, healthcare professionals can provide optimal care to their patients and ensure their nutritional needs are being met.
-
This question is part of the following fields:
- Surgery
-
-
Question 59
Correct
-
As a first-year resident on a surgical rotation, which of the following procedures would necessitate the use of prophylactic antibiotics?
Your Answer: Appendicectomy
Explanation:Preventing Surgical Site Infections
Surgical site infections (SSI) are a common complication following surgery, with up to 20% of all healthcare-associated infections being SSIs. These infections occur when there is a breach in tissue surfaces, allowing normal commensals and other pathogens to initiate infection. In many cases, the organisms causing the infection are derived from the patient’s own body. Measures that may increase the risk of SSI include shaving the wound using a razor, using a non-iodine impregnated incise drape, tissue hypoxia, and delayed administration of prophylactic antibiotics in tourniquet surgery.
To prevent SSIs, there are several steps that can be taken before, during, and after surgery. Before surgery, it is recommended to avoid routine removal of body hair and to use electrical clippers with a single-use head if hair needs to be removed. Antibiotic prophylaxis should be considered for certain types of surgery, such as placement of a prosthesis or valve, clean-contaminated surgery, and contaminated surgery. Local formulary should be used, and a single-dose IV antibiotic should be given on anesthesia. If a tourniquet is to be used, prophylactic antibiotics should be given earlier.
During surgery, the skin should be prepared with alcoholic chlorhexidine, which has been shown to have the lowest incidence of SSI. The surgical site should be covered with a dressing, and wound edge protectors do not appear to confer any benefit. Postoperatively, tissue viability advice should be given for the management of surgical wounds healing by secondary intention. The use of diathermy for skin incisions is not advocated in the NICE guidelines, but several randomized controlled trials have demonstrated no increase in the risk of SSI when diathermy is used.
-
This question is part of the following fields:
- Surgery
-
-
Question 60
Incorrect
-
A 40-year-old male presents to his GP with concerns about his recent difficulty achieving erections, which is causing strain in his relationship. He reports a sudden onset of this issue a few weeks ago, but denies any changes in mood or previous medical or psychiatric conditions. The patient smoked occasionally in his teenage years but has been smoke-free for over 20 years. He maintains a healthy diet and exercises by cycling for an hour each week. Based on this history, what features suggest an organic cause for his erectile dysfunction?
Your Answer: Regular cycling
Correct Answer: Normal libido
Explanation:When it comes to the causes of erectile dysfunction (ED), there are two main factors to consider: organic and psychogenic. If a patient with ED has a normal libido, it is likely that an organic cause is to blame. However, in this particular case, the sudden onset of symptoms makes it difficult to determine whether the cause is organic or psychogenic. While smoking can contribute to ED, the patient’s history of occasional smoking during their teenage years is not significant enough to be a factor. Relationship issues are often linked to psychogenic causes of ED. Additionally, some studies suggest that cycling for more than three hours per week can compress nerves and arteries in the Alcock canal, leading to ED.
Erectile dysfunction (ED) is a condition where a man is unable to achieve or maintain an erection that is sufficient for sexual activity. It is not a disease but a symptom that can be caused by organic, psychogenic, or mixed factors. It is important to differentiate between the causes of ED, with gradual onset of symptoms, lack of tumescence, and normal libido favoring an organic cause, while sudden onset of symptoms, decreased libido, and major life events favoring a psychogenic cause. Risk factors for ED include cardiovascular disease, alcohol use, and certain medications.
To assess for ED, it is recommended to measure lipid and fasting glucose serum levels to calculate cardiovascular risk, as well as free testosterone levels in the morning. If free testosterone is low or borderline, further assessment may be needed. PDE-5 inhibitors, such as sildenafil, are the first-line treatment for ED and should be prescribed to all patients regardless of the cause. Vacuum erection devices can be used as an alternative for those who cannot or will not take PDE-5 inhibitors.
For young men who have always had difficulty achieving an erection, referral to urology is appropriate. Additionally, people with ED who cycle for more than three hours per week should be advised to stop. Overall, ED is a common condition that can be effectively managed with appropriate treatment.
-
This question is part of the following fields:
- Surgery
-
-
Question 61
Correct
-
A 44-year-old man is recovering on the ward several weeks after being treated for acute pancreatitis caused by excessive alcohol consumption. Despite being clinically stable, he continues to experience pain in the epigastric region. Routine blood tests and an abdominal ultrasound scan are performed, revealing the following results:
- Bilirubin: 28 µmol/l
- Albumin: 38 g/l
- ALT: 39 u/l
- γGT: 68 u/l
- CRP: 11.2 mg/l
- Amylase: 541 u/l
The abdominal ultrasound scan shows normal kidney and liver appearances, as well as a normal aortic diameter. However, a cystic lesion measuring 53 mm x 61 mm is present in the head of the pancreas. What is the most appropriate initial management strategy for this patient's pancreatic lesion?Your Answer: Conservative management
Explanation:When a cystic lesion and elevated amylase levels are observed after pancreatitis, it is likely to be a pancreatic pseudocyst. In such cases, it is best to initially manage the condition conservatively, especially if the patient is stable and liver function is not significantly affected. Procedures such as radiological fine-needle aspiration should be avoided as they can increase the risk of infection and have a high morbidity and mortality rate. Active drainage is only necessary if there are signs of infection, mass effect on abdominal organs, or if the pseudocyst persists beyond 12 weeks. Even if the patient experiences symptoms, conservative management is often preferred as the risks of a procedure outweigh the benefits.
Acute pancreatitis can lead to various complications, both locally and systemically. Local complications include peripancreatic fluid collections, which occur in about 25% of cases and may develop into pseudocysts or abscesses. Pseudocysts are walled by fibrous or granulation tissue and typically occur 4 weeks or more after an attack of acute pancreatitis. Pancreatic necrosis, which involves both the pancreatic parenchyma and surrounding fat, can also occur and is directly linked to the extent of necrosis. Pancreatic abscesses may result from infected pseudocysts and can be treated with drainage methods. Haemorrhage may also occur, particularly in cases of infected necrosis.
Systemic complications of acute pancreatitis include acute respiratory distress syndrome, which has a high mortality rate of around 20%. Local complications such as peripancreatic fluid collections and pancreatic necrosis can also lead to systemic complications if left untreated. It is important to manage these complications appropriately, with conservative management being preferred for sterile necrosis and early necrosectomy being avoided unless necessary. Treatment options for local complications include endoscopic or surgical cystogastrostomy, aspiration, and drainage methods. Overall, prompt recognition and management of complications is crucial in improving outcomes for patients with acute pancreatitis.
-
This question is part of the following fields:
- Surgery
-
-
Question 62
Incorrect
-
A 72-year-old man is prescribed tamsulosin for benign prostatic hyperplasia. What are the potential side-effects he may encounter?
Your Answer: Urgency + erectile dysfunction
Correct Answer: Dizziness + postural hypotension
Explanation:Benign prostatic hyperplasia (BPH) is a common condition that affects older men, with around 50% of 50-year-old men showing evidence of BPH and 30% experiencing symptoms. The risk of BPH increases with age, with around 80% of 80-year-old men having evidence of the condition. BPH typically presents with lower urinary tract symptoms (LUTS), which can be categorised into voiding symptoms (obstructive) and storage symptoms (irritative). Complications of BPH can include urinary tract infections, retention, and obstructive uropathy.
Assessment of BPH may involve dipstick urine tests, U&Es, and PSA tests. A urinary frequency-volume chart and the International Prostate Symptom Score (IPSS) can also be used to assess the severity of LUTS and their impact on quality of life. Management options for BPH include watchful waiting, alpha-1 antagonists, 5 alpha-reductase inhibitors, combination therapy, and surgery. Alpha-1 antagonists are considered first-line treatment for moderate-to-severe voiding symptoms, while 5 alpha-reductase inhibitors may be indicated for patients with significantly enlarged prostates and a high risk of progression. Combination therapy and antimuscarinic drugs may also be used in certain cases. Surgery, such as transurethral resection of the prostate (TURP), may be necessary in severe cases.
-
This question is part of the following fields:
- Surgery
-
-
Question 63
Incorrect
-
An elderly man aged 70 visits his GP complaining of intermittent claudication. The vascular team diagnoses him with peripheral arterial disease. What treatment options may be available for him?
Your Answer: Digoxin
Correct Answer: Exercise training
Explanation:Exercise training is a proven beneficial treatment for peripheral arterial disease, while other options such as aspirin, carotid endarterectomy, digoxin, and warfarin are not used. Clopidogrel is now the preferred medication for this condition.
Peripheral arterial disease (PAD) is a condition that is strongly associated with smoking. Therefore, patients who still smoke should be provided with assistance to quit smoking. It is also important to treat any comorbidities that the patient may have, such as hypertension, diabetes mellitus, and obesity. All patients with established cardiovascular disease, including PAD, should be taking a statin, with Atorvastatin 80 mg being the recommended dosage. In 2010, NICE published guidance recommending the use of clopidogrel as the first-line treatment for PAD patients instead of aspirin. Exercise training has also been shown to have significant benefits, and NICE recommends a supervised exercise program for all PAD patients before other interventions.
For severe PAD or critical limb ischaemia, there are several treatment options available. Endovascular revascularization and percutaneous transluminal angioplasty with or without stent placement are typically used for short segment stenosis, aortic iliac disease, and high-risk patients. On the other hand, surgical revascularization, surgical bypass with an autologous vein or prosthetic material, and endarterectomy are typically used for long segment lesions, multifocal lesions, lesions of the common femoral artery, and purely infrapopliteal disease. Amputation should only be considered for patients with critical limb ischaemia who are not suitable for other interventions such as angioplasty or bypass surgery.
There are also drugs licensed for use in PAD, including naftidrofuryl oxalate, a vasodilator sometimes used for patients with a poor quality of life. Cilostazol, a phosphodiesterase III inhibitor with both antiplatelet and vasodilator effects, is not recommended by NICE.
-
This question is part of the following fields:
- Surgery
-
-
Question 64
Incorrect
-
A 7-year-old girl is discovered unresponsive in the bathtub and is rushed to the emergency department in a state of paediatric cardiac arrest. Despite attempts to establish peripheral IV access, the medical team is unable to do so. The decision is made by the registrar to insert an intraosseous line. What is the most frequently used insertion site for this type of line?
Your Answer: Proximal fibula
Correct Answer: Proximal tibia
Explanation:When it is difficult to obtain vascular access in an emergency situation, intraosseous access is often used. This method can be used for both adults and children, with the proximal tibia being the most common site for insertion. In paediatric cases, it is recommended to attempt two peripheral intravenous lines before moving on to intraosseous access. Other potential sites for insertion include the distal femur and humeral head.
Different Routes for Venous Access
There are various methods for establishing venous access, each with its own advantages and disadvantages. The peripheral venous cannula is easy to insert and has a wide lumen for rapid fluid infusions. However, it is unsuitable for administering vasoactive or irritant drugs and may cause infections if not properly managed. On the other hand, central lines have multiple lumens for multiple infusions but are more difficult to insert and require ultrasound guidance. Femoral lines are easier to manage but have high infection rates, while internal jugular lines are preferred. Intraosseous access is typically used in pediatric practice but can also be used in adults for a wide range of fluid infusions. Tunnelled lines, such as Groshong and Hickman lines, are popular for long-term therapeutic requirements and can be linked to injection ports. Finally, peripherally inserted central cannulas (PICC lines) are less prone to major complications and are inserted peripherally.
Overall, the choice of venous access route depends on the patient’s condition, the type of infusion required, and the operator’s expertise. It is important to weigh the benefits and risks of each method and to properly manage any complications that may arise.
-
This question is part of the following fields:
- Surgery
-
-
Question 65
Incorrect
-
A 47-year-old woman is recuperating after a live donor related kidney transplant. She is experiencing considerable abdominal discomfort. What pain-relieving medication should she steer clear of?
Your Answer: Morphine
Correct Answer: Diclofenac
Explanation:Patients who have received renal transplants are typically advised to avoid non-steroidal anti-inflammatory drugs due to their potential nephrotoxicity. The liver is primarily responsible for metabolizing paracetamol and morphine, although there is some renal involvement in the metabolism and excretion of morphine. If the transplanted kidney ceases to function, morphine should be administered in lower doses or avoided altogether.
Organ Transplant: Matching and Rejection
Organ and tissue transplants have become increasingly available, with allografts being the most common type of transplant where an organ is transplanted from one individual to another. However, allografts can elicit an immune response, leading to organ rejection. This is mainly due to allelic differences at genes that code immunohistocompatability complex genes, such as ABO blood group, human leucocyte antigens (HLA), and minor histocompatibility antigens. ABO incompatibility can result in early organ rejection, while HLA mismatching can lead to acute or chronic rejection. An ideal organ match would be one in which all eight alleles are matched.
There are three types of organ rejection: hyperacute, acute, and chronic. Hyperacute rejection occurs immediately due to pre-formed antigens, such as ABO incompatibility. Acute rejection occurs during the first six months and is usually T cell mediated, while chronic rejection occurs after the first six months and is characterized by vascular changes. All types of transplanted organs are susceptible to acute and chronic rejection, with renal transplants being at the greatest risk for hyperacute rejection and liver transplants being at the least risk.
In renal transplantation, patients with end-stage renal failure who are dialysis dependent or likely to become so in the immediate future are considered for transplant. Donor kidneys may be taken from live related donors or brain dead or dying patients. Laparoscopic donor nephrectomy minimizes operative morbidity for the donor, while minimizing warm ischaemic time in the donor phase is crucial. The kidney is prepared on the bench in theatre by the transplant surgeon immediately prior to implantation. The operation is performed under general anaesthesia, with the external iliac artery and vein being anastomosed to the iliacs and the ureter being implanted into the bladder. Acute tubular necrosis is a common problem encountered in cadaveric kidneys, but it tends to resolve. Graft survival times from cadaveric donors are typically of the order of 9 years, while monozygotic twin transplants may survive as long as 25 years.
-
This question is part of the following fields:
- Surgery
-
-
Question 66
Incorrect
-
A fifty eight year old male presents with a four month history of an unresolved varicocoele in his left testis. Initially he was given symptomatic advice. He has now presented with macroscopic haematuria and flank pain. He describes having no energy despite being fit for his age. The testes are palpable. No discharge is elicited from the urethral meatus. His urine dipstick demonstrates blood +++ but is negative for leucocytes. You send him for a cystoscopy as you're concerned he has presented with bladder cancer. The results are returned as normal. What is the most appropriate investigation to perform next in light of his normal cystoscopy?
Your Answer: CA 125
Correct Answer: Renal tract ultrasound
Explanation:Understanding Renal Cell Cancer
Renal cell cancer, also known as hypernephroma, is a primary renal neoplasm that accounts for 85% of cases. It typically arises from the proximal renal tubular epithelium, with the clear cell subtype being the most common. This type of cancer is more prevalent in middle-aged men and is associated with smoking, von Hippel-Lindau syndrome, and tuberous sclerosis. While renal cell cancer is only slightly increased in patients with autosomal dominant polycystic kidney disease, it can present with a classical triad of haematuria, loin pain, and abdominal mass. Other features include pyrexia of unknown origin, endocrine effects, and paraneoplastic hepatic dysfunction syndrome.
The T category criteria for renal cell cancer are based on the size and extent of the tumour. For confined disease, a partial or total nephrectomy may be recommended depending on the tumour size. Patients with a T1 tumour are typically offered a partial nephrectomy, while those with larger tumours may require a total nephrectomy. Treatment options for renal cell cancer include alpha-interferon, interleukin-2, and receptor tyrosine kinase inhibitors such as sorafenib and sunitinib. These medications have been shown to reduce tumour size and treat patients with metastases. It is important to note that renal cell cancer can have paraneoplastic effects, such as Stauffer syndrome, which is associated with cholestasis and hepatosplenomegaly. Overall, early detection and prompt treatment are crucial for improving outcomes in patients with renal cell cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 67
Incorrect
-
A 32-year-old woman is being evaluated on the surgical ward due to complaints of abdominal pain and vomiting. She underwent a gallstone removal procedure earlier in the day. Her vital signs reveal a heart rate of 102 beats/min, blood pressure of 132/92 mmHg, temperature of 38.6ºC, oxygen saturation of 99% in room air, and respiratory rate of 20/min. Blood tests are ordered and a CT scan of the abdomen is requested. What is the probable diagnosis?
Your Answer: Atelectasis
Correct Answer: Pancreatitis
Explanation:The most frequent complication of ERCP is acute pancreatitis, which is indicated by the patient’s symptoms. These may include abdominal pain that spreads to the back, nausea and vomiting, tachycardia caused by pain, and fever. To confirm the diagnosis, a full blood count, lipase, and CT abdomen should be ordered.
Acute pancreatitis is a condition that is mainly caused by gallstones and alcohol in the UK. A popular mnemonic to remember the causes is GET SMASHED, which stands for gallstones, ethanol, trauma, steroids, mumps, autoimmune diseases, scorpion venom, hypertriglyceridaemia, hyperchylomicronaemia, hypercalcaemia, hypothermia, ERCP, and certain drugs. CT scans of patients with acute pancreatitis show diffuse parenchymal enlargement with oedema and indistinct margins. It is important to note that pancreatitis is seven times more common in patients taking mesalazine than sulfasalazine.
-
This question is part of the following fields:
- Surgery
-
-
Question 68
Incorrect
-
Mrs. Smith is a 67-year-old woman who presents with worsening abdominal pain and nausea. She has not had a bowel movement in 5 days.
During examination, her vital signs are as follows: O2 saturation of 97%, respiratory rate of 18, heart rate of 110, and blood pressure of 100/70. She does not have a fever.
Upon palpation of her abdomen, there is significant guarding and she experiences pain when pressure is released. It is suspected that she has peritonism due to bowel obstruction and an urgent abdominal x-ray is ordered.
The x-ray reveals that Mrs. Smith is suffering from large bowel obstruction caused by a sigmoid volvulus. What is the most appropriate course of treatment for her?Your Answer: Insertion of an NG tube and administration of IV fluids
Correct Answer: Urgent laparotomy
Explanation:If a patient with sigmoid volvulus experiences bowel obstruction accompanied by symptoms of peritonitis, it is recommended to forego flexible sigmoidoscopy and opt for urgent midline laparotomy. This is especially important if previous attempts at decompression have failed, if necrotic bowel is observed during endoscopy, or if there is suspicion or confirmation of perforation or peritonitis. Urgent laparotomy is crucial in preventing bowel necrosis or perforation.
Understanding Volvulus: A Condition of Twisted Colon
Volvulus is a medical condition that occurs when the colon twists around its mesenteric axis, leading to a blockage in blood flow and closed loop obstruction. Sigmoid volvulus is the most common type, accounting for around 80% of cases, and is caused by the sigmoid colon twisting on the sigmoid mesocolon. Caecal volvulus, on the other hand, occurs in around 20% of cases and is caused by the caecum twisting. This condition is more common in patients with developmental failure of peritoneal fixation of the proximal bowel.
Sigmoid volvulus is often associated with chronic constipation, Chagas disease, neurological conditions like Parkinson’s disease and Duchenne muscular dystrophy, and psychiatric conditions like schizophrenia. Caecal volvulus, on the other hand, is associated with adhesions, pregnancy, and other factors. Symptoms of volvulus include constipation, abdominal bloating, abdominal pain, and nausea/vomiting.
Diagnosis of volvulus is usually done through an abdominal film, which shows signs of large bowel obstruction alongside the coffee bean sign for sigmoid volvulus. Small bowel obstruction may be seen in caecal volvulus. Management of sigmoid volvulus involves rigid sigmoidoscopy with rectal tube insertion, while caecal volvulus usually requires operative management, with right hemicolectomy often being necessary.
-
This question is part of the following fields:
- Surgery
-
-
Question 69
Incorrect
-
A 25-year-old man sustains 25% partial and full thickness burns in a residential fire, along with an inhalational injury. The medical team decides to provide intravenous fluids to replace lost fluids. What is the recommended intravenous fluid for initial resuscitation?
Your Answer: Fresh frozen plasma
Correct Answer: Hartmann's solution
Explanation:Typically, Hartmann’s (Ringers lactate) is the initial crystalloid administered in most units. However, there is still debate as some units prefer colloid. If colloid leaks into the interstitial tissues, it could potentially heighten the risk of edema.
Fluid Resuscitation for Burns
Fluid resuscitation is necessary for patients with burns that cover more than 15% of their total body area (10% for children). The primary goal of resuscitation is to prevent the burn from deepening. Most fluid is lost within the first 24 hours after injury, and during the first 8-12 hours, fluid shifts from the intravascular to the interstitial fluid compartments, which can compromise circulatory volume. However, fluid resuscitation causes more fluid to enter the interstitial compartment, especially colloid, which should be avoided in the first 8-24 hours. Protein loss also occurs.
The Parkland formula is used to calculate the total fluid requirement in 24 hours, which is given as 4 ml x (total burn surface area (%)) x (body weight (kg)). Fifty percent of the total fluid requirement is given in the first 8 hours, and the remaining 50% is given in the next 16 hours. The resuscitation endpoint is a urine output of 0.5-1.0 ml/kg/hour in adults, and the rate of fluid is increased to achieve this.
It is important to note that the starting point of resuscitation is the time of injury, and fluids already given should be deducted. After 24 hours, colloid infusion is begun at a rate of 0.5 ml x (total burn surface area (%)) x (body weight (kg)), and maintenance crystalloid (usually dextrose-saline) is continued at a rate of 1.5 ml x (burn area) x (body weight). Colloids used include albumin and FFP, and antioxidants such as vitamin C can be used to minimize oxidant-mediated contributions to the inflammatory cascade in burns. High tension electrical injuries and inhalation injuries require more fluid, and monitoring of packed cell volume, plasma sodium, base excess, and lactate is essential.
-
This question is part of the following fields:
- Surgery
-
-
Question 70
Incorrect
-
A patient is brought into resus following a seizure, she has a nasopharyngeal airway (NPA) in situ. A nasopharyngeal airway would be contraindicated in?
Your Answer: A patient with an obstructed airway
Correct Answer: Base of skull fractures
Explanation:Nasopharyngeal Airway for Maintaining Airway Patency
Nasopharyngeal airways are medical devices used to maintain a patent airway in patients with decreased Glasgow coma score (GCS). These airways are inserted into the nostril after being lubricated, and they come in various sizes. They are particularly useful for patients who are having seizures, as an oropharyngeal airway (OPA) may not be suitable for insertion.
Nasopharyngeal airways are generally well-tolerated by patients with low GCS. However, they should be used with caution in patients with base of skull fractures, as they may cause further damage. It is important to note that these airways should only be inserted by trained medical professionals to avoid any complications. Overall, nasopharyngeal airways are an effective tool for maintaining airway patency in patients with decreased GCS.
-
This question is part of the following fields:
- Surgery
-
-
Question 71
Incorrect
-
A 58-year-old male presents to the emergency department with a sudden and severe occipital headache accompanied by two episodes of vomiting within the last hour. Despite a normal CT scan, a lumbar puncture taken 12 hours later reveals xanthochromia, leading to a diagnosis of subarachnoid hemorrhage (SAH). Urgent neurosurgical consultation is requested, and a CT cerebral angiography confirms a posterior communicating artery aneurysm as the underlying cause of the SAH. The patient is otherwise healthy. What is the most suitable treatment option for the aneurysm?
Your Answer: Surgical clipping
Correct Answer: Coiling by an interventional neuroradiologist
Explanation:After a subarachnoid haemorrhage, urgent intervention is necessary for intracranial aneurysms due to the risk of rebleeding. The most common treatment for this is coiling by an interventional neuroradiologist, which involves inserting soft metallic coils into the aneurysm to exclude it from intracranial circulation. This is less invasive than surgical clipping. While nimodipine is used to reduce vasospasm following a SAH, it is not sufficient on its own and additional intervention is required. Typically, nimodipine is administered for 21 days and targets the brain vasculature by inhibiting calcium channels.
A subarachnoid haemorrhage (SAH) is a type of bleeding that occurs within the subarachnoid space of the meninges in the brain. It can be caused by head injury or occur spontaneously. Spontaneous SAH is often caused by an intracranial aneurysm, which accounts for around 85% of cases. Other causes include arteriovenous malformation, pituitary apoplexy, and mycotic aneurysms. The classic symptoms of SAH include a sudden and severe headache, nausea and vomiting, meningism, coma, seizures, and ECG changes.
The first-line investigation for SAH is a non-contrast CT head, which can detect acute blood in the basal cisterns, sulci, and ventricular system. If the CT is normal within 6 hours of symptom onset, a lumbar puncture is not recommended. However, if the CT is normal after 6 hours, a lumbar puncture should be performed at least 12 hours after symptom onset to check for xanthochromia and other CSF findings consistent with SAH. If SAH is confirmed, referral to neurosurgery is necessary to identify the underlying cause and provide urgent treatment.
Management of aneurysmal SAH involves supportive care, such as bed rest, analgesia, and venous thromboembolism prophylaxis. Vasospasm is prevented with oral nimodipine, and intracranial aneurysms require prompt intervention to prevent rebleeding. Most aneurysms are treated with a coil by interventional neuroradiologists, but some require a craniotomy and clipping by a neurosurgeon. Complications of aneurysmal SAH include re-bleeding, hydrocephalus, vasospasm, and hyponatraemia. Predictive factors for SAH include conscious level on admission, age, and amount of blood visible on CT head.
-
This question is part of the following fields:
- Surgery
-
-
Question 72
Incorrect
-
A 60-year-old man visits his doctor with worries about blood in his stool. He has been noticing red blood for a few weeks now. Recently, he experienced pain while passing stools and felt a lump around his anus. During the examination, a purple mass is observed in the perianal area. Upon direct rectal examination, a tender lump is confirmed at the 7 o'clock position. What is the best course of action for managing this presentation?
Your Answer: Referral to gastroenterology for suspected perianal Crohn's disease
Correct Answer: Advise analgesia and stool softeners, suggest ice packs around the area
Explanation:The symptoms described strongly suggest thrombosed haemorrhoids, as the patient experiences pain during bowel movements and has a tender lump near the anus, along with rectal bleeding. Normally, haemorrhoids do not cause pain unless they are thrombosed.
If the patient seeks medical attention within 72 hours of the onset of pain, NICE recommends hospital admission for surgical treatment of the haemorrhoids to provide immediate relief from pain.
After the first 72 hours, the thrombus is likely to contract and resolve on its own within a few weeks. In such cases, conservative management options such as pain relief medication, stool softeners, and ice packs are more appropriate.
It is unlikely that the patient has perianal Crohn’s disease if they have no history of inflammatory bowel disease.
Perianal abscesses cause severe pain in the perianal area, but unlike thrombosed haemorrhoids, this pain is not necessarily associated with bowel movements. A visible lump may or may not be present, and there may be pus discharge if the abscess has ruptured, but blood is not typically seen.
While it is important to rule out more serious causes of rectal bleeding, referring the patient under a 2-week-wait rule would not address their current symptoms. It is more appropriate to investigate the underlying cause once the acute presentation has resolved.Thrombosed haemorrhoids are characterized by severe pain and the presence of a tender lump. Upon examination, a purplish, swollen, and tender subcutaneous perianal mass can be observed. If the patient seeks medical attention within 72 hours of onset, referral for excision may be necessary. However, if the condition has progressed beyond this timeframe, patients can typically manage their symptoms with stool softeners, ice packs, and pain relief medication. Symptoms usually subside within 10 days.
-
This question is part of the following fields:
- Surgery
-
-
Question 73
Incorrect
-
You are shadowing a registrar on the pediatric ward, who is asked to help their consultant confirm a suspected case of brain stem death.
Which of the following would the doctors be assessing for?Your Answer: Babinski reflex
Correct Answer: Corneal reflex
Explanation:To confirm brain death, there are six tests that need to be conducted. These tests include the pupillary reflex, corneal reflex, oculovestibular reflex, cough reflex, absent response to supraorbital pressure, and no spontaneous respiratory effort. Out of these tests, the corneal reflex is the only one that is specifically tested for in suspected brain stem death. The Babinski reflex is used to test for upper motor neuron damage, while the Moro reflex is a primitive reflex that is only tested for in neonates. Lastly, the ankle jerk reflex is a deep tendon reflex that tests cutaneous innervation, motor supply, and cortical input at the S1 level.
Criteria and Testing for Brain Stem Death
Brain death occurs when the brain and brain stem cease to function, resulting in irreversible loss of consciousness and vital functions. To determine brain stem death, certain criteria must be met and specific tests must be performed. The patient must be in a deep coma of known cause, with reversible causes excluded and no sedation. Electrolyte levels must be normal.
The testing for brain stem death involves several assessments. The pupils must be fixed and unresponsive to changes in light intensity. The corneal reflex must be absent, and there should be no response to supraorbital pressure. The oculovestibular reflexes must be absent, which is tested by injecting ice-cold water into each ear. There should be no cough reflex to bronchial stimulation or gagging response to pharyngeal stimulation. Finally, there should be no observed respiratory effort in response to disconnection from the ventilator for at least five minutes, with adequate oxygenation ensured.
It is important that the testing is performed by two experienced doctors on two separate occasions, with at least one being a consultant. Neither doctor can be a member of the transplant team if organ donation is being considered. These criteria and tests are crucial in determining brain stem death and ensuring that the patient is beyond recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 74
Incorrect
-
A 67-year-old presents with acute abdominal pain and is found to have a perforated sigmoid colon due to colonic cancer. He is peritonitic on examination and requires an emergency Hartmann's procedure. What is a true statement regarding his condition?
Your Answer: He will most likely require a stoma on the right side of his abdomen
Correct Answer: He requires an end colostomy
Explanation:In cases of perforation of the rectosigmoid bowel leading to peritonitis, an emergency Hartmann’s procedure may be necessary. This involves removing the affected portion of the colon, creating an end colostomy, and sewing the rectal stump. The perforation may be caused by conditions such as colon cancer, diverticulitis, or trauma. The colostomy is typically placed on the left side of the abdomen and sewn flush with the skin.
Colorectal cancer is typically diagnosed through CT scans and colonoscopies or CT colonography. Patients with tumors below the peritoneal reflection should also undergo MRI to evaluate their mesorectum. Once staging is complete, a treatment plan is formulated by a dedicated colorectal MDT meeting.
For colon cancer, surgery is the primary treatment option, with resectional surgery being the only cure. The procedure is tailored to the patient and tumor location, with lymphatic chains being resected based on arterial supply. Anastomosis is the preferred method of restoring continuity, but in some cases, an end stoma may be necessary. Chemotherapy is often offered to patients with risk factors for disease recurrence.
Rectal cancer management differs from colon cancer due to the rectum’s anatomical location. Tumors can be surgically resected with either an anterior resection or an abdominoperineal excision of rectum (APER). A meticulous dissection of the mesorectal fat and lymph nodes is integral to the procedure. Neoadjuvant radiotherapy is often offered to patients prior to resectional surgery, and those with obstructing rectal cancer should have a defunctioning loop colostomy.
Segmental resections based on blood supply and lymphatic drainage are the primary operations for cancer. The type of resection and anastomosis depend on the site of cancer. In emergency situations where the bowel has perforated, an end colostomy is often safer. Left-sided resections are more risky, but ileocolic anastomoses are relatively safe even in the emergency setting and do not need to be defunctioned.
-
This question is part of the following fields:
- Surgery
-
-
Question 75
Incorrect
-
A 68-year-old woman undergoes a lumpectomy for a T2 hormone receptor-positive carcinoma in her right breast. The pathology report shows cancerous cells at the margins of the resected specimen. Should the patient receive any additional non-surgical treatment?
Your Answer: Ipsilateral chest wall and regional lymph node radiotherapy + course of letrozole
Correct Answer: Ipsilateral chest wall and regional lymph node radiotherapy
Explanation:Adjuvant ipsilateral chest wall and regional lymph node radiotherapy are recommended for patients with positive axillary lymph nodes and residual tumor at resection margins post-mastectomy, as studies have shown a beneficial effect on overall survival and locoregional recurrence. However, adding letrozole or trastuzumab is not appropriate for this patient with triple-negative carcinoma, as these treatments are used for ER+ and HER2+ cancers, respectively. It is also not necessary to irradiate both breasts/axillae in cases of unilateral breast cancer. No adjuvant treatment is not appropriate in this case, as there is residual disease that needs to be managed. These recommendations are based on the Nice guideline NG101 (2018).
Breast cancer management varies depending on the stage of the cancer, type of tumor, and patient’s medical history. Treatment options may include surgery, radiotherapy, hormone therapy, biological therapy, and chemotherapy. Surgery is typically the first option for most patients, except for elderly patients with metastatic disease who may benefit more from hormonal therapy. Prior to surgery, an axillary ultrasound is recommended for patients without palpable axillary lymphadenopathy, while those with clinically palpable lymphadenopathy require axillary node clearance. The type of surgery offered depends on various factors, such as tumor size, location, and type. Breast reconstruction is also an option for patients who have undergone a mastectomy.
Radiotherapy is recommended after a wide-local excision to reduce the risk of recurrence, while mastectomy patients may receive radiotherapy for T3-T4 tumors or those with four or more positive axillary nodes. Hormonal therapy is offered if tumors are positive for hormone receptors, with tamoxifen being used in pre- and perimenopausal women and aromatase inhibitors like anastrozole in postmenopausal women. Tamoxifen may increase the risk of endometrial cancer, venous thromboembolism, and menopausal symptoms. Biological therapy, such as trastuzumab, is used for HER2-positive tumors but cannot be used in patients with a history of heart disorders. Chemotherapy may be used before or after surgery, depending on the stage of the tumor and the presence of axillary node disease. FEC-D is commonly used in the latter case.
-
This question is part of the following fields:
- Surgery
-
-
Question 76
Incorrect
-
A 24-hour-old full-term neonate is attempting to feed from her mother, but is unable to keep anything down. The vomit appears green, indicating possible bile staining. The delivery was uncomplicated and vaginal. The neonate appears healthy and stable otherwise. What is the probable diagnosis?
Your Answer: Necrotising enterocolitis
Correct Answer: Intestinal atresia
Explanation:Bilious vomiting occurring on the first day of life is most likely caused by intestinal atresia, specifically duodenal atresia or ileal/jejunal atresia. To confirm the diagnosis, an ultrasound is necessary. Malrotation is not the most likely cause as it typically presents with haemodynamic instability on the third day of life. Meconium ileus is also unlikely as it usually presents with abdominal distention within the first 48 hours. A milk allergy is not a probable cause as it does not typically result in bilious vomiting.
Causes and Treatments for Bilious Vomiting in Neonates
Bilious vomiting in neonates can be caused by various disorders, including duodenal atresia, malrotation with volvulus, jejunal/ileal atresia, meconium ileus, and necrotising enterocolitis. Duodenal atresia occurs in 1 in 5000 births and is more common in babies with Down syndrome. It typically presents a few hours after birth and can be diagnosed through an abdominal X-ray that shows a double bubble sign. Treatment involves duodenoduodenostomy. Malrotation with volvulus is usually caused by incomplete rotation during embryogenesis and presents between 3-7 days after birth. An upper GI contrast study or ultrasound can confirm the diagnosis, and treatment involves Ladd’s procedure. Jejunal/ileal atresia is caused by vascular insufficiency in utero and occurs in 1 in 3000 births. It presents within 24 hours of birth and can be diagnosed through an abdominal X-ray that shows air-fluid levels. Treatment involves laparotomy with primary resection and anastomosis. Meconium ileus occurs in 15-20% of babies with cystic fibrosis and presents in the first 24-48 hours of life with abdominal distension and bilious vomiting. Diagnosis involves an abdominal X-ray that shows air-fluid levels, and a sweat test can confirm cystic fibrosis. Treatment involves surgical decompression, and segmental resection may be necessary for serosal damage. Necrotising enterocolitis occurs in up to 2.4 per 1000 births, with increased risks in prematurity and inter-current illness. It typically presents in the second week of life and can be diagnosed through an abdominal X-ray that shows dilated bowel loops, pneumatosis, and portal venous air. Treatment involves conservative and supportive measures for non-perforated cases, while laparotomy and resection are necessary for perforated cases or ongoing clinical deterioration.
-
This question is part of the following fields:
- Surgery
-
-
Question 77
Incorrect
-
A 32-year-old woman with long-standing varicose veins presents to the hospital with a burning pain over one of the veins, accompanied by tenderness and redness in the surrounding skin. On examination, a worm-like mass is felt, and the tissue appears erythematosus and hard. There is no evidence of deep vein thrombosis, and observations are normal. An ankle-brachial pressure index of 1.0 is recorded, and a Doppler reveals a lack of compressibility and an intraluminal thrombus in the superficial vein. What is the recommended treatment for this condition?
Your Answer: Intravenous antibiotics
Correct Answer: Compression stockings
Explanation:Compression stockings are the recommended treatment for superficial thrombophlebitis. This is because they are effective in managing symptoms and aiding in the resolution of the condition. The patient’s history of varicose veins, along with examination and investigation results, strongly support the diagnosis of superficial thrombophlebitis. The ankle-brachial pressure index was checked to ensure that the arterial supply is sufficient, as compression stockings may compromise this. In addition to compression stockings, a low-molecular-weight heparin or fondaparinux may also be used. Intravenous antibiotics are not necessary in this case, as there is no evidence of severe infection. Rivaroxaban and warfarin are not typically used in the management of superficial thrombophlebitis, as there is no evidence of deep vein thrombosis. While some vascular surgeons may prescribe topical heparinoid, there is little evidence supporting its use in treating this condition, and it is not part of the main guidelines for management.
Superficial thrombophlebitis is inflammation associated with thrombosis of a superficial vein, usually the long saphenous vein of the leg. Around 20% of cases have an underlying deep vein thrombosis (DVT) and 3-4% may progress to a DVT if untreated. Treatment options include NSAIDs, topical heparinoids, compression stockings, and low-molecular weight heparin. Patients with clinical signs of superficial thrombophlebitis affecting the proximal long saphenous vein should have an ultrasound scan to exclude concurrent DVT. Patients with superficial thrombophlebitis at, or extending towards, the saphenofemoral junction can be considered for therapeutic anticoagulation for 6-12 weeks.
-
This question is part of the following fields:
- Surgery
-
-
Question 78
Incorrect
-
Which one of the following is not a reason for circumcision in infants?
Your Answer: Phimosis
Correct Answer: Peyronie's disease
Explanation:Understanding Circumcision
Circumcision is a practice that has been carried out in various cultures for centuries. Today, it is mainly practiced by people of the Jewish and Islamic faith for religious or cultural reasons. However, it is important to note that circumcision for these reasons is not available on the NHS.
The medical benefits of circumcision are still a topic of debate. However, some studies have shown that it can reduce the risk of penile cancer, urinary tract infections, and sexually transmitted infections, including HIV.
There are also medical indications for circumcision, such as phimosis, recurrent balanitis, balanitis xerotica obliterans, and paraphimosis. It is crucial to rule out hypospadias before performing circumcision as the foreskin may be needed for surgical repair.
Circumcision can be performed under local or general anesthesia. It is a personal decision that should be made after careful consideration of the potential benefits and risks.
-
This question is part of the following fields:
- Surgery
-
-
Question 79
Incorrect
-
A 72-year-old type 2 diabetic is scheduled for a vaginal hysterectomy tomorrow. Her usual medication regimen includes taking Metformin in the morning and Gliclazide during breakfast and dinner. What is the recommended approach for managing her medications prior to surgery?
Your Answer: Omit Metformin on the day of surgery. Halve the Gliclazide doses at lunchtime and dinner.
Correct Answer: Omit Metformin on the day of surgery. Omit the morning Gliclazide, and take the dinner time Gliclazide if she is able to eat.
Explanation:Medication Management for Diabetic Patients on the Day of Surgery
When managing medication for diabetic patients on the day of surgery, it is important to consider the potential risks and benefits of each medication. Here are some guidelines for different scenarios:
– Omit Metformin on the day of surgery. Omit the morning Gliclazide, and take the dinner time Gliclazide if she is able to eat.
– Omit Metformin the day before and on the day. Take Gliclazide as normal.
– Take Metformin as normal. Omit Gliclazide.
– Omit Metformin the day before and on the day. Omit Gliclazide on the day of surgery.
– Omit Metformin on the day of surgery. Halve the Gliclazide doses at lunchtime and dinner.It is important to note that these guidelines may vary depending on the individual patient’s medical history and current condition. It is recommended to consult with a healthcare professional for personalized medication management.
-
This question is part of the following fields:
- Surgery
-
-
Question 80
Incorrect
-
You are on duty in the neurosurgical unit overnight. A patient in his sixties was admitted with an intracerebral hemorrhage, which was found to have extended into the ventricles on CT scan. The patient has been stable throughout the day, but a nurse contacts you to report a decrease in the patient's Glasgow Coma Scale score. While previously 15, the patient is now only able to localize to pain. What is the probable cause of this change in symptoms?
Your Answer: Expansion of the haematoma
Correct Answer: Hydrocephalus
Explanation:Intraventricular haemorrhages often lead to hydrocephalus, which is a frequent complication. Treatment typically involves the use of an external ventricular drain. While the expansion of the haematoma can cause midline shift, it is not as common as hydrocephalus. Reduced responsiveness is not a symptom of hyponatraemia, which can occur with various cerebral injuries. Vasospasm is only observed in patients with subarachnoid haemorrhages.
Understanding Hydrocephalus
Hydrocephalus is a medical condition characterized by an excessive amount of cerebrospinal fluid (CSF) in the ventricular system of the brain. This is caused by an imbalance between the production and absorption of CSF. Patients with hydrocephalus experience symptoms due to increased intracranial pressure, such as headaches, nausea, vomiting, and papilloedema. In severe cases, it can lead to coma. Infants with hydrocephalus have an increase in head circumference, and their anterior fontanelle bulges and becomes tense. Failure of upward gaze is also common in children with severe hydrocephalus.
Hydrocephalus can be classified into two categories: obstructive and non-obstructive. Obstructive hydrocephalus is caused by a structural pathology that blocks the flow of CSF, while non-obstructive hydrocephalus is due to an imbalance of CSF production and absorption. Normal pressure hydrocephalus is a unique form of non-obstructive hydrocephalus characterized by large ventricles but normal intracranial pressure. The classic triad of symptoms is dementia, incontinence, and disturbed gait.
To diagnose hydrocephalus, a CT head is used as a first-line imaging investigation. MRI may be used to investigate hydrocephalus in more detail, particularly if there is a suspected underlying lesion. Lumbar puncture is both diagnostic and therapeutic since it allows you to sample CSF, measure the opening pressure, and drain CSF to reduce the pressure. Treatment for hydrocephalus involves an external ventricular drain (EVD) in acute, severe cases, and a ventriculoperitoneal shunt (VPS) for long-term CSF diversion. In obstructive hydrocephalus, the treatment may involve surgically treating the obstructing pathology. It is important to note that lumbar puncture must not be used in obstructive hydrocephalus since it can cause brain herniation.
-
This question is part of the following fields:
- Surgery
-
-
Question 81
Incorrect
-
A 35-year-old male presents to your GP evening clinic with complaints of abdominal pain. He reports experiencing pain in the lower left abdomen which has worsened throughout the day. He also feels feverish, nauseous, and has vomited twice in the past hour. He cannot recall the last time he passed urine or stool and mentions having a small painless lump on his lower left abdomen for the past month which he has not sought medical attention for.
Upon examination, the patient appears unwell and clammy. He is tachycardic and normotensive. His abdomen is mildly distended and very tender to touch, with evidence of localised tenderness in the left iliac fossa. Additionally, you notice a 2 cm x 2 cm erythematosus lump in the left inguinal area which is now extremely painful to touch.
What is the most appropriate next step?Your Answer: Ask the patient to provide you with a urine sample
Correct Answer: Call 999 and arrange an urgent assessment of your patient in hospital
Explanation:It is not recommended to manually reduce strangulated inguinal hernias while awaiting surgery. In the scenario of a patient with an acute abdomen and signs of a strangulated hernia, the appropriate response is to call 999 for urgent assessment and inform the surgical registrar on-call. Attempting to manually reduce the hernia can worsen the patient’s condition. Requesting a urine sample or discussing an appendicectomy is not appropriate in this situation.
Understanding Strangulated Inguinal Hernias
An inguinal hernia occurs when abdominal contents protrude through the superficial inguinal ring. This can happen directly through the deep inguinal ring or indirectly through the posterior wall of the inguinal canal. Hernias should be reducible, meaning that the herniated tissue can be pushed back into place in the abdomen through the defect using a hand. However, if a hernia cannot be reduced, it is referred to as an incarcerated hernia, which is at risk of strangulation. Strangulation is a surgical emergency where the blood supply to the herniated tissue is compromised, leading to ischemia or necrosis.
Symptoms of a strangulated hernia include pain, fever, an increase in the size of a hernia or erythema of the overlying skin, peritonitic features such as guarding and localised tenderness, bowel obstruction, and bowel ischemia. Imaging can be used in cases of suspected strangulation, but it is not considered necessary and is more useful in excluding other pathologies. Repair involves immediate surgery, either from an open or laparoscopic approach with a mesh technique. This is the same technique used in elective hernia repair, however, any dead bowel will also have to be removed. While waiting for the surgery, it is not recommended that you manually reduce strangulated hernias, as this can cause more generalised peritonitis. Strangulation occurs in around 1 in 500 cases of all inguinal hernias, and indications that a hernia is at risk of strangulation include episodes of pain in a hernia that was previously asymptomatic and irreducible hernias.
-
This question is part of the following fields:
- Surgery
-
-
Question 82
Incorrect
-
A 45-year-old female presents to the Emergency Department with right upper quadrant pain, nausea and vomiting. Her temperature is 38.2ºC and she was described as having rigors in the ambulance. She scores 14 on the Glasgow coma scale (GCS) as she is confused when asked questions.
What is the likely diagnosis based on her symptoms, which include yellowing of the sclera, tenderness in the right upper quadrant of her abdomen with a positive Murphy's sign, and vital signs of a respiratory rate of 15/min, heart rate of 92/min, and blood pressure of 86/62 mmHg?Your Answer: Beck's triad
Correct Answer: Reynold's pentad
Explanation:The patient is suspected to have ascending cholangitis and exhibits Charcot’s triad of RUQ pain, fever, and jaundice. In severe cases, Reynold’s pentad may be present, which includes Charcot’s triad along with confusion and hypotension, indicating a higher risk of mortality. Beck’s triad, consisting of hypotension, raised JVP, and muffled heart sounds, is observed in patients with cardiac tamponade. Cushing’s triad, characterized by irregular and decreased respiratory rate, bradycardia, and hypertension, is seen in patients with elevated intracranial pressure.
Understanding Ascending Cholangitis
Ascending cholangitis is a bacterial infection that affects the biliary tree, with E. coli being the most common culprit. This condition is often associated with gallstones, which can predispose individuals to the infection. Patients with ascending cholangitis may present with Charcot’s triad, which includes fever, right upper quadrant pain, and jaundice. However, this triad is only present in 20-50% of cases. Other common symptoms include hypotension and confusion. In severe cases, Reynolds’ pentad may be observed, which includes the additional symptoms of hypotension and confusion.
To diagnose ascending cholangitis, ultrasound is typically used as a first-line investigation to look for bile duct dilation and stones. Raised inflammatory markers may also be observed. Treatment involves intravenous antibiotics and endoscopic retrograde cholangiopancreatography (ERCP) after 24-48 hours to relieve any obstruction.
Overall, ascending cholangitis is a serious condition that requires prompt diagnosis and treatment. Understanding the symptoms and risk factors associated with this condition can help individuals seek medical attention early and improve their chances of a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 83
Incorrect
-
This 30-year-old man underwent a laparotomy for a perforated duodenal ulcer 3 years ago. The scar that resulted is depicted in the image. What is the most commonly acknowledged factor in the formation of this anomaly?
Your Answer: Family history
Correct Answer: Race
Explanation:Understanding Keloid Scars: Causes and Risk Factors
Keloid scars are a type of abnormal scar tissue that grows beyond the original margins of a wound and does not regress. They are more common in individuals with highly pigmented skin, with a frequency 15 times higher than in those with less pigmented skin. Keloids tend to occur in individuals aged 10-30 years and are more likely to form in areas such as the upper chest, shoulders, sternum, and earlobes. Wounds that are under tension while healing or get infected, burns, and acne scars are also more likely to result in keloid formation. While there is some evidence of a genetic predisposition to keloid formation, race is a stronger risk factor. Keloids affect both sexes equally, but young women may be more susceptible due to the higher frequency of earlobe piercing.
-
This question is part of the following fields:
- Surgery
-
-
Question 84
Incorrect
-
A 67-year-old man presents to his oncology appointment with a recent diagnosis of renal cell carcinoma. He was referred to the haematuria clinic where an abnormal mass was discovered on his abdominal x-ray. Further staging investigations revealed a 9cm tumour on the left kidney that had invaded the renal capsule but was confined to Gerota's fascia. No evidence of metastatic disease was found. What is the optimal course of action for this patient?
Your Answer: Receptor tyrosine kinase inhibitors
Correct Answer: Radical nephrectomy
Explanation:Understanding Renal Cell Cancer
Renal cell cancer, also known as hypernephroma, is a primary renal neoplasm that accounts for 85% of cases. It typically arises from the proximal renal tubular epithelium, with the clear cell subtype being the most common. This type of cancer is more prevalent in middle-aged men and is associated with smoking, von Hippel-Lindau syndrome, and tuberous sclerosis. While renal cell cancer is only slightly increased in patients with autosomal dominant polycystic kidney disease, it can present with a classical triad of haematuria, loin pain, and abdominal mass. Other features include pyrexia of unknown origin, endocrine effects, and paraneoplastic hepatic dysfunction syndrome.
The T category criteria for renal cell cancer are based on the size and extent of the tumour. For confined disease, a partial or total nephrectomy may be recommended depending on the tumour size. Patients with a T1 tumour are typically offered a partial nephrectomy, while those with larger tumours may require a total nephrectomy. Treatment options for renal cell cancer include alpha-interferon, interleukin-2, and receptor tyrosine kinase inhibitors such as sorafenib and sunitinib. These medications have been shown to reduce tumour size and treat patients with metastases. It is important to note that renal cell cancer can have paraneoplastic effects, such as Stauffer syndrome, which is associated with cholestasis and hepatosplenomegaly. Overall, early detection and prompt treatment are crucial for improving outcomes in patients with renal cell cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 85
Incorrect
-
A 68-year-old woman has been diagnosed with breast cancer and is now taking anastrozole to prevent recurrence after a mastectomy. She has a medical history of hypothyroidism and depression, which are managed with levothyroxine and fluoxetine. What is the most probable complication she may encounter during her breast cancer treatment?
Your Answer: Increased likelihood of cancer recurrence due to drug interaction
Correct Answer: Osteoporotic fracture
Explanation:Osteoporosis may be a potential side effect of aromatase inhibitors such as anastrozole.
Anti-oestrogen drugs are used in the management of oestrogen receptor-positive breast cancer. Selective oEstrogen Receptor Modulators (SERM) such as Tamoxifen act as an oestrogen receptor antagonist and partial agonist. However, Tamoxifen can cause adverse effects such as menstrual disturbance, hot flashes, venous thromboembolism, and endometrial cancer. On the other hand, aromatase inhibitors like Anastrozole and Letrozole reduce peripheral oestrogen synthesis, which is important in postmenopausal women. Anastrozole is used for ER +ve breast cancer in this group. However, aromatase inhibitors can cause adverse effects such as osteoporosis, hot flashes, arthralgia, myalgia, and insomnia. NICE recommends a DEXA scan when initiating a patient on aromatase inhibitors for breast cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 86
Incorrect
-
A 72-year-old man visits his GP complaining of voiding symptoms but no storage symptoms. After being diagnosed with benign prostatic hyperplasia, conservative management proves ineffective. The recommended first-line medication also fails to alleviate his symptoms. Further examination reveals an estimated prostate size of over 30g and a prostate-specific antigen level of 2.2 ng/ml. What medication is the GP likely to prescribe for this patient?
Your Answer: Terazosin
Correct Answer: Finasteride
Explanation:If a patient with BPH has a significantly enlarged prostate, 5 alpha-reductase inhibitors should be considered as a second-line treatment option. Finasteride is an example of a 5 alpha-reductase inhibitor and is used when alpha-1-antagonists fail to manage symptoms. Desmopressin is a later stage drug used for BPH with nocturnal polyuria after other treatments have failed. Tamsulosin is an alpha-1-antagonist and is the first-line option for BPH. Terazosin is another alpha-blocker and could also be used as a first-line option.
Benign prostatic hyperplasia (BPH) is a common condition that affects older men, with around 50% of 50-year-old men showing evidence of BPH and 30% experiencing symptoms. The risk of BPH increases with age, with around 80% of 80-year-old men having evidence of the condition. BPH typically presents with lower urinary tract symptoms (LUTS), which can be categorised into voiding symptoms (obstructive) and storage symptoms (irritative). Complications of BPH can include urinary tract infections, retention, and obstructive uropathy.
Assessment of BPH may involve dipstick urine tests, U&Es, and PSA tests. A urinary frequency-volume chart and the International Prostate Symptom Score (IPSS) can also be used to assess the severity of LUTS and their impact on quality of life. Management options for BPH include watchful waiting, alpha-1 antagonists, 5 alpha-reductase inhibitors, combination therapy, and surgery. Alpha-1 antagonists are considered first-line treatment for moderate-to-severe voiding symptoms, while 5 alpha-reductase inhibitors may be indicated for patients with significantly enlarged prostates and a high risk of progression. Combination therapy and antimuscarinic drugs may also be used in certain cases. Surgery, such as transurethral resection of the prostate (TURP), may be necessary in severe cases.
-
This question is part of the following fields:
- Surgery
-
-
Question 87
Incorrect
-
A 55-year-old motorcyclist is involved in a head-on collision with a truck. The air ambulance arrives at the scene and finds that the patient's Glasgow Coma Scale (GCS) is 6 (E2, V1, M3) and he has no air entry on the right side of the chest, with an open fractured neck of femur on the left side. His vital signs are as follows: temperature 37.8ºC, heart rate 120 bpm, blood pressure 70/50 mmHg, SpO2 94% on air, and respiratory rate 24/min. The fractured femur is reduced at the scene, but due to the patient's low GCS, the decision is made to intubate him at the scene. What is the most appropriate agent for induction of anesthesia?
Your Answer: Suxamethonium
Correct Answer: Ketamine
Explanation:Ketamine is a suitable anaesthetic option for patients who are haemodynamically unstable. Other anaesthetic agents can cause hypotension, which can be dangerous for patients who are already experiencing low blood pressure. Ketamine is often used in prehospital settings for pain relief and intubation, as it does not reduce blood pressure or cause cardiosuppression. Propofol, suxamethonium, desflurane, and thiopental sodium are not ideal options for induction of anaesthesia in haemodynamically unstable patients due to their potential to cause hypotension or other adverse effects.
Overview of Commonly Used IV Induction Agents
Propofol, sodium thiopentone, ketamine, and etomidate are some of the commonly used IV induction agents in anesthesia. Propofol is a GABA receptor agonist that has a rapid onset of anesthesia but may cause pain on IV injection. It is widely used for maintaining sedation on ITU, total IV anesthesia, and daycase surgery. Sodium thiopentone has an extremely rapid onset of action, making it the agent of choice for rapid sequence induction. However, it may cause marked myocardial depression and metabolites build up quickly, making it unsuitable for maintenance infusion. Ketamine, an NMDA receptor antagonist, has moderate to strong analgesic properties and produces little myocardial depression, making it a suitable agent for anesthesia in those who are hemodynamically unstable. However, it may induce a state of dissociative anesthesia resulting in nightmares. Etomidate has a favorable cardiac safety profile with very little hemodynamic instability but has no analgesic properties and is unsuitable for maintaining sedation as prolonged use may result in adrenal suppression. Postoperative vomiting is common with etomidate.
Overall, each of these IV induction agents has specific features that make them suitable for different situations. Anesthesiologists must carefully consider the patient’s medical history, current condition, and the type of surgery being performed when selecting an appropriate induction agent.
-
This question is part of the following fields:
- Surgery
-
-
Question 88
Incorrect
-
A 65-year-old man comes to the emergency department complaining of intermittent abdominal pain for the past 24 hours. He is experiencing vomiting and has not been able to eat. During the examination, scleral icterus is observed, and there is guarding in the right upper quadrant. His vital signs show a heart rate of 110 bpm, respiratory rate of 25/min, temperature of 37.9ºC, and blood pressure of 100/60 mmHg. What is the probable diagnosis?
Your Answer: Mirizzi's syndrome
Correct Answer: Ascending cholangitis
Explanation:The correct diagnosis for this patient is ascending cholangitis, as evidenced by the presence of Charcot’s triad of fever, jaundice, and right upper quadrant pain. This condition is commonly caused by gallstones and is often seen in individuals with recurrent biliary colic. It is important to note that acute cholangitis is a medical emergency and requires immediate treatment with antibiotics and preparation for endoscopic retrograde cholangiopancreatography (ERCP).
Acute cholecystitis is a possible differential diagnosis, but it is less likely in this case as it typically presents without jaundice. Acute pancreatitis is also a potential differential, but it is characterized by epigastric pain that radiates to the back and is relieved by sitting up. A serum amylase or lipase test can help differentiate between the two conditions. Biliary colic is another possible diagnosis, but the presence of secondary infective signs and jaundice suggest a complication of gallstones, such as cholangitis.
Understanding Ascending Cholangitis
Ascending cholangitis is a bacterial infection that affects the biliary tree, with E. coli being the most common culprit. This condition is often associated with gallstones, which can predispose individuals to the infection. Patients with ascending cholangitis may present with Charcot’s triad, which includes fever, right upper quadrant pain, and jaundice. However, this triad is only present in 20-50% of cases. Other common symptoms include hypotension and confusion. In severe cases, Reynolds’ pentad may be observed, which includes the additional symptoms of hypotension and confusion.
To diagnose ascending cholangitis, ultrasound is typically used as a first-line investigation to look for bile duct dilation and stones. Raised inflammatory markers may also be observed. Treatment involves intravenous antibiotics and endoscopic retrograde cholangiopancreatography (ERCP) after 24-48 hours to relieve any obstruction.
Overall, ascending cholangitis is a serious condition that requires prompt diagnosis and treatment. Understanding the symptoms and risk factors associated with this condition can help individuals seek medical attention early and improve their chances of a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 89
Correct
-
A 60-year-old man with a long history of diabetes arrives at the emergency department complaining of excruciating pain around his 'rear end', inability to defecate due to the pain, and spiking temperatures. During the examination, the patient is unable to tolerate an anal examination, but the anus appears red and inflamed. What is the most probable cause of this man's symptoms?
Your Answer: Perianal abscess
Explanation:Understanding Perianal Abscesses
A perianal abscess is a type of anorectal abscess that occurs when pus collects within the subcutaneous tissue surrounding the anal sphincter. It is the most common form of anorectal abscess, accounting for around 60% of cases, and is more prevalent in men with an average age of 40 years. Symptoms include pain around the anus, hardened tissue in the anal region, and pus-like discharge from the anus. In some cases, patients may also experience systemic infection.
Perianal abscesses are typically caused by gut flora such as E. coli, although those caused by Staph. aureus are more likely to be a skin infection. Diagnosis can be made through inspection of the anus and digital rectal examination, with further investigations such as colonoscopy and blood tests used to determine underlying causes. Imaging such as MRI and transperineal ultrasound may also be used in complicated cases.
Treatment for perianal abscesses involves surgical incision and drainage under local anaesthetic, with the wound either packed or left open to heal over several weeks. Antibiotics may be used in cases of systemic infection, but are not typically used for wound healing. It is important to note that perianal abscesses are just one type of anorectal abscess, with others classified by the layers and planes they occupy, such as ischiorectal, supralevator, intersphincteric, and horseshoe abscesses.
Overall, understanding perianal abscesses and their causes, symptoms, and treatment options is important for proper diagnosis and management of this common condition.
-
This question is part of the following fields:
- Surgery
-
-
Question 90
Incorrect
-
A 38-year-old man comes to see his GP with concerns about his fertility. He and his partner have been trying to conceive for the past year without success. The patient has a history of diabetes mellitus and is a heavy smoker, consuming 30 cigarettes per day, and drinks 12 units of alcohol per week.
During the examination, the patient is found to be obese and has slight gynaecomastia. Upon testicular examination, a lump is detected on the right side that feels similar to a bag of worms. The lump does not disappear when the patient lies down, and he denies experiencing any pain or haematuria.
What is the most appropriate course of action for the patient's management?Your Answer: Routine referral to urology for surgery
Correct Answer: Urgent 2-week wait referral to urology
Explanation:The nutcracker angle, which refers to the compression of the renal vein between the abdominal aorta and the superior mesenteric artery, can cause varicocele and may indicate the presence of malignancy.
Understanding Renal Cell Cancer
Renal cell cancer, also known as hypernephroma, is a primary renal neoplasm that accounts for 85% of cases. It typically arises from the proximal renal tubular epithelium, with the clear cell subtype being the most common. This type of cancer is more prevalent in middle-aged men and is associated with smoking, von Hippel-Lindau syndrome, and tuberous sclerosis. While renal cell cancer is only slightly increased in patients with autosomal dominant polycystic kidney disease, it can present with a classical triad of haematuria, loin pain, and abdominal mass. Other features include pyrexia of unknown origin, endocrine effects, and paraneoplastic hepatic dysfunction syndrome.
The T category criteria for renal cell cancer are based on the size and extent of the tumour. For confined disease, a partial or total nephrectomy may be recommended depending on the tumour size. Patients with a T1 tumour are typically offered a partial nephrectomy, while those with larger tumours may require a total nephrectomy. Treatment options for renal cell cancer include alpha-interferon, interleukin-2, and receptor tyrosine kinase inhibitors such as sorafenib and sunitinib. These medications have been shown to reduce tumour size and treat patients with metastases. It is important to note that renal cell cancer can have paraneoplastic effects, such as Stauffer syndrome, which is associated with cholestasis and hepatosplenomegaly. Overall, early detection and prompt treatment are crucial for improving outcomes in patients with renal cell cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 91
Incorrect
-
A 26-year-old male is in need of immediate surgery after suffering from traumatic injuries to his right leg in a car accident. He has a family history of malignant hyperpyrexia and last consumed solid food 2 hours ago.
What would be considered unsafe for administration in this patient?Your Answer: Endotracheal tube
Correct Answer: Laryngeal mask
Explanation:A laryngeal mask is not suitable for non-fasted patients as it provides poor control against reflux of gastric contents, which can lead to aspiration during anaesthesia induction. Therefore, an endotracheal tube with an inflated cuff is a better option as it can protect the trachea and bronchial tree from aspirate. Ketamine is not contraindicated in this patient as it does not cause malignant hyperpyrexia, which is a concern due to the patient’s family history. Non-depolarising muscle relaxants are also not a concern for malignant hyperpyrexia.
Airway Management Devices and Techniques
Airway management is a crucial aspect of medical care, especially in emergency situations. In addition to airway adjuncts, there are simple positional manoeuvres that can be used to open the airway, such as head tilt/chin lift and jaw thrust. There are also several devices that can be used for airway management, each with its own advantages and limitations.
The oropharyngeal airway is easy to insert and use, making it ideal for short procedures. It is often used as a temporary measure until a more definitive airway can be established. The laryngeal mask is widely used and very easy to insert. It sits in the pharynx and aligns to cover the airway, but it does not provide good control against reflux of gastric contents. The tracheostomy reduces the work of breathing and may be useful in slow weaning, but it requires humidified air and may dry secretions. The endotracheal tube provides optimal control of the airway once the cuff is inflated and can be used for long or short-term ventilation, but errors in insertion may result in oesophageal intubation.
It is important to note that paralysis is often required for some of these devices, and higher ventilation pressures can be used with the endotracheal tube. Capnography should be monitored to ensure proper placement and ventilation. Each device has its own unique benefits and drawbacks, and the choice of device will depend on the specific needs of the patient and the situation at hand.
-
This question is part of the following fields:
- Surgery
-
-
Question 92
Correct
-
A 45-year-old man has been experiencing left shoulder pain for the last five years. Recently, this pain has become more severe, and he has been advised to undergo a left shoulder replacement surgery. The patient has a history of diabetes and high blood pressure, but no other medical conditions. During his preoperative evaluation, the patient inquires about eating and drinking before the surgery, as he will not be staying overnight and will be arriving at the hospital on the day of the procedure.
What is the appropriate information to provide to this patient regarding fasting times for elective surgery?Your Answer: You can eat solids up to six hours before, clear fluids two hours before and carbohydrate-rich drinks two hours before
Explanation:Pre-Operative Fasting Guidelines: What You Need to Know
When it comes to preparing for surgery, there are certain guidelines that patients must follow regarding their food and drink intake. Contrary to popular belief, patients do not always need to fast for extended periods of time before their procedure.
According to recent studies, prolonged fasting may not be necessary to prepare for the stress of surgery. However, there are still some important guidelines to follow. Patients should stop eating solid foods six hours before their operation, and most patients having morning surgery are made nil by mouth from midnight. Clear fluids can be consumed up to two hours before the procedure, but carbohydrate-rich drinks should be stopped two hours before surgery.
Carbohydrate-rich drinks are often used in enhanced recovery programs to increase energy stores postoperatively and aid in recovery and mobilization. It is important to note that eating solids two hours before the procedure can increase the risk of residual solids in the stomach at induction of anesthesia.
In summary, patients should follow these guidelines: stop eating solids six hours before surgery, stop consuming carbohydrate-rich drinks two hours before surgery, and continue clear fluids up until two hours before the procedure. By following these guidelines, patients can ensure a safe and successful surgery.
-
This question is part of the following fields:
- Surgery
-
-
Question 93
Incorrect
-
Which tumour marker is most effective in detecting hepatocellular carcinoma?
Your Answer: CEA
Correct Answer: Serum AFP
Explanation:Liver Tumours: Types, Diagnosis, and Treatment
Liver tumours can be classified as primary or metastatic. Primary liver tumours are relatively rare, with cholangiocarcinoma and hepatocellular carcinoma being the most common types. Hepatocellular carcinoma accounts for 75% of primary liver tumours and is often associated with chronic inflammatory activity, such as cirrhosis or chronic hepatitis B infection. Diagnosis is typically made through imaging modalities like CT or MRI, with elevated levels of a-fetoprotein being a common marker. Biopsy should be avoided as it can spread tumour cells. Treatment options include surgical resection, liver resection, transplantation, and tumour ablation. However, the poor overall survival rate of 15% at 5 years highlights the need for better treatment options.
Cholangiocarcinoma is the second most common type of primary liver malignancy, with up to 80% of tumours arising in the extrahepatic biliary tree. Primary sclerosing cholangitis is a major risk factor, and patients typically present with jaundice. Diagnosis is made through liver function tests, imaging methods like CT or MRI, and elevated levels of tumour markers like CA 19-9, CEA, and CA 125. Surgical resection offers the best chance of cure, but local invasion of peri hilar tumours and lobar atrophy can often make it impossible. Palliation of jaundice is important, but metallic stents should be avoided in those considered for resection. The poor survival rate of approximately 5-10% 5 year survival highlights the need for better treatment options.
In summary, liver tumours can be classified as primary or metastatic, with primary liver tumours being relatively rare. Hepatocellular carcinoma and cholangiocarcinoma are the most common types of primary liver tumours, with diagnosis typically made through imaging modalities and elevated tumour markers. Treatment options include surgical resection, liver resection, transplantation, and tumour ablation, but the poor overall survival rate highlights the need for better treatment options.
-
This question is part of the following fields:
- Surgery
-
-
Question 94
Incorrect
-
A 49-year-old man presents to the Emergency department with excruciating pain in his right loin that has been occurring in waves for the past 2 hours. The physician decides to prescribe analgesia to alleviate his discomfort. What would be the most suitable medication to administer at this point?
Your Answer: Co-codamol 30mg oral
Correct Answer: Diclofenac 75 mg IM
Explanation:NICE guidelines still advise the utilization of IM diclofenac as the primary treatment for acute renal colic due to its superior analgesic properties. While other analgesic options are also effective, they are not recommended as the first line of treatment for this condition.
The management of renal stones involves initial medication and investigations, including an NSAID for analgesia and a non-contrast CT KUB for imaging. Stones less than 5mm may pass spontaneously, but more intensive treatment is needed for ureteric obstruction or renal abnormalities. Treatment options include shockwave lithotripsy, ureteroscopy, and percutaneous nephrolithotomy. Prevention strategies include high fluid intake, low animal protein and salt diet, and medication such as thiazides diuretics for hypercalciuria and allopurinol for uric acid stones.
-
This question is part of the following fields:
- Surgery
-
-
Question 95
Incorrect
-
A 65-year-old woman undergoes a right hemicolectomy for colon cancer and four days later presents with vomiting, a distended abdomen, and absent bowel sounds. Her blood results show a CRP of 124 mg/l and a WBC count of 5.2 * 109/l. Nursing notes reveal no bowel movements since surgery. What is the probable cause of her clinical presentation?
Your Answer: Hirschsprung's disease
Correct Answer: Paralytic ileus
Explanation:Simple constipation is unlikely in this patient due to the presence of vomiting and absent bowel sounds, which suggests paralytic ileus, especially so soon after surgery. Additionally, constipation alone would not explain all of the patient’s symptoms and signs. As the patient underwent a right hemicolectomy, the caecum would have been removed, making caecal volvulus an unlikely diagnosis. The raised CRP is a normal response to surgery. While peritonitis is a possibility, it would typically present with severe abdominal pain, tenderness, guarding, and more significantly elevated inflammatory markers and fever. Hirschsprung’s disease, a congenital condition, is highly unlikely to present for the first time in a 67-year-old patient.
Postoperative ileus, also known as paralytic ileus, is a common complication that can occur after bowel surgery, particularly if the bowel has been extensively handled. This condition is characterized by a reduction in bowel peristalsis, which can lead to pseudo-obstruction. Symptoms of postoperative ileus include abdominal distention, bloating, pain, nausea, vomiting, inability to pass flatus, and difficulty tolerating an oral diet. It is important to check for deranged electrolytes, such as potassium, magnesium, and phosphate, as they can contribute to the development of postoperative ileus.
The management of postoperative ileus typically involves starting with nil-by-mouth and gradually progressing to small sips of clear fluids. If vomiting occurs, a nasogastric tube may be necessary. Intravenous fluids are administered to maintain normovolaemia, and additives may be used to correct any electrolyte disturbances. In severe or prolonged cases, total parenteral nutrition may be required. It is important to monitor the patient closely and adjust the treatment plan as necessary to ensure a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 96
Incorrect
-
A 49-year-old woman arrives at the surgical assessment unit with fever, right upper quadrant pain, and yellowing of the sclera. Imaging confirms ascending cholangitis. She has a history of multiple hospitalizations for biliary colic. What is the primary cause of this condition?
Your Answer: Staphylococcus aureus
Correct Answer: Escherichia coli
Explanation:Ascending cholangitis is commonly caused by E. coli, while Mycobacterium avium complex is unlikely to cause chronic diarrhea in immunodeficient patients. Clostridium difficile is also unlikely to cause this condition, as it typically follows an antibiotic course. Staphylococcus aureus would not be a likely cause of this condition, as it requires a breach in the skin to enter the body.
Understanding Ascending Cholangitis
Ascending cholangitis is a bacterial infection that affects the biliary tree, with E. coli being the most common culprit. This condition is often associated with gallstones, which can predispose individuals to the infection. Patients with ascending cholangitis may present with Charcot’s triad, which includes fever, right upper quadrant pain, and jaundice. However, this triad is only present in 20-50% of cases. Other common symptoms include hypotension and confusion. In severe cases, Reynolds’ pentad may be observed, which includes the additional symptoms of hypotension and confusion.
To diagnose ascending cholangitis, ultrasound is typically used as a first-line investigation to look for bile duct dilation and stones. Raised inflammatory markers may also be observed. Treatment involves intravenous antibiotics and endoscopic retrograde cholangiopancreatography (ERCP) after 24-48 hours to relieve any obstruction.
Overall, ascending cholangitis is a serious condition that requires prompt diagnosis and treatment. Understanding the symptoms and risk factors associated with this condition can help individuals seek medical attention early and improve their chances of a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 97
Incorrect
-
Which one of the following statements regarding male circumcision is correct?
Your Answer: It is available on the NHS in areas with a high Jewish or Islamic population
Correct Answer: Reduces the rate of HIV transmission
Explanation:Understanding Circumcision
Circumcision is a practice that has been carried out in various cultures for centuries. Today, it is mainly practiced by people of the Jewish and Islamic faith for religious or cultural reasons. However, it is important to note that circumcision for these reasons is not available on the NHS.
The medical benefits of circumcision are still a topic of debate. However, some studies have shown that it can reduce the risk of penile cancer, urinary tract infections, and sexually transmitted infections, including HIV.
There are also medical indications for circumcision, such as phimosis, recurrent balanitis, balanitis xerotica obliterans, and paraphimosis. It is crucial to rule out hypospadias before performing circumcision as the foreskin may be needed for surgical repair.
Circumcision can be performed under local or general anesthesia. It is a personal decision that should be made after careful consideration of the potential benefits and risks.
-
This question is part of the following fields:
- Surgery
-
-
Question 98
Incorrect
-
A 50-year-old male construction worker presents to the Emergency Department with new onset frank haematuria. He has been passing blood and clots during urination for the past three days. He denies any dysuria or abdominal pain. His vital signs are stable with a heart rate of 80 bpm and blood pressure of 130/80 mmHg. Upon examination, his abdomen is soft without tenderness or palpable masses in the abdomen or renal angles. He has a 30 pack-year history of smoking. What is the most appropriate initial investigation to determine the cause of his haematuria?
Your Answer: CT scan of the thorax, abdomen and pelvis with IV contrast
Correct Answer: Flexible cystoscopy
Explanation:When lower urinary tract tumour is suspected based on the patient’s history and risk factors, cystoscopy is the preferred diagnostic method for bladder cancer. If a bladder tumour is confirmed, a CT scan or PET-CT may be necessary to evaluate metastatic spread. While a CT-angiogram can identify a bleeding source, it is unlikely to be useful in this case as the patient is stable and a bleeding source is unlikely to be detected.
Bladder cancer is the second most common urological cancer, with males aged between 50 and 80 years being the most commonly affected. Smoking and exposure to hydrocarbons such as 2-Naphthylamine increase the risk of the disease. Chronic bladder inflammation from Schistosomiasis infection is a common cause of squamous cell carcinomas in countries where the disease is endemic. Benign tumors of the bladder, including inverted urothelial papilloma and nephrogenic adenoma, are uncommon.
Urothelial (transitional cell) carcinoma is the most common type of bladder malignancy, accounting for over 90% of cases. Squamous cell carcinoma and adenocarcinoma are less common. Urothelial carcinomas may be solitary or multifocal, with up to 70% having a papillary growth pattern. Superficial tumors have a better prognosis, while solid growths are more prone to local invasion and may be of higher grade, resulting in a worse prognosis. TNM staging is used to determine the extent of the tumor and the presence of nodal or distant metastasis.
Most patients with bladder cancer present with painless, macroscopic hematuria. Incidental microscopic hematuria may also indicate malignancy in up to 10% of females over 50 years old. Diagnosis is made through cystoscopy and biopsies or transurethral resection of bladder tumor (TURBT), with pelvic MRI and CT scanning used to determine locoregional spread and distant disease. Treatment options include TURBT, intravesical chemotherapy, radical cystectomy with ileal conduit, or radical radiotherapy, depending on the extent and grade of the tumor. Prognosis varies depending on the stage of the tumor, with T1 having a 90% survival rate and any T with N1-N2 having a 30% survival rate.
-
This question is part of the following fields:
- Surgery
-
-
Question 99
Incorrect
-
A 25-year-old man was driving under the influence of alcohol at a high speed, with his seat belt on. He crashed into a brick wall at approximately 140 km/h. Upon arrival at the emergency department, he was found to be in a comatose state. Although his CT scan showed no abnormalities, he remained in a persistent vegetative state. What is the probable underlying reason for this?
Your Answer: Subarachnoid haemorrhage
Correct Answer: Diffuse axonal injury
Explanation:Types of Traumatic Brain Injury
Traumatic brain injury can result in primary and secondary brain injury. Primary brain injury can be focal or diffuse. Diffuse axonal injury occurs due to mechanical shearing, which causes disruption and tearing of axons. intracranial haematomas can be extradural, subdural, or intracerebral, while contusions may occur adjacent to or contralateral to the side of impact. Secondary brain injury occurs when cerebral oedema, ischaemia, infection, tonsillar or tentorial herniation exacerbates the original injury. The normal cerebral auto regulatory processes are disrupted following trauma rendering the brain more susceptible to blood flow changes and hypoxia. The Cushings reflex often occurs late and is usually a pre-terminal event.
Extradural haematoma is bleeding into the space between the dura mater and the skull. It often results from acceleration-deceleration trauma or a blow to the side of the head. The majority of epidural haematomas occur in the temporal region where skull fractures cause a rupture of the middle meningeal artery. Subdural haematoma is bleeding into the outermost meningeal layer. It most commonly occurs around the frontal and parietal lobes. Risk factors include old age, alcoholism, and anticoagulation. Subarachnoid haemorrhage classically causes a sudden occipital headache. It usually occurs spontaneously in the context of a ruptured cerebral aneurysm but may be seen in association with other injuries when a patient has sustained a traumatic brain injury. Intracerebral haematoma is a collection of blood within the substance of the brain. Causes/risk factors include hypertension, vascular lesion, cerebral amyloid angiopathy, trauma, brain tumour, or infarct. Patients will present similarly to an ischaemic stroke or with a decrease in consciousness. CT imaging will show a hyperdensity within the substance of the brain. Treatment is often conservative under the care of stroke physicians, but large clots in patients with impaired consciousness may warrant surgical evacuation.
-
This question is part of the following fields:
- Surgery
-
-
Question 100
Incorrect
-
An 80-year-old man presents to the surgical assessment unit with vomiting and abdominal distension. He has been experiencing absolute constipation for the past three days and his abdomen has become increasingly distended. He also reports feeling nauseous and has been vomiting for the last day. The patient has a medical history of hypertension and takes ramipril.
Upon examination, the patient has a soft but significantly distended abdomen that is tympanic to percussion. Loud bowel sounds are audible. His vital signs are as follows: heart rate of 87 bpm, blood pressure of 135/87 mmHg, and temperature of 36.8ºC. An abdominal x-ray reveals a 'coffee-bean' sign, indicating a sigmoid volvulus.
What is the initial management approach for this condition?Your Answer:
Correct Answer: Decompression via rigid sigmoidoscopy and flatus tube insertion
Explanation:Flatus tube insertion is the primary management approach for unruptured sigmoid volvulus.
In elderly patients, sigmoid volvulus is a common condition that can be initially treated without surgery by decompressing the bowel using a flatus tube. This approach is preferred as surgery poses a higher risk in this age group. Flatus tube decompression typically leads to resolution of the volvulus without recurrence. If flatus tube decompression fails or recurrence occurs despite multiple attempts, the next step is to insert a percutaneous colostomy tube to decompress the volvulus.
Conservative management is not appropriate for patients with absolute constipation as the volvulus can become ischemic and perforate, which is associated with a high mortality rate. Anti-muscarinic agents are used to treat pseudo-obstruction, not volvulus. There is no evidence to support the need for a Hartmann’s procedure as perforation is not a concern.
Understanding Volvulus: A Condition of Twisted Colon
Volvulus is a medical condition that occurs when the colon twists around its mesenteric axis, leading to a blockage in blood flow and closed loop obstruction. Sigmoid volvulus is the most common type, accounting for around 80% of cases, and is caused by the sigmoid colon twisting on the sigmoid mesocolon. Caecal volvulus, on the other hand, occurs in around 20% of cases and is caused by the caecum twisting. This condition is more common in patients with developmental failure of peritoneal fixation of the proximal bowel.
Sigmoid volvulus is often associated with chronic constipation, Chagas disease, neurological conditions like Parkinson’s disease and Duchenne muscular dystrophy, and psychiatric conditions like schizophrenia. Caecal volvulus, on the other hand, is associated with adhesions, pregnancy, and other factors. Symptoms of volvulus include constipation, abdominal bloating, abdominal pain, and nausea/vomiting.
Diagnosis of volvulus is usually done through an abdominal film, which shows signs of large bowel obstruction alongside the coffee bean sign for sigmoid volvulus. Small bowel obstruction may be seen in caecal volvulus. Management of sigmoid volvulus involves rigid sigmoidoscopy with rectal tube insertion, while caecal volvulus usually requires operative management, with right hemicolectomy often being necessary.
-
This question is part of the following fields:
- Surgery
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)