-
Question 1
Incorrect
-
A 42-year-old man visits his GP complaining of heel pain that has been bothering him for four months. He mentions that the pain intensifies when he walks to and from work. The man has a BMI of 29 kg/m² and is being evaluated for diabetes mellitus. He has a medical history of asthma, generalized anxiety disorder, and Peyronie's disease.
What is the most appropriate initial course of action for his heel pain?Your Answer: Suggest simple stretch exercises, prescribe ibuprofen and review in 6 weeks
Correct Answer: Suggest weight loss, simple stretch exercises and resting the heel
Explanation:To manage plantar fasciitis, it is recommended to start with rest, stretching, and weight loss if the patient is overweight. Stretching exercises targeting the plantar fascia and Achilles tendon should be done three times a day. Orthotics and NSAIDs can be used, but only after trying the initial measures. It is important to note that the patient has asthma, so prescribing ibuprofen would not be appropriate. While a 6 week review is appropriate, it should also include monitoring weight loss as a key factor in managing the condition. Therefore, weight loss should be considered as the best initial step, given the patient’s BMI of 29.
Understanding Plantar Fasciitis
Plantar fasciitis is a prevalent condition that causes heel pain in adults. The pain is typically concentrated around the medial calcaneal tuberosity, which is the bony bump on the inside of the heel. This condition occurs when the plantar fascia, a thick band of tissue that runs along the bottom of the foot, becomes inflamed or irritated.
To manage plantar fasciitis, it is essential to rest the feet as much as possible. Wearing shoes with good arch support and cushioned heels can also help alleviate the pain. Insoles and heel pads may also be beneficial in providing additional support and cushioning. It is important to note that plantar fasciitis can take time to heal, and it is crucial to be patient and consistent with treatment. By taking these steps, individuals can effectively manage their plantar fasciitis and reduce their discomfort.
-
This question is part of the following fields:
- Musculoskeletal
-
-
Question 2
Correct
-
An 82-year-old man attends the GP practice with his daughter, who is concerned about her father's health and states that he has not been himself lately. For the past few months, he has had a reduced appetite and is spending most of his time in bed, despite waking up early each day. He is forgetting simple things like his grandson's name, appointments and conversations he has recently had, and seems uninterested in most things. He denies any visual or auditory hallucinations. He has a medical history of well controlled hypertension. His wife passed away several years ago. He scores 20 on a Mini-Mental State Examination.
What is the most likely diagnosis?Your Answer: Depression
Explanation:Differential Diagnosis of Cognitive Impairment: Depression, Alzheimer’s Disease, Vascular Dementia, Normal Ageing, and Normal Grief Reaction
This patient is presenting with cognitive impairment, but the underlying cause is unclear. Several potential diagnoses should be considered, including depression, Alzheimer’s disease, vascular dementia, normal ageing, and normal grief reaction.
Depression is a likely diagnosis due to the patient’s lack of interest in activities, low appetite, early morning wakening, and diminished concentration. However, it is important to rule out dementia as a differential diagnosis, as depression can present similarly to cognitive impairments.
Alzheimer’s disease is characterized by a gradual decline in cognitive function, with early changes in memory. Neurological examination is typically normal, and gait is rarely affected.
Vascular dementia, on the other hand, is usually sudden onset and can occur after a TIA or stroke. Neurological deficits are often present, with executive function and gait being affected early, and memory later.
Normal ageing does not present in the same way as this patient, as it is a more gradual decline without the depressive symptoms.
Finally, a normal grief reaction is unlikely to be the cause of this patient’s cognitive impairment, as his wife died several years ago.
A comprehensive dementia workup, including a series of baseline blood tests, cognitive assessment, and potentially a brain scan, should be performed to determine the underlying cause of this patient’s cognitive impairment.
-
This question is part of the following fields:
- Neurology
-
-
Question 3
Correct
-
An 80-year-old man complains of colicky pain in his lower abdomen that eventually subsides in the left iliac fossa (LIF). He is septic and has localized peritonitis in the LIF. What is the probable diagnosis?
Your Answer: Diverticulitis
Explanation:Colicky Abdominal Pain
Colicky abdominal pain is caused by the distension of the bowel wall, which is a hollow viscus. The pain is not well-localized but is typically felt in the upper, central, or lower regions of the abdomen, corresponding to the embryological development of the gut. The foregut, midgut, and hindgut regions are responsible for the epigastric, umbilical, and suprapubic pain, respectively.
When palpating the abdomen, tenderness can be felt on the surface, and deeper palpation can reveal the exact location of the tenderness. Rebound tenderness or percussion tenderness can be elicited by bouncing the parietal peritoneum against the inflamed organ. As inflammation progresses, localized ischemia and perforation may occur, resulting in somatic pain as the peritoneum becomes inflamed.
Movement becomes painful, breathing becomes shallow, and if the entire peritoneum is inflamed, the patient may experience a rigid abdomen and guarding. It is important to understand the different regions of the gut and their corresponding pain locations to properly diagnose and treat colicky abdominal pain.
-
This question is part of the following fields:
- Clinical Sciences
-
-
Question 4
Incorrect
-
An 82-year-old man is brought to see his general practitioner by his daughter, who reports a 3- to 4- month history of falls, intermittent confusion and worsening urinary incontinence. On examination, the man has an abbreviated mental test score (AMTS) of 4/10 but is otherwise well. There is no focal neurological deficit, but he is unable to walk without the assistance of his daughter. Routine investigations, including FBC, U&Es, RBG, LFTs, TFTs, Ca2+ and ESR, are all within normal limits. The diagnosis is later confirmed by serial lumbar puncture studies.
What is the most likely diagnosis?Your Answer: Wernicke's encephalopathy
Correct Answer: Normal pressure hydrocephalus
Explanation:Differential Diagnosis of a Patient with Gait Dyspraxia, Confusion, and Urinary Incontinence
The presenting symptoms of gait dyspraxia, fluctuating confusion, and urinary incontinence can be indicative of various conditions in the elderly population. However, the classical triad of normal pressure hydrocephalus (NPH) is a possible diagnosis that requires clinical expertise and imaging studies, such as a CT or MRI scan, to confirm the presence of hydrocephalus with relatively well-preserved sulci. Lumbar puncture studies can also aid in the diagnosis of NPH, and the insertion of a ventriculo-peritoneal shunt may be curative.
Idiopathic intracranial hypertension is a disease that primarily affects young women and can lead to devastating neurological effects, including blindness. Wernicke’s encephalopathy, caused by thiamine deficiency, is characterized by a progressive confusional state, ataxia, and ophthalmoplegia. Herpes encephalitis is a rapidly fatal cause of encephalitis that presents with severe headache, confusion, or reduced level of consciousness. However, the absence of a severe headache and the need for serial lumbar punctures to confirm the diagnosis make NPH a more likely diagnosis in this case.
A colloid cyst of the third ventricle is a benign tumor that is usually discovered incidentally on a brain scan. While it may cause fluctuating confusion and symptoms of raised intracranial pressure, including headaches, it would not require serial lumbar punctures to confirm the diagnosis. In rare cases, it may also cause weakness of the lower limbs and episodes of collapse.
-
This question is part of the following fields:
- Neurosurgery
-
-
Question 5
Incorrect
-
In case there is no intravenous access available, what is the next most favored way to administer adrenaline during a cardiac arrest?
Your Answer: Intramuscular
Correct Answer: Intraosseous
Explanation:Intraosseous Access as an Alternative to Intravenous Access in Emergency Situations
In emergency situations where intravenous access cannot be obtained quickly, intraosseous access should be attempted as it is preferred over endotracheal access. According to the Resuscitation Council (UK) guidelines, if intravenous access cannot be established within the first 2 minutes of resuscitation, gaining intraosseous access should be considered. This is particularly important during a cardiac arrest when epinephrine is an essential resuscitation drug. The recommended dose for intraosseous access is the same as intravenous access, which is 1 mg of 1:10,000 adrenaline each 3-5 minutes. Therefore, it is crucial for healthcare professionals to be trained in intraosseous access as it can be a life-saving alternative when intravenous access is not possible.
-
This question is part of the following fields:
- Anaesthetics & ITU
-
-
Question 6
Correct
-
A 50-year-old man presents with a chronic cough and shortness of breath. He has recently developed a red/purple nodular rash on both shins. He has a history of mild asthma and continues to smoke ten cigarettes per day. On examination, he has mild wheezing and red/purple nodules on both shins. His blood pressure is 135/72 mmHg, and his pulse is 75/min and regular. The following investigations were performed: haemoglobin, white cell count, platelets, erythrocyte sedimentation rate, sodium, potassium, creatinine, and corrected calcium. His chest X-ray shows bilateral hilar lymphadenopathy. What is the most likely underlying diagnosis?
Your Answer: Sarcoidosis
Explanation:Differential Diagnosis for a Patient with Chest Symptoms, Erythema Nodosum, and Hypercalcaemia: Sarcoidosis vs. Other Conditions
When a patient presents with chest symptoms, erythema nodosum, hypercalcaemia, and signs of systemic inflammation, sarcoidosis is a likely diagnosis. To confirm the diagnosis, a transbronchial biopsy is usually performed to demonstrate the presence of non-caseating granulomata. Alternatively, skin lesions or lymph nodes may provide a source of tissue for biopsy. Corticosteroids are the main treatment for sarcoidosis.
Other conditions that may be considered in the differential diagnosis include asthma, bronchial carcinoma, chronic obstructive pulmonary disease (COPD), and primary hyperparathyroidism. However, the presence of erythema nodosum and bilateral hilar lymphadenopathy are more suggestive of sarcoidosis than these other conditions. While hypercalcaemia may be a symptom of primary hyperparathyroidism, the additional symptoms and findings in this patient suggest a more complex diagnosis.
-
This question is part of the following fields:
- Respiratory
-
-
Question 7
Incorrect
-
A 70-year-old man is scheduled for circumcision due to phimosis and requires a penile block with local anaesthetic. He weighs 65 kg. The maximum safe dose of lidocaine is 3 mg/kg, and 7 mg/kg when combined with adrenaline. What is the safest option for local anaesthetic in this patient?
Your Answer: 25 ml of 1% Lidocaine with adrenaline 1:10,000
Correct Answer: 18 ml of 1% Lidocaine
Explanation:Understanding Local Anaesthetics and Adrenaline in Clinical Practice
Local anaesthetics are commonly used in clinical practice to block pain impulses along nerves by inhibiting sodium channels. The maximum safe dose of lidocaine for a patient can be calculated by multiplying 3 mg/kg by the patient’s weight. For example, a 60 kg patient can safely receive 180 mg (or 18 ml of 1% lidocaine).
When adrenaline is added to local anaesthetic, it has three effects: preventing bleeding by causing vasoconstriction, preventing systemic absorption of the local anaesthetic, and allowing larger doses to be used. However, adrenaline should never be used on pedicles that contain an end-artery, as it may cause ischaemic necrosis.
It is important to note that the usual concentration of adrenaline used is 1 : 100 000 to 1 : 400 000. Adrenaline is contraindicated in certain situations, such as when the patient has an end-artery or when the maximum safe dose of lidocaine has already been reached.
In summary, understanding the safe doses and contraindications of local anaesthetics and adrenaline is crucial in clinical practice to ensure patient safety and effective pain management.
-
This question is part of the following fields:
- Pharmacology
-
-
Question 8
Correct
-
A 65-year-old man, who presented to the Emergency Department a day before for uncontrollable epistaxis, has been admitted following Ear, Nose and Throat (ENT) referral. Bleeding was located and managed by posterior nasal packing. He had no complications following the procedure. However, on the next day, he developed fever, myalgia, hypotension, rashes in the oral mucocutaneous junctions, generalized oedema and several episodes of watery diarrhoea, with nausea and vomiting.
Which of the following investigations/findings would help you make a diagnosis?Your Answer: Culture and sensitivity of posterior nasal swab
Explanation:Interpreting Clinical Findings in a Patient with Posterior Nasal Swab Procedure
Toxic shock syndrome (TSS) is a potential complication of an infected posterior nasal swab in the management of epistaxis. Clinical signs and symptoms of multiorgan involvement, along with a positive swab from the posterior pharyngeal mucosa, would be diagnostic for TSS caused by Staphylococcus aureus. Blood cultures are not necessary for diagnosis, as they are positive in only 5% of cases. Eosinophilia is not characteristic of TSS, but rather a hallmark of drug reactions with eosinophilia and systemic symptoms (DRESS). Kawasaki’s disease, another systemic inflammatory disease, is characterised by an increase in acute phase reactants (ESR, CRP) and localised oedema. A non-blanching purpuric rash is typically seen in meningococcal infection and does not match with the clinical features and history of posterior nasal swab procedure in this patient.
-
This question is part of the following fields:
- ENT
-
-
Question 9
Correct
-
Which one of the following statements regarding osteosarcoma is true?
Your Answer: More than 90% of children survive to adulthood
Explanation:Retinoblastoma is a prevalent type of eye cancer that is commonly found in children, with an average age of diagnosis at 18 months. It is caused by a loss of function of the retinoblastoma tumor suppressor gene on chromosome 13, which is inherited in an autosomal dominant pattern. About 10% of cases are hereditary. The most common presenting symptom is the absence of red-reflex, which is replaced by a white pupil (leukocoria). Other possible features include strabismus and visual problems.
When it comes to managing retinoblastoma, enucleation is not the only option. Depending on how advanced the tumor is, other treatment options include external beam radiation therapy, chemotherapy, and photocoagulation. The prognosis for retinoblastoma is excellent, with over 90% of patients surviving into adulthood.
-
This question is part of the following fields:
- Paediatrics
-
-
Question 10
Incorrect
-
A three-year-old male is brought into the paediatric emergency department by his mother. He has been coughing for four days, producing green sputum and has been off his food. He has been drinking water but has only wet two nappies today. On examination, he has a moderate intercostal recession, right-sided lung crackles and appears withdrawn. His mucous membranes appear dry.
Based on the NICE traffic light system, which symptom of the child is the most worrying?Your Answer: Reduced urine output
Correct Answer: Moderate intercostal recession
Explanation:In paediatric patients with a fever, moderate intercostal recession is a concerning sign. It is considered a ‘red’ flag on the NICE traffic light system, indicating a potentially serious condition. Other ‘amber’ signs to watch for include nasal flaring, lung crackles on auscultation, reduced nappy wetting, dry mucous membranes, and pallor reported by parent or carer. ‘Red’ signs that require immediate attention include not waking if roused, reduced skin turgor, mottled or blue appearance, and grunting.
The NICE Feverish illness in children guidelines were introduced in 2007 and updated in 2013. These guidelines use a ‘traffic light’ system to assess the risk of children under 5 years old presenting with a fever. It is important to note that these guidelines only apply until a clinical diagnosis of the underlying condition has been made. When assessing a febrile child, their temperature, heart rate, respiratory rate, and capillary refill time should be recorded. Signs of dehydration should also be looked for. Measuring temperature should be done with an electronic thermometer in the axilla if the child is under 4 weeks old or with an electronic/chemical dot thermometer in the axilla or an infrared tympanic thermometer.
The risk stratification table includes green for low risk, amber for intermediate risk, and red for high risk. The table includes categories such as color, activity, respiratory, circulation and hydration, and other symptoms. If a child is categorized as green, they can be managed at home with appropriate care advice. If they are categorized as amber, parents should be provided with a safety net or referred to a pediatric specialist for further assessment. If a child is categorized as red, they should be urgently referred to a pediatric specialist. It is important to note that oral antibiotics should not be prescribed to children with fever without an apparent source, and a chest x-ray does not need to be routinely performed if a pneumonia is suspected but the child is not going to be referred to the hospital.
-
This question is part of the following fields:
- Paediatrics
-
-
Question 11
Correct
-
A previously healthy 85-year-old woman presents to the surgical admissions unit after being referred by her GP due to a two-day history of increasing pain and swelling in the right groin area. Upon examination, there is a firm and red swelling that extends from the pubic tubercle downwards and outwards. What is the probable diagnosis?
Your Answer: Femoral hernia
Explanation:Types of Hernias and their Characteristics
Inguinal hernias are the most common type of hernia in adults, while femoral hernias are more commonly seen in elderly females. The femoral canal is formed by several ligaments and opens at the femoral ring, which is located inferolaterally to the pubic tubercle. On the other hand, inguinal hernias open at the superficial inguinal ring, which is found superolateral to the pubic tubercle. Therefore, options A and D are incorrect.
Incisional hernias occur at a previous site of surgery where the underlying tissue has been weakened. This type of hernia can occur anywhere on the abdomen where surgery has taken place. However, in the absence of any previous surgery or scar, it is not the correct answer.
Spigelian hernias occur in the abdominal wall within the aponeurotic layer between the rectus abdominis muscle medially and the semilunar line laterally. They do not present with a groin swelling.
In summary, there are different types of hernias, each with its own characteristics and location. It is important to correctly identify the type of hernia to determine the appropriate treatment.
-
This question is part of the following fields:
- Emergency Medicine
-
-
Question 12
Incorrect
-
A 78-year-old man with advanced adenocarcinoma of the colon and extensive pulmonary metastases reports experiencing breathlessness recently. He notices this when he takes just a few steps away from his bed. Despite trying controlled breathing techniques, he finds no relief from his breathing difficulties.
What is the next appropriate course of action for managing dyspnoea in this patient?Your Answer: Continuous non-invasive ventilatory support
Correct Answer: Systemic opioids (oral/subcutaneous/intravenous)
Explanation:Management Options for Dyspnoea in Palliative Care Patients
Dyspnoea is a common complaint in palliative care patients and requires appropriate management. Short-acting systemic opioids have been shown to be effective in alleviating dyspnoea in terminally ill patients, but caution should be exercised in patients with certain conditions. Heliox® and benzodiazepines may also be used in certain cases, but require expertise and careful consideration. Continuous non-invasive ventilatory support may be considered if other options fail, but requires adequate support. Nebulised opioids may also be a viable option depending on the underlying cause of dyspnoea. Treatment should be tailored to the individual patient’s needs.
-
This question is part of the following fields:
- Oncology
-
-
Question 13
Correct
-
A 56-year-old man presents with progressively worsening dysphagia, which is worse for food than liquid. He has lost several stones in weight and, on examination, he is cachexia. An oesophagogastroduodenoscopy (OGD) confirms oesophageal cancer.
Which of the following is the strongest risk factor for oesophageal adenocarcinoma?Your Answer: Barrett's oesophagus
Explanation:Understanding Risk Factors for Oesophageal Cancer
Oesophageal cancer is a type of cancer that is becoming increasingly common. It often presents with symptoms such as dysphagia, weight loss, and retrosternal chest pain. Adenocarcinomas, which are the most common type of oesophageal cancer, typically develop in the lower third of the oesophagus due to inflammation related to gastric reflux.
One of the risk factors for oesophageal cancer is Barrett’s oesophagus, which is the metaplasia of the squamous epithelium of the lower oesophagus when exposed to an acidic environment. This adaptive change significantly increases the risk of malignant change. Treatment options for Barrett’s oesophagus include ablative or excisional therapy and acid-lowering medications. Follow-up with repeat endoscopy every 2–5 years is required.
Blood group A is not a risk factor for oesophageal cancer, but it is associated with a 20% higher risk of stomach cancer compared to those with blood group O. A diet low in calcium is also not a risk factor for oesophageal carcinoma, but consumption of red meat is classified as a possible cause of oesophageal cancer. Those with the highest red meat intake have a 57% higher risk of oesophageal squamous cell carcinoma compared to those with the lowest intake.
Ulcerative colitis is not a risk factor for oesophageal cancer, but it is a risk factor for bowel cancer. On the other hand, alcohol is typically a risk factor for squamous cell carcinomas. Understanding these risk factors can help individuals take steps to reduce their risk of developing oesophageal cancer.
-
This question is part of the following fields:
- Gastroenterology
-
-
Question 14
Incorrect
-
A 62-year-old man presents to the pre-admission clinic for assessment prior to an elective prostatectomy. You find no adverse past medical history and examination is unremarkable. An electrocardiogram (ECG) is indicated in all pre-operative patients undergoing major surgery who are over the age of 60. The ECG is shown below.
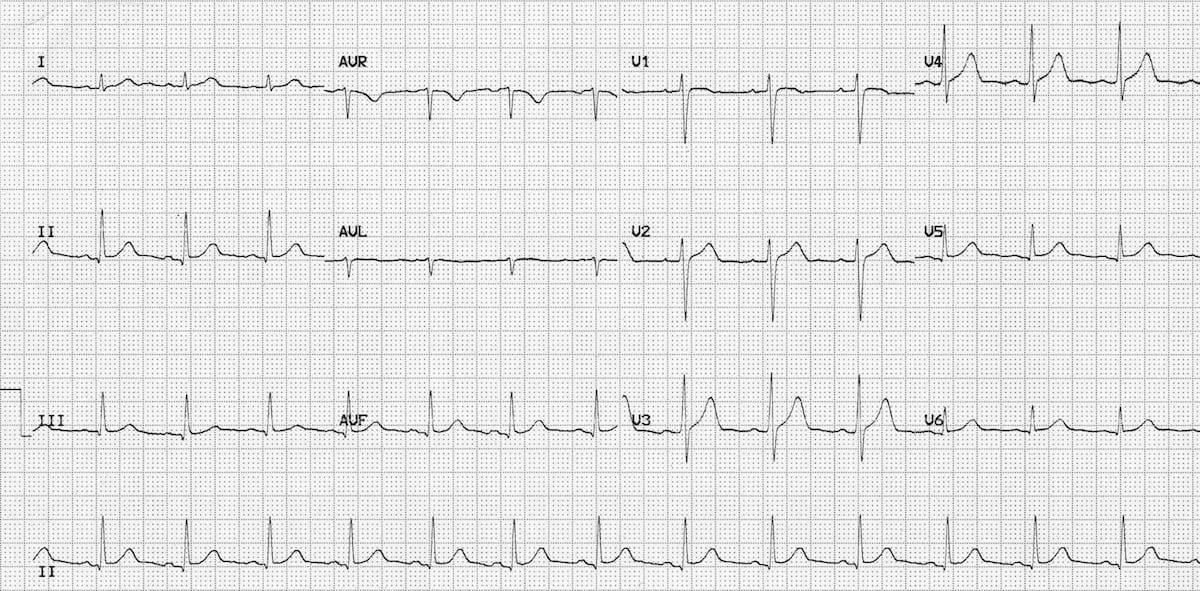 After having reviewed the ECG, what is the next best step to take with this patient?
After having reviewed the ECG, what is the next best step to take with this patient? Your Answer: Cancel the patient’s procedure as her current cardiac condition is too risky to proceed with major surgery
Correct Answer: No further assessment is required
Explanation:Assessing Cardiac Risk in Preoperative Patients: Common Misconceptions
There are several misconceptions when it comes to assessing cardiac risk in preoperative patients. One common mistake is assuming that all patients require extensive cardiac testing, even when there are no significant risk factors or symptoms present. For example, if a patient has no significant past medical history and their examination is unremarkable, an echocardiogram is not necessary.
On the other hand, some clinicians may be too cautious and cancel a patient’s procedure based on a perceived cardiac risk that is not supported by evidence. If the patient’s ECG is normal and there are no cardiac risk factors, cancelling the procedure would be unreasonable.
It is important to recognise that not all preoperative patients require extensive cardiac testing. Instead, clinicians should focus on identifying patients with specific cardiac conditions that require closer monitoring and management. By avoiding unnecessary testing and interventions, clinicians can improve patient outcomes and reduce healthcare costs.
-
This question is part of the following fields:
- Surgery
-
-
Question 15
Correct
-
A 70-year-old man contacts his primary care physician for guidance. He lost his wife to cancer and has been a widower for 6 months. The patient has a supportive family and is not experiencing clinical depression, but he was very emotional after his wife's passing. He occasionally feels indifferent and disheartened, but this has improved significantly over time. However, he has heard his late wife speaking to him on several occasions over the last 2 weeks. He also believed he saw her once while shopping with a friend, but he acknowledges that this is impossible. What is the most appropriate course of action for management?
Your Answer: Reassure and safety-net
Explanation:It is possible for pseudo hallucinations to be a normal part of the grieving process. People who are grieving may experience hearing, seeing, or smelling their deceased loved one, especially during acute grief. This can happen at any stage of bereavement. Therefore, the patient in question can be reassured that this is a common experience.
Since there is no evidence of an organic cause for the patient’s symptoms, it would not be appropriate to arrange blood tests or urinalysis.
While antidepressants may be used to treat severe or atypical cases of grief, the patient is not clinically depressed and is unlikely to benefit from them. In fact, they may cause harm due to their adverse effects.
The patient is fully aware of the situation and has insight into their condition. Therefore, there is no need for urgent psychiatric involvement or sectioning under the Mental Health Act 1983.
Understanding Pseudohallucinations
Pseudohallucinations are false sensory perceptions that occur in the absence of external stimuli, but with the awareness that they are not real. While not officially recognized in the ICD 10 or DSM-5, there is a general consensus among specialists about their definition. Some argue that it is more helpful to view hallucinations on a spectrum, from mild sensory disturbances to full-blown hallucinations, to avoid misdiagnosis or mistreatment.
One example of a pseudohallucination is a hypnagogic hallucination, which occurs during the transition from wakefulness to sleep. These vivid auditory or visual experiences are fleeting and can happen to anyone. It is important to reassure patients that these experiences are normal and do not necessarily indicate the development of a mental illness.
Pseudohallucinations are particularly common in people who are grieving. Understanding the nature of these experiences can help healthcare professionals provide appropriate support and reassurance to those who may be struggling with them. By acknowledging the reality of pseudohallucinations and their potential impact on mental health, we can better equip ourselves to provide compassionate care to those who need it.
-
This question is part of the following fields:
- Psychiatry
-
-
Question 16
Correct
-
You are participating in a morbidity and mortality meeting following the death of a patient on the 30th day after birth. The classification of the patient's death is being debated. What is the appropriate classification for this case?
Your Answer: Neonatal death
Explanation:Neonatal death is the term used to describe the death of a baby within the first 28 days of life. This classification is important for public health interventions and is a common topic in exams. Miscarriage, on the other hand, is defined as the death of a fetus before 24 weeks of gestation in the UK, or before 28 weeks globally. Puerperal death refers to the death of a mother within the first 6 weeks after giving birth. Perinatal death is a broader term that includes stillbirths and deaths within the first week of life, often resulting from obstetric events. Early neonatal death refers to death within the first week of life, while late neonatal death refers to death after 7 days but before 28 days of life.
Perinatal Death Rates and Related Metrics
Perinatal mortality rate is a measure of stillbirths and early neonatal deaths within seven days per 1,000 births after 24 weeks of gestation. In the UK, this rate is around 6 per 1,000 births. This figure is usually broken down into 4 per 1,000 stillbirths and 2 per 1,000 early neonatal deaths.
Maternal mortality rate, on the other hand, is calculated by dividing the number of deaths during pregnancy, labor, and six weeks after delivery by the total number of maternities and multiplying the result by 1000. Meanwhile, the stillbirth rate is determined by dividing the number of babies born dead after 24 weeks by the total number of births (live and stillborn) and multiplying the result by 1000. Lastly, the neonatal death rate is computed by dividing the number of babies who died between 0-28 days by the total number of live births and multiplying the result by 1000.
These metrics are important in assessing the quality of perinatal care and identifying areas for improvement. By monitoring these rates, healthcare providers can work towards reducing perinatal deaths and improving maternal and neonatal outcomes.
-
This question is part of the following fields:
- Paediatrics
-
-
Question 17
Incorrect
-
An 80-year-old woman presents to the Emergency department with a Pretibial laceration and skin flap after injuring her leg on furniture at home. She is currently taking prednisolone for polymyalgia rheumatica. What is the optimal approach to managing this injury?
Your Answer: Clean then suture the laceration with an absorbable suture
Correct Answer: Clean then steristrip the laceration
Explanation:Management of Pretibial Lacerations in Different Patient Populations
In managing Pretibial lacerations, the approach may vary depending on the patient’s age and skin condition. For young patients with good skin, suturing with non-absorbable sutures is usually done and removed after seven to 10 days. However, for elderly patients with thin skin or those taking warfarin or steroids, suturing may not be possible due to fragile skin. In this case, the wound is cleaned thoroughly and steristripped meticulously to promote skin healing. A non-adherent dressing and light bandage are applied, and the patient is advised to elevate the leg.
After a week, patients should be reviewed to monitor the wound’s progress. It is important to note that Pretibial lacerations may take several months to heal, and some may require skin grafting procedures. By tailoring the management approach to the patient’s specific needs, optimal wound healing can be achieved.
-
This question is part of the following fields:
- Emergency Medicine
-
-
Question 18
Incorrect
-
A parent brings her daughter in for surgery suspecting a squint. She believes her left eye is 'turned inwards'. You conduct a cover test to gather more information. What result would indicate a left esotropia?
Your Answer: On covering the right eye the left eye moves laterally to take up fixation
Correct Answer: On covering the left eye the right eye moves laterally to take up fixation
Explanation:Squints can be categorized based on the direction in which the eye deviates. If the eye turns towards the nose, it is called esotropia. If it turns towards the temporal side, it is called exotropia. If it turns upwards, it is called hypertropia, and if it turns downwards, it is called hypotropia. For instance, when the left eye is covered, the right eye may move laterally from its esotropic position towards the center to focus on an object.
Squint, also known as strabismus, is a condition where the visual axes are misaligned. There are two types of squints: concomitant and paralytic. Concomitant squints are more common and are caused by an imbalance in the extraocular muscles. On the other hand, paralytic squints are rare and are caused by the paralysis of extraocular muscles. It is important to detect squints early on as they can lead to amblyopia, where the brain fails to process inputs from one eye and favours the other eye over time.
To detect a squint, a corneal light reflection test can be performed by holding a light source 30cm from the child’s face to see if the light reflects symmetrically on the pupils. The cover test is also used to identify the nature of the squint. This involves asking the child to focus on an object, covering one eye, and observing the movement of the uncovered eye. The test is then repeated with the other eye covered.
If a squint is detected, it is important to refer the child to secondary care. Eye patches may also be used to help prevent amblyopia.
-
This question is part of the following fields:
- Ophthalmology
-
-
Question 19
Correct
-
A 50-year-old man presents to the hospital with acute knee pain, swelling, and stiffness that started last night. He is experiencing systemic symptoms with a temperature of 39.2ºC and is unable to bear weight. A joint aspiration is performed to confirm the diagnosis.
What is the recommended duration of antibiotic treatment for this patient's most likely diagnosis?Your Answer: 4-6 weeks
Explanation:Septic arthritis necessitates a prolonged antibiotic treatment of at least 4-6 weeks. The most probable diagnosis in this scenario is septic arthritis, as the patient is experiencing acute joint swelling and pain, along with systemic distress and a high fever. Joint aspiration is a crucial diagnostic tool that is likely to reveal purulent synovial fluid, which may test positive for the causative organism. Patients with septic arthritis should receive joint aspiration and an initial 2 weeks of intravenous antibiotics, followed by 2-4 weeks of oral antibiotics. Antibiotics are necessary for treating septic arthritis, and joint aspiration alone is insufficient and may lead to joint destruction and sepsis. Current British Society of Rheumatology guidelines (2006) recommend against antibiotic courses of 7 days and 2 weeks, as they are inadequate. However, some evidence suggests that 1 week of intravenous antibiotics followed by oral antibiotics may be as effective as longer intravenous courses in some patients. A lifelong course of antibiotics is not necessary in this case, although it may be used under expert supervision in patients with recurrent septic arthritis.
Septic Arthritis in Adults: Causes, Symptoms, and Treatment
Septic arthritis is a condition that occurs when bacteria infect a joint, leading to inflammation and pain. The most common organism that causes septic arthritis in adults is Staphylococcus aureus, but in young adults who are sexually active, Neisseria gonorrhoeae is the most common organism. The infection usually spreads through the bloodstream from a distant bacterial infection, such as an abscess. The knee is the most common location for septic arthritis in adults. Symptoms include an acute, swollen joint, restricted movement, warmth to the touch, and fever.
To diagnose septic arthritis, synovial fluid sampling is necessary and should be done before administering antibiotics if necessary. Blood cultures may also be taken to identify the cause of the infection. Joint imaging may also be used to confirm the diagnosis.
Treatment for septic arthritis involves intravenous antibiotics that cover Gram-positive cocci. Flucloxacillin or clindamycin is recommended if the patient is allergic to penicillin. Antibiotic treatment is typically given for several weeks, and patients are usually switched to oral antibiotics after two weeks. Needle aspiration may be used to decompress the joint, and arthroscopic lavage may be required in some cases.
-
This question is part of the following fields:
- Musculoskeletal
-
-
Question 20
Incorrect
-
How would you describe March fracture?
Your Answer: Stress fracture of the neck of the talus
Correct Answer: Stress fracture of the neck of the second metatarsal
Explanation:March Fracture: A Common Injury in Active Individuals
March fracture is a type of stress fracture that affects the metatarsals, commonly seen in individuals who engage in repetitive activities such as running or walking. This injury is often observed in army recruits, nurses, and runners. One of the primary symptoms of March fracture is the development of a tender lump on the back of the foot, which can be felt just below the midshaft of a metatarsal bone, usually the second one.
While early radiology tests may not show any abnormalities, later tests may reveal a hairline fracture or the formation of callus in more severe cases. Fortunately, March fracture does not cause any displacement, so there is no need for reduction or splinting. Instead, normal walking is encouraged, and the forefoot may be supported with elastoplast to alleviate pain.
It typically takes around five to six weeks for the pain to subside, as the fracture heals and unites. the symptoms and treatment options for March fracture can help individuals who engage in repetitive activities take the necessary precautions to prevent this common injury.
-
This question is part of the following fields:
- Surgery
-
-
Question 21
Correct
-
A 20-year-old man presents with complaints of palpitations and dizzy spells. Upon performing an echocardiogram, the diagnosis of hypertrophic obstructive cardiomyopathy (HOCM) is made.
What will be visualized on the echocardiogram?Your Answer: Reduced left ventricular cavity size
Explanation:Echocardiographic Findings in Hypertrophic Obstructive Cardiomyopathy
Hypertrophic obstructive cardiomyopathy (HOCM) is a condition characterized by thickening of the heart muscle, particularly the septum, which can lead to obstruction of blood flow out of the heart. Echocardiography is a useful tool for diagnosing and monitoring HOCM. Here are some echocardiographic findings commonly seen in HOCM:
Reduced left ventricular cavity size: Patients with HOCM often have a banana-shaped left ventricular cavity, with reduced size due to septal hypertrophy.
Increased left ventricular outflow tract gradients: HOCM can cause obstruction of blood flow out of the heart, leading to increased pressure gradients in the left ventricular outflow tract.
Systolic anterior motion of the mitral leaflet: This is a characteristic finding in HOCM, where the mitral valve moves forward during systole and can contribute to obstruction of blood flow.
Asymmetrical septal hypertrophy: While some patients with HOCM may have symmetrically hypertrophied ventricles, the more common presentation is asymmetrical hypertrophy, with thickening of the septum.
Mitral regurgitation: HOCM can cause dysfunction of the mitral valve, leading to mild to moderate regurgitation of blood back into the left atrium.
Overall, echocardiography plays an important role in the diagnosis and management of HOCM, allowing for visualization of the structural and functional abnormalities associated with this condition.
-
This question is part of the following fields:
- Cardiology
-
-
Question 22
Correct
-
A 21-year-old student presents to the General Practitioner with complaints of passing bright red blood during bowel movements. The patient experiences severe pain each time they open their bowels, which has been ongoing for the past two weeks. The patient is now very anxious and avoids opening their bowels whenever possible, but this seems to worsen the pain symptoms. Rectal examination is not possible due to the patient's inability to tolerate the procedure because of pain.
What is the recommended treatment for the most likely diagnosis?Your Answer: Nitroglycerin ointment
Explanation:Anal Fissure: Causes, Symptoms, and Treatment Options
An anal fissure is a common condition that can occur at any age, but is most common in individuals aged 15-40. It can be primary, without underlying cause, or secondary, associated with conditions such as inflammatory bowel disease or constipation. Symptoms include severe anal pain during and after bowel movements, bleeding, and itching.
Treatment options include managing pain with simple analgesia and topical anesthetics, regular sitz baths, increasing dietary fiber and fluid intake, and stool softeners. Topical glyceryl trinitrate ointment may also be used to promote relaxation of the anal sphincter and aid healing. If the fissure remains unhealed after 6-8 weeks, surgical management options such as local Botox injection or sphincterotomy may be considered.
Antibiotic therapy does not have a role in the management of anal fissures, and band ligation is a secondary care option for the treatment of hemorrhoids, not anal fissures. Incision and drainage would only be indicated if the patient presented with a perianal abscess. Simple analgesia can be offered to manage pain symptoms, but opioid-containing preparations should be avoided to prevent further constipation and worsening of symptoms.
-
This question is part of the following fields:
- Colorectal
-
-
Question 23
Incorrect
-
A 65-year-old patient presents with acute severe abdominal pain and the following blood results:
Investigation Result Normal value
Haemoglobin 130 g/l
Female: 115–155 g/l
Male: 135–175 g/l
White cell count (WCC) 18 × 109/l 4–11 × 109/l
Sodium (Na+) 142 mmol/l 135–145 mmol/l
Potassium (K+) 4.2 mmol/l 3.5–5.0 mmol/l
Urea 22 mmol/l 2.5–6.5 mmol/l
Creatinine 95 μmol/l 50–120 μmol/l
Calcium 1.9 mmol/l 2.20–2.60 mmol/l
Lactate Dehydrogenase (LDH) 800 IU/l 50–120 IU/l
Albumin 30 g/l 35–50 g/l
Amylase 1600 U/l < 200 U/l
What is the most appropriate transfer location for ongoing care?Your Answer: Operating theatre
Correct Answer: Intensive care as an inpatient
Explanation:Appropriate Management of Acute Pancreatitis: A Case Study
A patient presents with acutely raised amylase, high white cell count (WCC), and high lactate dehydrogenase (LDH), indicating acute pancreatitis or organ rupture. The Glasgow system suggests severe pancreatitis with a poor outcome. In this case study, we explore the appropriate management options for this patient.
Intensive care as an inpatient is the most appropriate response, as the patient is at high risk for developing multi-organ failure. The modified Glasgow score is used to assess the severity of acute pancreatitis, and this patient meets the criteria for severe pancreatitis. Aggressive support in an intensive care environment is necessary.
Discharge into the community and general practitioner review in 1 week would be a dangerous response, as the patient needs inpatient treatment and acute assessment and treatment. The same applies to general surgical outpatient review in 1 week.
Operating theatre would be inappropriate, as no operable problem has been identified. Supportive management is the most likely course of action. If organ rupture is suspected, stabilisation of shock and imaging would likely be done first.
General medical ward as an inpatient is not the best option, as acute pancreatitis is a surgical problem and should be admitted under a surgical team. Additionally, the patient’s deranged blood tests, especially the low calcium and high WCC, indicate a high risk of developing multi-organ failure, requiring intensive monitoring.
In conclusion, appropriate management of acute pancreatitis requires prompt and aggressive support in an intensive care environment, with close monitoring of the patient’s condition.
-
This question is part of the following fields:
- Acute Medicine And Intensive Care
-
-
Question 24
Incorrect
-
A 25-year-old female has been discharged from hospital after being diagnosed with schizophrenia. She is now being seen in the GP clinic and is concerned about her prognosis. Prior to her illness, she was a high-functioning accountant. Her symptoms began gradually and mainly involved auditory hallucinations and persecutory delusions, which are currently under control. What factor in her case suggests a poor prognosis?
Your Answer: Predominant symptoms were auditory hallucinations and delusions
Correct Answer: Gradual onset of symptoms
Explanation:The gradual onset of schizophrenia is associated with a worse long-term outcome, making it a poor prognostic indicator for this patient. However, her gender (being female) and good pre-illness functioning are both positive prognostic indicators. Additionally, her predominant positive symptoms (auditory hallucinations and delusions) suggest a better prognosis compared to predominant negative symptoms. Lastly, being diagnosed at a younger age (such as in her teens) would have resulted in a poorer prognosis.
Schizophrenia is a mental disorder that can have varying prognosis depending on certain factors. Some indicators associated with a poor prognosis include a strong family history of the disorder, a gradual onset of symptoms, a low IQ, a prodromal phase of social withdrawal, and a lack of an obvious precipitant. These factors can contribute to a more severe and chronic course of the illness, making it more difficult to manage and treat. It is important for individuals with schizophrenia and their loved ones to be aware of these indicators and seek appropriate treatment and support.
-
This question is part of the following fields:
- Psychiatry
-
-
Question 25
Correct
-
A 59-year-old man presents to your clinic with a 6-month history of experiencing ‘tingling’ in his wrists and hands at night, with the right side being more affected than the left. Upon examination, you observe atrophy of the thenar eminence of his right hand. He displays slight weakness in thumb opposition and reduced sensation to light touch on the palmar surface of his right hand on the lateral three digits and the lateral half of the fourth digit. Reproduction of his symptoms occurs when you tap immediately distal to the wrist joint of his right hand for about 30 s.
Which nerve is implicated in this man’s condition?Your Answer: Median nerve
Explanation:Common Nerve Injuries in the Upper Limb
Nerve injuries in the upper limb can cause a range of symptoms, including pain, weakness, and sensory loss. Here are some of the most common nerve injuries and their associated symptoms:
1. Carpal Tunnel Syndrome (Median Nerve): Compression of the median nerve within the carpal tunnel can cause pain and loss of sensation in the lateral three-and-a-half digits. Symptoms are often worse at night and are more common in people who use their hands repetitively throughout the day.
2. Radial Neuropathy (Radial Nerve): Compression of the radial nerve at the spiral groove of the humerus can cause weakness of wrist and finger extension, as well as elbow flexion. There may also be sensory loss on the dorsum of the hand.
3. Ulnar Neuropathy (Ulnar Nerve): The ulnar nerve supplies sensation to the fifth digit and the medial aspect of the fourth digit, as well as the interosseous muscles of the hand. It is the second most commonly affected nerve in the upper limb after the median nerve.
4. Musculocutaneous Nerve: Weakness of elbow flexion and sensory loss over the lateral forearm can occur with musculocutaneous nerve palsy.
5. Long Thoracic Nerve: Injury to the long thoracic nerve affects the serratus anterior muscle, causing a winged scapula. This nerve is purely motor.
-
This question is part of the following fields:
- Neurology
-
-
Question 26
Correct
-
A 50-year-old woman comes to the clinic with creamy nipple discharge. She had a mammogram screening a year ago which was normal. She smokes 10 cigarettes per day. Upon examination, there were no alarming findings. A repeat mammogram was conducted and no abnormalities were detected. Although she is concerned about the possibility of a tumor, she is not bothered by the discharge itself. Her serum prolactin level is provided below.
Prolactin 200 mIU/L (<600)
What is the most probable diagnosis and what would be the best initial treatment?Your Answer: Reassurance
Explanation:Duct ectasia does not require any specific treatment. However, lumpectomy may be used to treat breast masses if they meet certain criteria such as being small-sized and peripheral, and taking into account the patient’s preference. Mastectomy may be necessary for malignant breast masses if lumpectomy is not suitable. In young women with duct ectasia, microdochectomy may be performed if the condition is causing discomfort. It is also used to treat intraductal papilloma.
Understanding Duct Ectasia
Duct ectasia is a condition that affects the terminal breast ducts located within 3 cm of the nipple. It is a common condition that becomes more prevalent as women age. The condition is characterized by the dilation and shortening of the ducts, which can cause nipple retraction and creamy nipple discharge. It is important to note that duct ectasia can be mistaken for periductal mastitis, which is more common in younger women who smoke. Periductal mastitis typically presents with infections around the periareolar or subareolar areas and may recur.
When dealing with troublesome nipple discharge, treatment options may include microdochectomy for younger patients or total duct excision for older patients.
-
This question is part of the following fields:
- Surgery
-
-
Question 27
Correct
-
What is the preferred intravenous induction agent for anesthesia in day case procedures?
Your Answer: Propofol
Explanation:Comparison of Different Anesthetic Agents
Propofol is a short-acting anesthetic agent with an elimination half-life of four hours. It is commonly used for day case procedures and sedation in intensive care units. On the other hand, etomidate is no longer preferred due to its side effects such as postoperative nausea and vomiting, venous thrombosis, and interference with glucocorticoid production. Ketamine, a phencyclidine derivative, can cause hallucinations and nightmares. Methohexitone may lead to involuntary muscular movement and epileptiform activity on an EEG. Lastly, thiopentone has the longest elimination half-life of 12 hours, which can cause a prolonged hangover effect.
In summary, different anesthetic agents have their own advantages and disadvantages. It is important to choose the appropriate agent based on the patient’s condition and the type of procedure being performed.
-
This question is part of the following fields:
- Anaesthetics & ITU
-
-
Question 28
Correct
-
A 9-year-old girl is brought to see the General Practitioner (GP) by her father, who is concerned about her behaviour at home and school. Over the past 18 months, her father has noted problems with inattention, hyperactivity and impulsivity. Teachers have also been raising similar issues about her behaviour in school. Her symptoms are affecting her performance in school and her relationship at home with her parents and siblings.
Which one of the following conditions is she most likely to be diagnosed with?Your Answer: Attention deficit/hyperactivity disorder (ADHD)
Explanation:The patient is exhibiting signs of ADHD, which is characterized by persistent patterns of inattention, hyperactivity, and impulsivity that interfere with functioning or development. These symptoms must have been present before the age of 12 and evident in multiple settings for at least six months. However, there are no indications of autism spectrum disorder, learning difficulty, or learning disability. Additionally, the patient does not display any symptoms of oppositional defiance disorder, which is characterized by angry or irritable mood, argumentative behavior, or vindictiveness lasting at least six months and causing distress or impairment in social, educational, or occupational functioning.
-
This question is part of the following fields:
- Psychiatry
-
-
Question 29
Correct
-
A 45-year-old man is recovering on the surgical ward three days after a laparotomy and right hemicolectomy for cancer. You are asked to see him as he has developed a temperature of 38.5ºC and is tachycardic at 120 bpm and tachypnoeic at 25 breaths per minute. On examination his abdomen is soft and not distended but tender around his midline wound. There is some discharge seeping through the dressing. His chest is clear and he has no signs of a deep vein thrombosis.
What is the most probable cause of this man's elevated temperature?Your Answer: Wound infection
Explanation:Abdominal wound infections can lead to post-operative fevers after a few days and may be accompanied by signs of systemic infection. This is a common urgent call for junior surgeons, and the two main differentials to consider are infection and thrombosis, as they are the most serious causes of post-operative fever. Given that the operation involved the bowel and was not sterile, a wound infection is the most likely differential, especially with the presence of discharge and tenderness. While an anastomotic leak is possible, it would typically present with a painful, firm abdomen and severe sepsis. There are no indications of a chest pathology from the patient’s history or examination. A physiological cause of fever would not be associated with systemic inflammation symptoms, as seen in this case.
Post-operative pyrexia, or fever, can occur after surgery and can be caused by various factors. Early causes of post-op pyrexia, which typically occur within the first five days after surgery, include blood transfusion, cellulitis, urinary tract infection, and a physiological systemic inflammatory reaction that usually occurs within a day following the operation. Pulmonary atelectasis is also often listed as an early cause, but the evidence to support this link is limited. Late causes of post-op pyrexia, which occur more than five days after surgery, include venous thromboembolism, pneumonia, wound infection, and anastomotic leak.
To remember the possible causes of post-op pyrexia, it is helpful to use the memory aid of the 4 W’s: wind, water, wound, and what did we do? (iatrogenic). This means that the causes can be related to respiratory issues (wind), urinary tract or other fluid-related problems (water), wound infections or complications (wound), or something that was done during the surgery or post-operative care (iatrogenic). It is important to identify the cause of post-op pyrexia and treat it promptly to prevent further complications. This information is based on a peer-reviewed publication available on the National Center for Biotechnology Information website.
-
This question is part of the following fields:
- Surgery
-
-
Question 30
Incorrect
-
A 38-year-old man comes to his primary care clinic complaining of an itchy rash on his arm. During the examination, you observe polygonal, violaceous papules on the inner part of his forearm. Some of these papules have merged to form plaques. He has no history of skin disorders and is not presently taking any medications.
What is the most probable diagnosis?Your Answer: Atopic dermatitis
Correct Answer: Lichen planus
Explanation:Dermatological Disorders: Characteristics and Differences
Lichen planus is a skin disorder that is believed to be autoimmune in nature. It is characterized by a purple, polygonal, and papular rash that is often accompanied by itching. This condition is rare in both young and elderly populations and typically appears acutely on the flexor aspect of the wrists, forearms, and legs.
Atopic dermatitis, also known as eczema, is a condition that usually presents as a red, itchy rash on the flexural areas of joints such as the elbows and knees. It is most commonly seen in children under the age of 5. As the patient in question has no history of skin disease, it is unlikely that he has eczema.
Scabies is a contagious skin condition that is most commonly seen in children, young adults, and older adults in care homes. It causes widespread itching and linear burrows on the sides of fingers, interdigital webs, and the flexor aspect of the wrists.
Lichen sclerosus is a chronic inflammatory skin disease that typically presents with itchy white spots. It is most commonly seen on the vulva in elderly women or on the penis in men.
Plaque psoriasis is a skin condition that presents as itchy white or red plaques on the extensor surfaces of joints such as the elbows.
-
This question is part of the following fields:
- Dermatology
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)