-
Question 1
Correct
-
A 75-year-old retired teacher is brought to the general practitioner (GP) by her concerned son. He tells you that his mother had got lost when returning home from shopping yesterday, a trip that she had been carrying out without problems for over 20 years. He also notes that she has had a general decline in her memory function over the past year or so, frequently repeating stories, and not being able to remember if she had eaten a meal or not that day when questioned. The son would like to know if his mother could be tested for Alzheimer’s disease, a condition that also affected her maternal grandmother.
Deposition of which of the following is associated with the development of Alzheimer’s disease?Your Answer: Amyloid precursor protein (APP)
Explanation:Proteins Associated with Neurodegenerative Diseases
Neurodegenerative diseases are characterized by the progressive loss of neurons in the brain and spinal cord. Several proteins have been identified as being associated with these diseases. For example, Alzheimer’s disease is associated with both amyloid precursor protein (APP) and tau proteins. Lewy body disease and Parkinson’s disease are associated with alpha-synuclein, while fronto-temporal dementia and ALS are associated with TARDBP-43 and tau protein. Additionally, Huntington’s disease is associated with huntingtin. Other changes, such as bunina bodies and Pick bodies, are also seen in certain neurodegenerative diseases and can serve as markers of neuronal degeneration. Understanding the role of these proteins in disease pathology is crucial for developing effective treatments for these devastating conditions.
-
This question is part of the following fields:
- Neurology
-
-
Question 2
Correct
-
A nurse in the Emergency Department presents an electrocardiogram (ECG) to you. The elderly patient is feeling breathless and has long-standing limited mobility. The ECG shows a sinus tachycardia with an S-wave in lead I, Q-wave in lead III and T-wave inversion in lead III.
What is the most likely diagnosis?Your Answer: Pulmonary embolus
Explanation:Diagnosis of Pulmonary Embolus Based on ECG Findings
The ECG changes observed in this clinical presentation strongly suggest a pulmonary embolus. Pulmonary embolism occurs when a blood clot blocks one of the blood vessels in the lungs, leading to symptoms such as chest pain, breathlessness, and sudden collapse. Patients who are immobile or have undergone surgery are at a higher risk of developing this condition, which accounts for around 50% of cases that occur in hospital. To confirm the diagnosis, further tests such as a computed tomography pulmonary angiogram (CTPA) or ventilation/perfusion (V/Q) scan may be required. Although exacerbation of chronic obstructive pulmonary disease (COPD) is a possible differential diagnosis, the history of immobility, sinus tachycardia, and ECG changes make pulmonary embolism more likely. The ECG findings are not consistent with supraventricular tachycardia (SVT) or non-ST-segment elevation myocardial infarction (NSTEMI), and there is no evidence of ST-segment elevation myocardial infarction (STEMI).
-
This question is part of the following fields:
- Respiratory
-
-
Question 3
Incorrect
-
A 45-year-old Afro-Caribbean man presents to the Emergency Department with acute severe chest pain, fever and a cough, which he has had for five days. Examination revealed signs of jaundice and the spleen was not big enough to be palpable.
You take some basic observations:
Temperature: 38 °C
Respiratory rate: 26 breaths/min
O2 saturation: 86%
Heart rate: 134 bpm (regular)
Blood pressure (lying): 134/86 mmHg
Blood pressure (standing): 132/90 mmHg
His initial investigation findings are as follows:
Investigation Result Normal
White cell count (WCC) 13.8 × 109/l 4–11.0 × 109/l
Neutrophils 7000 × 106/l 3000–5800 × 106/l
Lymphocytes 2000 × 106/l 1500–3000 × 106/l
Haemoglobin (Hb) 105 g/l 135–175 g/l
Mean corpuscular volume (MCV) 110 fl 76–98 fl
Platelets 300 × 109/l 150–400 × 109/l
Troponin l 0.01 ng/ml < 0.1 ng/ml
D-dimer 0.03 μg/ml < 0.05 μg/ml
Arterial blood gas (ABG) showed type 1 respiratory failure with a normal pH. Chest X-ray showed left lower lobe consolidation.
The patient was treated successfully and is due for discharge tomorrow.
Upon speaking to the patient, he reveals that he has suffered two similar episodes this year.
Given the likely diagnosis, what medication should the patient be started on to reduce the risk of further episodes?Your Answer: Granulocyte colony-stimulating factor (G-CSF)
Correct Answer: Hydroxycarbamide (hydroxyurea)
Explanation:Treatment Options for a Patient with Sickle Cell Disease and Acute Chest Pain Crisis
A patient with sickle cell disease is experiencing an acute chest pain crisis, likely due to a lower respiratory tract infection. Hydroxycarbamide is recommended as a preventative therapy to reduce the risk of future crises by increasing the amount of fetal hemoglobin and reducing the percentage of red cells with hemoglobin S. Granulocyte colony-stimulating factor (G-CSF) is not necessary as the patient has a raised white blood cell count. Inhaled beclomethasone is not appropriate as asthma or COPD are not likely diagnoses in this case. Oral prednisolone may be used as a preventative therapy for severe asthma, but is not recommended for COPD and is not appropriate for this patient’s symptoms. A tuberculosis (TB) vaccination may be considered for primary prevention, but would not be useful for someone who has already been infected.
-
This question is part of the following fields:
- Haematology
-
-
Question 4
Correct
-
A 35-year-old recently arrived female with several skin blisters comes in for assessment. A few of the blisters have burst, resulting in a sore, exposed region. The base of one of the erosive lesions is scraped for Tzanck test. Upon examination, acantholytic keratinocytes with significant hyperchromatic nuclei are detected under the microscope.
What is the probable diagnosis?Your Answer: Pemphigus vulgaris
Explanation:Distinguishing Skin Conditions on Tzanck Smear: Pemphigus Vulgaris, Cytomegalovirus, Herpes Simplex, Chickenpox, and Bullous Pemphigoid
When examining a patient’s bullous skin lesions on a Tzanck smear, it is important to distinguish between various skin conditions. In the case of acantholytic keratinocytes, the most likely diagnosis is pemphigus vulgaris. This autoimmune disorder is caused by an antibody against intraepithelial desmosomal junctions, resulting in the separation of keratinocytes and the formation of intraepithelial blisters.
Cytomegalovirus, herpes simplex, and chickenpox can also present with multinucleated giant cells on a Tzanck smear. However, these conditions are caused by viral infections rather than autoimmune disorders.
Bullous pemphigoid, on the other hand, is caused by an antibody against the dermal-epidermal junction. The associated blisters are sub-epidermal in location and do not contain acantholytic keratinocytes.
In summary, a Tzanck smear can provide valuable information in diagnosing various skin conditions, including pemphigus vulgaris, cytomegalovirus, herpes simplex, chickenpox, and bullous pemphigoid. Proper diagnosis is crucial in determining the appropriate treatment plan for the patient.
-
This question is part of the following fields:
- Dermatology
-
-
Question 5
Correct
-
A 62-year-old man presents to the pre-admission clinic for assessment prior to an elective prostatectomy. You find no adverse past medical history and examination is unremarkable. An electrocardiogram (ECG) is indicated in all pre-operative patients undergoing major surgery who are over the age of 60. The ECG is shown below.
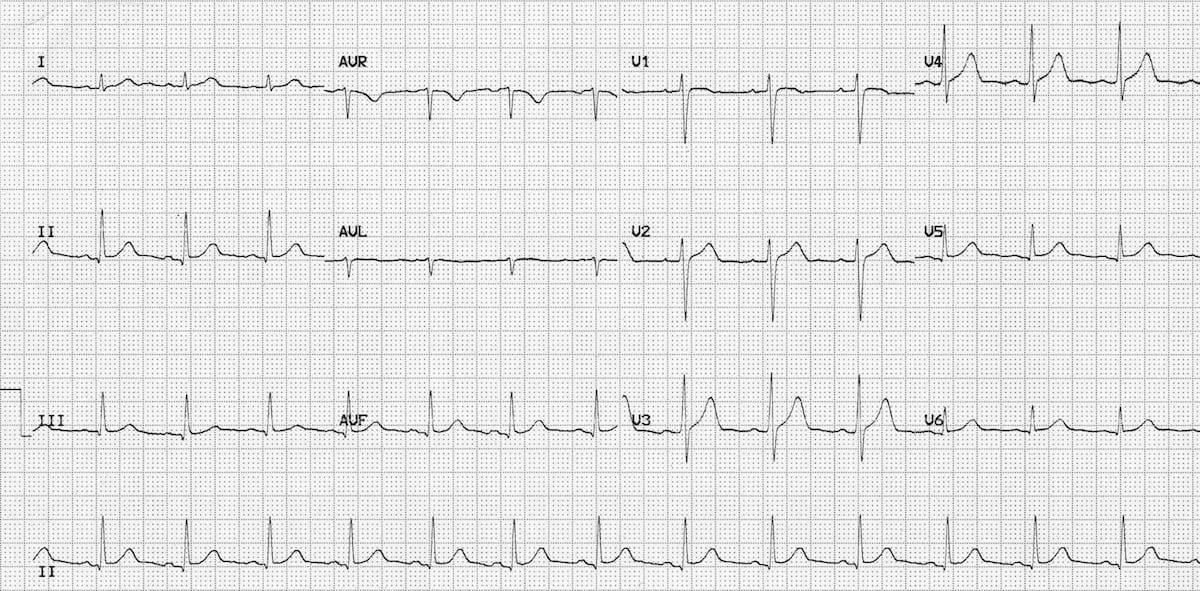 After having reviewed the ECG, what is the next best step to take with this patient?
After having reviewed the ECG, what is the next best step to take with this patient? Your Answer: No further assessment is required
Explanation:Assessing Cardiac Risk in Preoperative Patients: Common Misconceptions
There are several misconceptions when it comes to assessing cardiac risk in preoperative patients. One common mistake is assuming that all patients require extensive cardiac testing, even when there are no significant risk factors or symptoms present. For example, if a patient has no significant past medical history and their examination is unremarkable, an echocardiogram is not necessary.
On the other hand, some clinicians may be too cautious and cancel a patient’s procedure based on a perceived cardiac risk that is not supported by evidence. If the patient’s ECG is normal and there are no cardiac risk factors, cancelling the procedure would be unreasonable.
It is important to recognise that not all preoperative patients require extensive cardiac testing. Instead, clinicians should focus on identifying patients with specific cardiac conditions that require closer monitoring and management. By avoiding unnecessary testing and interventions, clinicians can improve patient outcomes and reduce healthcare costs.
-
This question is part of the following fields:
- Surgery
-
-
Question 6
Incorrect
-
What is the way in which ciprofloxacin works?
Your Answer: Inhibition of protein synthesis (translation)
Correct Answer: Interference with DNA replication
Explanation:Antibiotics and their Mechanisms of Action
Antibiotics are drugs that are used to treat bacterial infections. They work by targeting specific mechanisms within the bacteria to either kill or inhibit their growth. One example is ciprofloxacin, which disrupts the function of DNA gyrase and interferes with DNA synthesis. However, there are many other antibiotics that act by different mechanisms.
Penicillins and cephalosporins, as well as vancomycin, work by inhibiting the cell wall of bacteria. Trimethoprim and sulfamethoxazole, or co-trimoxazole, inhibit folic acid metabolism. Dapsone also works by inhibiting folic acid metabolism. Rifampicin inhibits transcription, while aminoglycosides and tetracyclines inhibit protein synthesis at the 30S subunit. Chloramphenicol, macrolides, and clindamycin inhibit protein synthesis at the 50S subunit.
the mechanisms of action of antibiotics is important in selecting the appropriate drug for a specific bacterial infection. It also helps in preventing the development of antibiotic resistance, as different mechanisms of action can be used in combination to target bacteria in different ways.
-
This question is part of the following fields:
- Clinical Sciences
-
-
Question 7
Correct
-
A 35-year-old man presents to the Emergency Department with sudden-onset, severe chest pain, radiating to the intrascapular area, which he describes as a tearing-type pain.
The patient is usually well, with the only other medical history of note being a diagnosis of Ehlers–Danlos syndrome. He is a non-smoker and rarely drinks.
On examination, the patient appears to be in a significant amount of pain. He is apyrexial, with oxygen saturation of 98% on room air. Of note, the patient has a blood pressure of 175/100 mmHg in the right arm and 150/80 mmHg in the left. An early diastolic murmur is also heard in the aortic area.
What is the most likely diagnosis?Your Answer: Aortic dissection
Explanation:Differential Diagnosis: Aortic Dissection
Aortic dissection is a medical emergency that occurs when there is a tear in the aortic intima, creating a false lumen between the intima and media. This condition is more likely to occur in men, older individuals, and those with hypertension or connective tissue disorders such as Marfan and Ehlers-Danlos syndromes.
The classic presentation of aortic dissection includes abrupt chest pain that is often described as a shearing or tearing-type pain that may radiate to the back. Other symptoms may include differences in blood pressure between the right and left arm, aortic regurgitation, and signs of malperfusion.
While a chest X-ray may show widening of the mediastinal shadow, imaging such as computed tomography (CT) or transoesophageal echocardiography is necessary to confirm the diagnosis. Treatment involves stabilizing the patient’s heart rate and blood pressure to prevent further damage, followed by surgical repair.
Although myocardial infarction is a differential diagnosis, the classical history of presentation, age, and connective tissue disorder diagnosis make aortic dissection more likely in this scenario. Other differentials, such as ruptured abdominal aortic aneurysm, acute pancreatitis, and pulmonary embolism, can be ruled out based on the patient’s symptoms and examination findings.
In conclusion, aortic dissection should be considered in any patient presenting with sudden-onset chest pain, especially those with risk factors for the condition. Early diagnosis and treatment are crucial in improving patient outcomes.
-
This question is part of the following fields:
- Cardiothoracic
-
-
Question 8
Correct
-
An 87-year-old man is brought into the emergency department by ambulance. He was found on his bathroom floor early this morning by his caregiver. He fell over last night, and had been unable to get up since then. He is now complaining of generalised aches and pains. He has no past medical history and does not take any regular medications.
On examination, he is cold and appears frail; he has a heart rate of 70/minute, and a blood pressure of 130/80 mmHg. His urine is also “muddy-looking'.
Blood tests showed the following:
pH 7.29
Bicarbonate 15 mmol/l
Creatine kinase 1559 u/l
Creatinine 301 µmol/l
Potassium 5.7 mmol/l
Routine blood tests a few weeks ago showed:
pH 7.41
Bicarbonate 27 mmol/l
Creatine kinase 99 u/l
Creatinine 61 µmol/l
Potassium 4.2 mmol/l
What is the underlying pathophysiology of this patient’s acute kidney injury (AKI)?Your Answer: Acute tubular necrosis
Explanation:The patient’s symptoms and history strongly suggest that their AKI is caused by rhabdomyolysis, which can lead to acute tubular necrosis. The patient’s prolonged immobility, muscle pain, and discolored urine (due to myoglobinuria) support this diagnosis, as does the metabolic acidosis seen on the VBG. The fact that the patient had normal kidney function just a few weeks ago suggests that this is an AKI rather than CKD. Renal artery stenosis is unlikely given the absence of hypertension, atherosclerosis, and antihypertensive medication use. While some forms of glomerulonephritis can cause a rapidly progressive AKI, the patient has not reported any other symptoms (such as hemoptysis) that would suggest this as a cause. Chronic interstitial nephritis typically results in a gradual decline in kidney function, which is not consistent with the patient’s rapid deterioration.
Acute tubular necrosis (ATN) is a common cause of acute kidney injury (AKI) that affects the functioning of the kidney by causing necrosis of renal tubular epithelial cells. The condition is reversible in its early stages if the cause is removed. There are two main causes of ATN: ischaemia and nephrotoxins. Ischaemia can be caused by shock or sepsis, while nephrotoxins can be caused by aminoglycosides, myoglobin secondary to rhabdomyolysis, radiocontrast agents, or lead. Features of ATN include raised urea, creatinine, and potassium levels, as well as muddy brown casts in the urine. Histopathological features include tubular epithelium necrosis, dilation of the tubules, and necrotic cells obstructing the tubule lumen. ATN has three phases: the oliguric phase, the polyuric phase, and the recovery phase.
-
This question is part of the following fields:
- Surgery
-
-
Question 9
Incorrect
-
An 80-year-old man is brought to the Emergency Department from a nursing home with fever and a non-healing infected ulcer in his leg. He has a history of obesity and type 2 diabetes. He reports that his leg was extremely painful but now is no longer painful. On clinical examination, his temperature is 38.6 °C, heart rate 110 bpm and blood pressure 104/69 mmHg. Peripheral pulses are palpable on examining his legs. There is tense oedema, dusky blue/purple plaques and haemorrhagic bullae on his right leg, with an underlying venous ulcer. Palpation reveals crepitus. After taking blood cultures, treatment is commenced with intravenous (IV) antibiotics and fluids.
What is the next and most important step in management?Your Answer: Magnetic resonance imaging (MRI) of the affected limb
Correct Answer: Surgical debridement in theatre
Explanation:Treatment Options for Necrotising Fasciitis
Necrotising fasciitis (NF) is a serious medical emergency that requires immediate surgical intervention. Antimicrobial therapy and support alone have shown to have a mortality rate of almost 100%. The primary goal of surgical intervention is to remove all necrotic tissue until healthy, viable tissue is reached. This can be done through surgical debridement in theatre or bedside wound debridement by a plastic surgeon in an aseptic environment.
Hyperbaric oxygen (HBO) treatment is believed to increase the bactericidal effects of neutrophils and can be useful in treating synergistic infections. However, access to HBO units with appropriate staffing and chambers large enough for intensive care patients is limited.
IV immunoglobulin (IVIG) has shown potential benefits in group A streptococcal (GAS) infections, but further studies are needed to determine its exact benefits in NF.
While X-ray, MRI, and CT scans can aid in the diagnosis of NF, surgical treatment should never be delayed for these tests. Immediate surgical intervention is crucial in treating this life-threatening condition.
-
This question is part of the following fields:
- Acute Medicine And Intensive Care
-
-
Question 10
Incorrect
-
A 49-year-old male has been experiencing a rash on and off for the past two years. Upon examination, it is noted that the rash is symmetrical and located on the cheeks, nose, and chin. The patient has multiple papules and pustules. What is the recommended treatment for this individual?
Your Answer: Flucloxacillin
Correct Answer: Oxytetracycline
Explanation:Acne Rosacea Treatment with Tetracycline
Acne rosacea is a skin condition that is characterized by the presence of redness, bumps, and pimples on the face. This condition is usually long-lasting and can be quite uncomfortable for those who suffer from it. Unlike other types of acne, acne rosacea does not typically present with blackheads or whiteheads. The distribution of the condition is usually limited to the face, particularly the cheeks, nose, and forehead.
The most effective treatment for acne rosacea is a medication called tetracycline. This medication is an antibiotic that works by reducing inflammation and killing the bacteria that cause acne. Tetracycline is usually taken orally, and it is important to follow the prescribed dosage and duration of treatment. In addition to tetracycline, there are other medications and topical treatments that can be used to manage the symptoms of acne rosacea. However, tetracycline is often the first line of treatment due to its effectiveness and low risk of side effects.
-
This question is part of the following fields:
- Dermatology
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Mins)