-
Question 1
Incorrect
-
In normal pregnancy, levels of all of the following hormones increases, EXCEPT:
Your Answer: Oestradiol
Correct Answer: Parathyroid hormone (PTH) in the 2nd & 3rd trimesters
Explanation:In order to maintain fetal bone growth, the maternal compartment undergoes adjustments that provide a net transfer of sufficient calcium to the foetus. Maternal compartment changes that permit calcium accumulation include increases in maternal dietary intake, increases in maternal 1, 25-dihydroxyvitamin D3 levels, and increases in parathyroid hormone (PTH) levels. The levels of total calcium and phosphorus decline in maternal serum, but ionized calcium levels remain unchanged. During pregnancy, the placenta forms a calcium pump in which a gradient of calcium and phosphorus is established which favours the foetus. Thus, circulating fetal calcium and phosphorus levels increase steadily throughout gestation. Furthermore, fetal levels of total and ionized calcium, as well as phosphorus, exceed maternal levels at term. By 10-12 weeks’ gestation, the fetal parathyroid glands secrete PTH. Fetal plasma levels of PTH are low during gestation, but increase after delivery.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 2
Incorrect
-
A 27-year-old woman presents for difficulty and pain in attempting sexual intercourse. She states that she never had such symptoms prior. The pain is not felt at the time of penetration, but appears to hurt deeper in the vagina. She was recently pregnant with her first child and delivery was three months ago. She did not have an episiotomy or sustain any vaginal lacerations during delivery. She denies any vaginal bleeding since her lochia had stopped two months ago. She is still breastfeeding her child. Which of the following is the most likely cause of her dyspareunia?
Your Answer: Trichomonas vaginitis.
Correct Answer: Atrophic vaginal epithelium.
Explanation:This is a patient that recently gave birth and is still breastfeeding presenting with dyspareunia. The most likely cause would be a thin atrophic vaginal epithelium. This is very common presentation and is due to the low oestrogen levels due to the prolactin elevation from breastfeeding.
An unrecognised and unsutured vaginal tear should have healed by this time and should not be causing issues.
Endometriosis tends to resolve during a pregnancy, but if this was the issue, it would have caused dyspareunia prior to pregnancy.
Vaginal infective causes of dyspareunia, such as monilial or trichomonal infections, are rare in amenorrhoeic women.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 3
Correct
-
Question 4
Correct
-
Regarding the biophysical profile:
Your Answer: Includes fetal movement, fetal tone, fetal breathing, fetal heart rate & amniotic fluid
Explanation:The biophysical profile is a composite test that collects 5 indicators of fetal well-being, including fetal heart rate reactivity, breathing movements, gross body movements, muscular tone, and quantitative estimation of amniotic fluid volume. The assessment of fetal heart rate is accomplished by performing a non-stress test, whereas the latter 4 variables are observed using real-time ultra-sonography.
-
This question is part of the following fields:
- Biophysics
-
-
Question 5
Correct
-
In relation to ovulation, when does the LH surge occur?
Your Answer: 24-36 hours before ovulation
Explanation:Ovulation usually occurs on day 14 in a typical 28-day cycle. Luteinizing hormone levels spike as a result of increased oestrogen levels secreted from maturing follicles. This LH spike occurs about 24-36 hours before the release of the oocyte from the mature follicle.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 6
Correct
-
A 28-year-old female patient comes in for a prenatal appointment. She eats only vegetables. Which of the following is the most appropriate suggestion for folic acid supplementation?
Your Answer: She should be started on folic acid 0.5 mg per day
Explanation:Folate has been in the news because of its connection with a type of birth defect called neural tube defect. Studies have shown that women who have infants with neural tube defects have lower intakes of folate and lower blood folate levels than other women. Folate is needed early in pregnancy (before many women know they are pregnant) for normal neural tube development.
Many vegan foods including enriched bread, pasta, and cold cereal; dried beans; green leafy vegetables; and orange juice are good sources of folate. Vegan diets tend to be high in folate, however, to be on the safe side, women capable of becoming pregnant should take a supplement or use fortified foods that provide 400 micrograms of folate daily.
For the above mentioned reasons, all other options are incorrect.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 7
Correct
-
A 60-year-old lady complains of a mild discomfort in her lower abdomen. She attained menopause 6 years ago whereas her last vaginal examination 2 years prior, was normal. She now has a palpable mass measuring 8cm in diameter in the left ovarian area. Which is the best next step in her management?
Your Answer: Admission to hospital for early surgical exploration.
Explanation:This lady should be admitted to hospital for early surgical exploration. Taking into account her age, mild abdominal discomfort and a palpable lower abdominal mass, it is imperative that ovarian malignancy be ruled out as soon as possible. Patients with ovarian malignancy often present in advanced stages of cancer as the symptoms tend to be occult and non-specific. Other things to include in her workup would be her CA125 level. Any form of hormonal therapy is contraindicated until ovarian malignancy has been ruled out. A pap smear is not relevant here since we are suspecting an ovarian malignancy rather than cervical. Evaluation of her mass takes priority over an assessment for osteoporosis.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 8
Correct
-
Which one of the following methods helps determine the fetal position and presentation?
Your Answer: Leopold's manoeuvre
Explanation:Fetal position and presentation is best evaluated by Leopold’s manoeuvre. It will determine which part of the foetus is in the uterine fundus.
Cullen’s sign is found in ruptured ectopic pregnancy characterised by bruising and oedema of the periumbilical region.
Mauriceau-Smelli-Veit manoeuvre is done during a breech delivery. -
This question is part of the following fields:
- Obstetrics
-
-
Question 9
Correct
-
You see a patient in antenatal clinic who is concerned that she has never had chicken pox and may catch it during pregnancy. You check her Varicella status and she is non-immune. She asks you about vaccination. What type of vaccine is the varicella vaccine?
Your Answer: Attenuated
Explanation:Varicella is a live vaccine. The recent RCOG green top guidelines suggest vaccine can be considered postpartum or pre pregnancy but NOT whilst pregnant. In the non-immune pregnant woman they should be advised to avoid contact with people with chickenpox or shingles and to contact a healthcare professional promptly if exposed. If they have a significant exposure VZIG should be offered as soon as possible.
-
This question is part of the following fields:
- Immunology
-
-
Question 10
Correct
-
What is the prevalence of antiphospholipid syndrome in patients with recurrent miscarriage?
Your Answer: 15%
Explanation:Anti phospholipid syndrome is an autoimmune disorder in which abnormal antibodies are formed which increases the risk of blood clots to develop in vessels and leads to recurrent miscarriages to occurs. The changes of recurrent miscarriage in a previously known case of APL is 15%.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 11
Incorrect
-
A patient admitted to the medical ward complains of a mild fever and vaginal discharge. Clue cells are seen on microscopy from a vaginal swab. Which of the following infections feature clue cells?
Your Answer: Neisseria gonorrhoea
Correct Answer: Bacterial Vaginosis
Explanation:Bacterial vaginosis (BV) is a common infection of the vagina caused by the overgrowth of atypical bacteria, most commonly Gardnerella vaginalis, a gram-negative rod. In diagnosing BV, a swab is taken for microscopy, often revealing clue cells. Clue cells are cells of the vaginal epithelium which are covered by adherent Gardnerella, giving them a distinctive look under the microscope. Though many are asymptomatic, some infected women complain of a greyish, foul-smelling vaginal discharge. Their vaginal fluid pH may also become more alkaline. BV does not however present with pyrexia, so the lady’s fever could be attributed to another cause as she is still a patient on the medical ward.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 12
Incorrect
-
A patient has had limited response to conservative measures for her overactive bladder (OAB). Which of the following is the most appropriate pharmacological choice?
Your Answer: Desmopressin
Correct Answer: Darifenacin
Explanation:Detrusor overactivity can be treated with anti-cholinergic agents such as oxybutynin or tolterodine, solifenacin, fesoterodine and darifenacin. They are used as first line agents. Imipramine is used for enuresis and desmopressin is used for nocturia.
NICE pathwayPrior to initiating anticholinergics:
Bladder training
Consider treating vaginal atrophy and nocturia with topical oestrogen and desmopressin respectively before commencing treatments below.
Consider catheterisation if chronic retention
1st line treatments:
1. Oxybutynin (immediate release) – Do not offer to frail elderly patients
2. Tolterodine (immediate release)
3. Darifenacin (once daily preparation)
DO NOT offer any of the 3 drugs below:
1. Flavoxate
2. Propantheline
3. Imipramine
2nd line treatment
Consider transdermal anticholinergic (antimuscarinic)
Mirabegron
Adjuvant Treatments
Desmopressin can be considered for those with nocturia
Duloxetine may be considered for those who don’t want/unsuitable for surgical treatment
Intravaginal oestrogen can be offered to postmenopausal women with OAB -
This question is part of the following fields:
- Clinical Management
-
-
Question 13
Correct
-
A 34 year old white primigravida in her first trimester had established moderate hypertension before becoming pregnant. She currently has a blood pressure of 168/108 mm Hg. You are considering how to best manage her hypertension during the pregnancy. Which one of the following is associated with the greatest risk of fetal growth retardation if used for hypertension throughout pregnancy?
Your Answer: Atenolol (Tenormin)
Explanation:Atenolol and propranolol are associated with intrauterine growth retardation when used for prolonged periods during pregnancy. They are class D agents during pregnancy. Other beta-blockers may not share this risk.
Methyldopa, hydralazine, and calcium channel blockers have not been associated with intrauterine growth retardation. They are generally acceptable agents to use for established, significant hypertension during pregnancy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 14
Correct
-
Question 15
Correct
-
Question 16
Correct
-
If a sample of cervical mucus is taken on the 12th day of the menstrual cycle and examined under the microscope, what kind of findings would be observed?
Your Answer: A fern pattern characteristic of oestrogen
Explanation:Fern test looks for a specific fern like pattern of cervical mucus when observed under light microscope after the sample is dried. It occurs due to the presence of sodium chloride under oestrogen influence whereas progesterone opposes it.
-
This question is part of the following fields:
- Physiology
-
-
Question 17
Correct
-
Where are ADH (vasopressin) and Oxytocin synthesised?
Your Answer: Hypothalamus
Explanation:ADH and vasopressin are synthesized in the supraoptic and periventricular nuclei of the hypothalamus, they are eventually transported to the posterior pituitary where they are stored to be released later.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 18
Correct
-
A 28-year-old, currently at 26 weeks’ gestation of her third pregnancy, presents with irregular uterine contractions for the past 24 hours and has concerns about premature delivery. She delivered her first child at 38 weeks of gestation and her second at 39 weeks gestation. On examination, BP and urinalysis have come back normal. Her symphysis-fundal height measures 27cm, the uterus is lax and non-tender. Fetal heart rate is 148/min. She also undergoes a pelvic examination along with other investigations. Which findings would suggest that delivery is most likely going to happen before 30 weeks’ of gestation?
Your Answer: The cervix is closed, but the fetal fibronectin test on cervical secretions is positive.
Explanation:Predisposing factors of preterm delivery include a short cervix (or if it shortens earlier than in the third trimester), urinary tract or sexually transmitted infections, open cervical os, and history of a previous premature delivery. Increased uterine size can also contribute to preterm delivery and is seen with cases of polyhydramnios, macrosomia and multiple pregnancies. The shorter the cervical length, the greater the risk of a premature birth.
In this case, the risk of bacterial vaginosis and candidiasis contributing to preterm delivery would be lower than if in the context of an open cervical os. However, the risk of premature delivery is significantly increased if it is found that the fetal fibronectin test is positive, even if the os is closed. -
This question is part of the following fields:
- Obstetrics
-
-
Question 19
Correct
-
Question 20
Correct
-
Regarding urinary tract infection (UTI) in pregnancy. What is the most common causative organism of urinary tract infection?
Your Answer: Escherichia coli
Explanation:E.coli is the most common cause of UTI. Other organisms include pseudomonas, proteus and klebsiella.
NICE guidelines: UTI in pregnancy (updated in July 2015)
Send urine for culture and sensitivity from all women in whom UTI is suspected before starting empirical antibiotics and 7 days after antibiotic treatment is completed.
Prescribe an antibiotic to all women with suspected UTI (awaiting culture result is not advised)
Although local antibiotic resistance needs to be taken into account the following is advised in terms of antibiotic selection:
1. Nitrofurantoin 50 mg QDS (or 100 mg MR BD) for 7 days.
2. Trimethoprim 200 mg twice daily, for 7 days
Give folic acid 5 mg OD if it is the 1st trimester
Do not give trimethoprim if the woman is folate deficient, taking a folate antagonist, or has been treated with trimethoprim in the past year.
3. Cefalexin 500 mg BD (or 250 mg 6qds) for 7 days -
This question is part of the following fields:
- Clinical Management
-
-
Question 21
Correct
-
A44-year-old woman underwent a cervical screening test at your clinic a week ago revealingInvasive squamous cell carcinoma. What is the best course of action for her management?
Your Answer: Refer to a gynaecologist at tertiary hospital
Explanation:If a cervical screening test reveals invasive squamous cell carcinoma or adenocarcinoma, refer the patient to a gynaecologist at a tertiary hospital right once for further treatment.
Colposcopy at a GP practice is not appropriate in these situations. When it comes to the prospect of cancer, reassurance isn’t enough. -
This question is part of the following fields:
- Gynaecology
-
-
Question 22
Correct
-
DEXA scans measure bone density by
Your Answer: Measuring absorption from two different XRAY beams with different energy peaks at the same site
Explanation:DEXA works by passing two low dose XRAY beams with different energy peaks at the patient’s bone. Some of the XRAY radiation will be absorbed (the greater the density the greater the absorption) whilst some will pass through to a detector. Soft tissue absorption is subtracted out and the BMD can be determined from the absorption of each beam. It is important to realise that two beams are used at each site when measuring bone density (hence ‘dual’). Although two sites are typically used (spine and femoral neck) when measuring bone density this is not why the term dual is used Computer analysis of multiple X-ray beams taken from different angles and geographical digital processing are features of CT scanning
-
This question is part of the following fields:
- Biophysics
-
-
Question 23
Correct
-
Question 24
Correct
-
A 32-year-old woman who is multigravida and with breech presentation presented to the emergency department for vaginal delivery. Upon spontaneous rupture of the membranes, bradycardia and variable deceleration was noted on the fetal heart rate monitoring. Vaginal examination was performed and revealed cord prolapse that is still pulsating. Which of the following is considered the most appropriate next step in managing the patient?
Your Answer: Arrange for emergency caesarean delivery
Explanation:Umbilical cord prolapse (UCP) occurs when the umbilical cord exits the cervical opening before the fetal presenting part. It is a rare obstetric emergency that carries a high rate of potential fetal morbidity and mortality. Resultant compression of the cord by the descending foetus during delivery leads to fetal hypoxia and bradycardia, which can result in fetal death or permanent disability.
Certain features of pregnancy increase the risk for the development of umbilical cord prolapse by preventing appropriate engagement of the presenting part with the pelvis. These include fetal malpresentation, multiple gestations, polyhydramnios, preterm rupture of membranes, intrauterine growth restriction, preterm delivery, and fetal and cord abnormalities.
The occurrence of fetal bradycardia in the setting of ruptured membranes should prompt immediate evaluation for potential cord prolapse.
In overt prolapse, the cord is palpable as a pulsating structure in the vaginal vault. In occult prolapse, the cord is not visible or palpable ahead of the fetal presenting part. The definitive management of umbilical cord prolapse is expedient delivery; this is usually by caesarean section.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 25
Incorrect
-
A 35 year old female presented with complaints of a 3 cm lump in her right breast, which was firm & irregular. O/E there was also some colour change over the breast. The most likely diagnosis would be?
Your Answer: Carcinoma
Correct Answer:
Explanation:Breast carcinoma is one of the most common malignancies in women. It presents as an irregular, firm consistency nodule/lump, which is attached to the skin most of the time. The overlying skin also exhibits a peau d’ orange appearance, along with dimpling. A sebaceous cyst is a small cystic swelling with no colour change and can occur anywhere over the skin. A lipoma is a benign tumour of fats which is soft in consistency.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 26
Correct
-
There are increasing rates of pregnancies among teenagers especially in low socioeconomic rural areas. What is the contraception method of choice for teenagers with high risk of unplanned pregnancy?
Your Answer: Intrauterine Contraceptive Device
Explanation:The use of long-acting reversible contraceptives (LARCs) is globally accepted as a strategy that is successful in decreasing rates of unintended pregnancy, especially in very young women.
Long-acting reversible contraceptives (LARCs) are defined as any contraceptive that requires administration less than once per cycle (i.e. per month). This includes copper and progestogen-only intrauterine devices (IUDs), and progestogen subdermal implants and injections. However, subdermal implants and IUDs, which have a life of at least three years, have superior efficacy over injections, which require administration every three months. Implants and IUDs are highly cost-effective when compared with other contraceptive methods.LARCs are widely recommended by professional bodies and the World Health Organization (WHO) as first-line contraception for young women as they are safe, effective and reversible. Young women should be offered the choice of a LARC as part of a fully informed decision for their first form of contraception.
LARCs surpass barrier methods and contraceptive pills in effectiveness and safety therefore all other options are incorrect.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 27
Correct
-
The resting pulse in pregnancy is:
Your Answer: Increased by 10 to 15 bpm
Explanation:During pregnancy cardiac output increases by 30 to 50%. As a result, the resting pulse speeds up from a normal of about 70 bpm to 80 or 90 bpm.
-
This question is part of the following fields:
- Physiology
-
-
Question 28
Correct
-
A 23-year-old pregnant woman, in her 19 weeks of pregnancy, presents to your office complaining of increased frequency and urgency along with dysuria. Further investigations established the diagnosis of urinary tract infection and the culture results are pending. The patient also mentioned a history of allergic reaction to penicillin which manifest as a rash. For treating this patient, which one of the following would be the antibiotic of choice?
Your Answer: Cephalexin
Explanation:The best antibiotic of choice for empirical treatment of a urinary tract infection (UTI) during pregnancy is cephalexin. Nitrofurantoin and amoxicillin-clavulanate are second and third in-line respectively.
Patients allergic to penicillin, which is manifested as a rash can also be safely treated with cephalexin. But cephalosporins are not recommended if the presentation of allergic reaction to penicillin was anaphylactic, instead they should be treated with nitrofurantoin.NOTE– Asymptomatic bacteriuria, such as >10 to power of 5 colony count in urine culture of an asymptomatic woman in pregnancy, should best be treated with a one week course of antibiotics, followed by confirming the resolution of infection via a urine culture repeated 48 hours after the completion of treatment.
Amoxicillin without clavulanate is recommended only in cases were the susceptibility of the organism is proven.
Macrolides like clarithromycin are usually not recommended for the treatment of UTI.
Aminoglycosides are coming under category D drugs should be avoided during pregnancy, unless there is a severe indication of gram negative sepsis.
Tetracycline, due to their potential teratogenic effects, are contraindicated in pregnancy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 29
Correct
-
A 24-year-old gravida 3 para 1 is admitted to the hospital at 29 weeks gestation with a high fever, flank pain, and an abnormal urinalysis. You order blood and urine cultures, a CBC, electrolyte levels, and a serum creatinine level. You also start her on intravenous fluids andintravenous cefazolin. After 24 hours of antibiotic treatment she is clinically improved but continues to have fever spikes. What would be the most appropriate management at this time?
Your Answer: Continue current management
Explanation:Pyelonephritis is the most common serious medical problem that complicates pregnancy. Infection is more common after midpregnancy, and is usually caused by bacteria ascending from the lower tract. Escheria coli is the offending bacteria in approximately 75% of cases. About 15% of women with acute pyelonephritis are bacteraemia- A common finding is thermoregulatory instability, with very high spiking fevers sometimes followed by hypothermia- Almost 95% of women will be afebrile by 72 hours. However, it is common to see continued fever spikes up until that time- Thus, further evaluation is not indicated unless clinical improvement at 48-71 hours is lacking. If this is the case, the patient should be evaluated for urinary tract obstruction, urinary calculi and an intrarenal or perinephric abscess. Ultrasonography, plain radiography, and modified intravenous pyelography are all acceptable methods, depending on the clinical setting.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 30
Correct
-
If your patient is 8 weeks pregnant which one of the following USS measurements is most useful?
Your Answer: Crown rump length
Explanation:Fetal crown-rump length (CRL) is recommended over last menstrual period for estimating GA when measured in early pregnancy i.e. before 9 to 13+6 weeks.
-
This question is part of the following fields:
- Anatomy
-
-
Question 31
Incorrect
-
A couple has decided to practice the daily basal body temperature assessment (BBT) as a means of contraception. Over the past year, her cycles varied in length from 24 to 30 days with menses lasting 4 days. They do not have sexual intercourse when she is on her period. Which regimen would be the most suitable to minimise the chances of getting pregnant?
Your Answer: Intercourse day 4 to 5 abstinence day 6 until two days after the temperature elevation of 0.3°C, intercourse thereafter.
Correct Answer: No intercourse in the follicular phase of the cycle, commence intercourse two days after temperature elevation of 0.3°C and continue thereafter.
Explanation:The best regimen would be to have no intercourse in the follicular phase of the cycle and then commence it two days after a temperature rise of 0.3C and continue then onwards. When deciding the best contraceptive method, one has to consider two factors-the duration of survival of sperm in the uterus and body temperature in relation to ovulation. For this case, since her cycle length varies from 24 to 30 days, the earliest time in which ovulation would occur would be 14 days before her shortest cycle i.e. day 10. Intercourse has to be avoided from day 4 of her cycle just in case the current cycle is short because sperm can survive up to 6 days in the uterus. Day 4 would be the day her menses would end and as this couple avoids intercourse during her menstruation, there would be no intercourse during the follicular phase of her cycle.
During ovulation, her serum progesterone levels would start to increase, causing a 0.3°C to 0.4°C increase in her body temperature within 2-3 days of ovulating. This elevation in temperature would remain until close to when her period starts. The ovum can only be fertilised for roughly 24 hours after ovulation has taken place. Resuming sexual intercourse once her temperature has risen for 2 days would suggest that ovulation had already taken place 3-4 days earlier and so it is unlikely for pregnancy to occur.
Options that include intercourse during any part of her follicular phase is not correct. Hence, the only option that satisfies the above criteria would be intercourse avoidance during her follicular phase and to resume 2 days following a rise of 0.03°C in body temperature.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 32
Correct
-
Which of the following hormones is secreted by the corpus luteum in a non pregnant state?
Your Answer: Progesterone
Explanation:The corpus luteum is formed from the granulosa cells of the mature follicle. The structure functions as a transient endocrine organ which secretes mainly progesterone with additional secretion of oestradiol and inhibin, which serve to suppress FSH levels. In the event of no pregnancy, the corpus luteum stops producing progesterone and degenerates into the corpus albicans.
-
This question is part of the following fields:
- Embryology
-
-
Question 33
Correct
-
Question 34
Incorrect
-
A 32 year old patient develops painful ulcerated genital lesions and inguinal lymphadenopathy. She is 32 weeks pregnant. You suspect genital herpes and send swabs. Which of the following is appropriate management according to the 2014 BASHH/RCOG guidelines?
Your Answer: Give Acyclovir 800mg 5 times daily for 5 days
Correct Answer: Send bloods to check antibody status. If this supports this is a first episode genital HSV then patient should be advised to have C-section delivery
Explanation:Although acyclovir should be given, this patient is in the 3rd trimester so the course should continue until delivery. Dose will be 400mg TDS unless disseminated disease. If this is a primary HSV infection (This should be confirmed by lesion swabs to confirm HSV infection and bloods to check no antibody response i.e. evidence previous infection) then C-section is indicated.
-
This question is part of the following fields:
- Microbiology
-
-
Question 35
Correct
-
A 30-year-old woman in her 36 weeks of gestation, presents for her planned antenatal appointment. On examination her blood pressure is 150/90 mmHg, in two consecutive readings 5 minutes apart. Which among the following statements is true regarding gestational hypertension and pre-eclampsia?
Your Answer: Pre-eclampsia involves other features in addition to the presence of hypertension
Explanation:Pre-eclampsia presents with other features in addition to the presence of hypertension, also it’s diagnosis cannot be made considered peripheral edema as the only presenting symptom. Proteinuria occurs more commonly in pre-eclampsia than in gestational hypertension and the latter is mostly asymptomatic.
Hypertensive disorders are found to complicate about 10% of all pregnancies. Common one among them is Gestational hypertension, which is defined as the new onset of hypertension after 20 weeks of gestation without any maternal or fetal features of pre-eclampsia, in this case BP will return to normal within three months of postpartum.
Types of hypertensive disorders during pregnancy:
1. Pregnancy-induced hypertension:
a. Systolic blood pressure (SBP) above 140 mm of Hg and diastolic hypertension above 90 mmHg occurring for the first time after the 20th week of pregnancy, which regresses postpartum.
b. The rise in systolic blood pressure above 25 mm of Hg or diastolic blood pressure above 15 mm of Hg from readings before pregnancy or in the first trimester.
2. Mild pre-eclampsia:
BP up to 170/110 mm of Hg in the absence of associated features.
3. Severe pre-eclampsia:
BP above 170/110 mm of Hg and along with features such as kidney impairment, thrombocytopenia, abnormal liver transaminase levels, persistent headache, epigastric tenderness or fetal compromise.
4. Essential (coincidental) hypertension:
Chronic underlying hypertension occurring before the onset of pregnancy or persisting after postpartum.
5. Pregnancy-aggravated hypertension:
Underlying hypertension which is worsened by pregnancy.To diagnose pre-eclampsia clinically, presence of one or more of the following symptoms are required along with a history of onset of hypertension after 20 weeks of gestation.
– Proteinuria: Above 300 mg/24 h or urine protein
reatinine ratio more than 30 mg/mmol.
– Renal insufficiency: serum/plasma creatinine above 0.09 mmol/L or oliguria.
– Liver disease: raised serum transaminases and severe epigastric or right upper quadrant pain.
– Neurological problems: convulsions (eclampsia); hyperreflexia with clonus; severe headaches with hyperreflexia; persistent visual disturbances (scotomata).
– Haematological disturbances like thrombocytopenia; disseminated intravascular coagulation; hemolysis. -
This question is part of the following fields:
- Obstetrics
-
-
Question 36
Correct
-
A 32-year-old woman at 37 weeks of gestation, who has been fine antenatally, presented with a history of sudden onset of severe abdominal pain with vaginal bleeding, and cessation of contractions after 18 hours of active pushing at home. On examination, she is conscious and pale. Her vital signs include blood pressure of 70/45 mm of Hg and a pulse rate of 115 beats per minute which is weak. Her abdomen is irregularly distended, with both shifting dullness and fluid thrill present. Fetal heart sounds are not audible. What will be the most likely diagnosis?
Your Answer: Uterine rupture
Explanation:Patient’s presentation is classic for uterine rupture, were she developed sudden abdominal pain followed by cessation of contractions, termination of urge to push and vaginal bleeding.
Abdominal examination shows no fetal cardiac activity and signs of fluid collection like fluid thrill and shifting dullness. The fluid collected will be blood, which usually enters the peritoneum after the rupture of the uterus. In such patients vaginal examination will reveal a range of cervical dilatation with evidences of cephalopelvic disproportion.
Anterior lower transverse segment is the most common site for spontaneous uterine rupture. Patient in the case presenting with tachycardia and hypotension is in shock due to blood loss and will require urgent resuscitation.Placenta previa presents with painless bleeding from the vagina and Placental abruption will present with painful vaginal bleeding with tender and tense uterine wall, however, in contrary to that of uterine rupture, uterine contractions will continue in both these cases.
Shoulder dystocia is more likely to present in a prolonged labour with a significant delay in the progress of labour. However, in this case, there is no mention of shoulder dystocia.
Disseminated intravascular coagulation (DIC) is a condition which is causes due to abnormal and excessive generation of thrombin and fibrin in the circulating blood which results in bleeding from every skin puncture sites. It results in increased platelet aggregation and consumption of coagulation factors which results in bleeding at some sites and thromboembolism at other sites. Placental abruption, or retained products of conception in the uterine cavity are the causes for DIC.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 37
Correct
-
Regarding cardiac examination during pregnancy which of the following findings should be considered pathological
Your Answer: Diastolic murmur
Explanation:Diastolic murmurs should be considered pathological until proven otherwise. The following are common and typically benign findings in pregnancy: A third heart sound after mid-pregnancy. Systolic flow murmurs are common. Left axis deviation on ECG is common, Sagging ST segments and inversion or flattening of the T wave in lead III may also occur
-
This question is part of the following fields:
- Physiology
-
-
Question 38
Correct
-
Which one of the following features indicates complete placental separation after delivery?
Your Answer: All of the options given
Explanation:At the time of delivery, the most important signs of complete placental separation are lengthening of the umbilical cord, per vaginal bleeding and change in shape of uterus from discoid to globular shape. The uterus contracts in size and rises upward.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 39
Correct
-
A 53 year old female presents with hot flushes and night sweats. Her last menstrual period was last year. She had MI recently. Choose the most appropriate management for this patient.
Your Answer: Clonidine
Explanation:With a history of MI, oestrogen and COCP should be avoided. Evening primrose is also not suitable for post-menopausal symptoms. Raloxifene is a SERM – these make hot flushes worse. Clonidine will help improve the hot flushes and the vasomotor symptoms.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 40
Correct
-
A 50-year-old woman, who had her last menstrual period at age 49, presented with an episode of per vaginal bleeding two weeks ago. It lasted four days in duration. A reduction in the severity of hot flushes as well as some breast enlargement preceded the bleeding episode. What is the most likely cause of the bleeding?
Your Answer: An episode of ovarian follicular activity.
Explanation:It has been found that it is possible for premenopausal hormones to persist for a period of time after attaining menopause. If one or a few ovarian follicles remain, they could produce oestrogen in response to the very elevated levels of FSH typically seen in menopause. In doing so, the woman can then bleed as a result of this physiological response. The symptoms seen in this vignette are consistent with the rise in oestrogen levels, likely due to follicular activity.
In the absence of any pathological findings such as endometrial carcinoma, this phenomenon would be the most likely cause of this post-menopausal bleed. Furthermore, it is unlikely for cervical cancer and endometrial cancer to present during the first few years following menopause. Atrophic vaginitis is unlikely to be associated with the other symptoms the patient presented with i.e. reduction in the intensity of hot flushes and breast enlargement. This patient was not stated to have any risk factors for endometrial hyperplasia such as obesity, late menopause and early menarche, which makes it a less likely diagnosis.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 41
Correct
-
WHO defines the perinatal mortality rate as
Your Answer: The number of stillbirths and deaths in the first week of life per 1000 births
Explanation:The number of stillbirths and deaths in the first week of life per 1000 births.
According to WHO the perinatal period commences at 22 completed weeks (154 days) of gestation and ends seven completed days after birth. -
This question is part of the following fields:
- Epidemiology
-
-
Question 42
Correct
-
A patient undergoes surgery for a vaginal vault prolapse. After surgery she complains of numbness and groin pain. You assess her and find the numb area is the anterior aspect of the labia. Which nerve has likely been damaged during surgery?
Your Answer: Ilioinguinal
Explanation:This describes the sensory area supplied by the ilioinguinal nerve. This is a potential complication with pelvic surgery.
-
This question is part of the following fields:
- Anatomy
-
-
Question 43
Correct
-
Question 44
Correct
-
CTG showing early decelerations is :
Your Answer: From increased vagal tone secondary to head compression
Explanation:Early decelerations: a result of increased vagal tone due to compression of the fetal head during contractions. Monitoring usually shows a symmetrical, gradual decrease and return to baseline of FHR, which is associated with a uterine contraction.
-
This question is part of the following fields:
- Physiology
-
-
Question 45
Correct
-
Which of the following dugs is a strong inducer of cytochrome P450?
Your Answer: Phenytoin
Explanation:Antiepileptic, phenytoin more so than topiramate are inducers of cytochrome P450. They should not be given with COCPs. The metabolism of oestrogen and progestogen is increased by anti-epileptic drugs that induce cytochrome P450 leading to a loss of contraceptive effect.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 46
Correct
-
A 32-year-old gravida 3 para 2 presents for routine prenatal care. The patient is at 14 weeks estimated gestational age by last menstrual period, and ultrasonography at 8 weeks gestation was consistent with these dates. Fetal heart tones are not heard by handheld Doppler. Transvaginal ultrasonography reveals an intrauterine foetus without evidence of fetal cardiac activity. The patient has not had any bleeding or cramping, and otherwise feels fine. A pelvic examination reveals a closed cervix without any signs of bleeding or products of conception. Which one of the following is the most likely cause of this presentation?
Your Answer: A missed abortion
Explanation:In this case, the patient has a missed abortion, which is defined as a dead foetus or embryo without passage of tissue and with a closed cervix. This condition often presents with failure to detect fetal heart tones or a lack of growth in uterine size.
– By 14 weeks estimated gestational age, fetal heart tones should be detected by both handheld Doppler and ultrasonography.
– An inevitable abortion presents with a dilated cervix, but no passage of fetal tissue.
– A blighted ovum involves failure of the embryo to develop, despite the presence of a gestational sac and placental tissue. -
This question is part of the following fields:
- Obstetrics
-
-
Question 47
Incorrect
-
According to the WHO, maternal mortality ratio is defined as which of the following?
Your Answer: Maternal deaths per 10,000 live births & stillbirths
Correct Answer: Maternal deaths per 100,000 live births
Explanation:The World Health Organisation defines the maternal mortality ratio as the number of maternal deaths during a given period per 100,000 live births during the same period. This measure indicates the risk of death in a single pregnancy.
-
This question is part of the following fields:
- Epidemiology
-
-
Question 48
Correct
-
Question 49
Correct
-
According to the RCOG Green-top guidelines on prevention and management of post-partum haemorrhage (PPH) which of the following statements is true?
Your Answer: For women delivering by caesarean section, Oxytocin 5 iu by slow IV injection should be used
Explanation:Misoprostol is not as effective as oxytocin but may be used if Oxytocin is not available e.g. home birth Recommended doses of Oxytocin For vaginal deliveries: 5 iu or 10 iu by intramuscular injection. For C-section: 5 iu by IV injection
-
This question is part of the following fields:
- Clinical Management
-
-
Question 50
Correct
-
All of the following are characteristic features of normal labour, except:
Your Answer: Moderate bleeding
Explanation:Normal labour is characterized by spontaneous onset, rhythmical uterine contractions along with vertex presentation. Cervical dilatation starts from the 1st stage of labour and intensity of the uterine contractions increases with passing time. Bleeding occurs after the child is expelled and the average loss is about 250-500 ml in a normal vaginal delivery.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 51
Incorrect
-
A 38 year old women attends clinic follow up. You note pelvic ultrasound shows a 36mm simple cyst. What is the most appropriate course of action regarding this cyst according to the RCOG green top guidelines?
Your Answer: Order Ca125
Correct Answer: Discharge with no follow up
Explanation:As this is a simple cyst less than 50mm in diameter the patient does not require further investigation or routine follow up
-
This question is part of the following fields:
- Clinical Management
-
-
Question 52
Correct
-
A 30 year old women who is 24 weeks pregnant attends clinic due to suprapubic pain. Ultrasound shows a viable foetus and also a fibroid with a cystic fluid filled centre. What is the likely diagnosis?
Your Answer: Cystic degeneration of fibroid
Explanation:A fibroid is a benign tumour of the smooth muscles of the uterus also known as a leiomyoma. It has a typical whorled appearance and this may be altered following degeneration which occurs in four main types:
1. Red degeneration, also known as carneous degeneration, of degeneration that can involve a uterine leiomyoma. While it is an uncommon type of degeneration, it is thought to be the most common form of degeneration of a leiomyoma during pregnancy. Red degeneration follows an acute disruption of the blood supply to the fibroid during growth typically in a mid-second trimester presenting as sudden onset of pain with tenderness localizing to the area of the uterus along with pyrexia and leucocytosis. On ultrasound it can have peripheral (rim).2. Hyaline degeneration is the most common form of degeneration that can occur in a uterine leiomyoma. It is thought to occur in up to 60% of uterine leiomyomasoccurs when the fibroid outgrows its blood supply. this may progresses to central necrosis leaving a cystic space in the centre knowns as cystic degeneration.
3. Cystic degeneration is an uncommon type of degeneration that a uterine leiomyoma (fibroid) can undergo. This type of degeneration is thought to represent ,4% of all types of uterine leiomyoma degeneration. When the leiomyoma increases in size, the vascular supply to it becomes inadequate and leads to different types of degeneration: hyaline, cystic, myxoid, or red degeneration. Dystrophic calcification may also occur. Hyalinization is the commonest type of degeneration. Cystic degeneration is an extreme sequel of edema. Ultrasound may show a hypoechoic or heterogeneous uterine mass with cystic areas.
4. Myxoid degeneration of leiomyoma is one of the rarer types of degeneration that can occur in a uterine leiomyoma. While this type of degeneration is generally considered rare, the highest prevalence for this type of degeneration has been reported as up to 50% of all degenerations of leiomyomas. Fibroids (i.e. uterine leiomyomas) that have undergone myxoid degeneration are filled with a gelatinous material and can be difficult to differentiate from cystic degeneration; however, they typically appear as more complex cystic masses. They appear hypocellular with a myxoid matrix.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 53
Correct
-
APGAR's score includes all the following, EXCEPT:
Your Answer: Blood pH
Explanation:Elements of the Apgar score include colour, heart rate, reflexes, muscle tone, and respiration. Apgar scoring is designed to assess for signs of hemodynamic compromise such as cyanosis, hypoperfusion, bradycardia, hypotonia, respiratory depression or apnoea. Each element is scored 0 (zero), 1, or 2. The score is recorded at 1 minute and 5 minutes in all infants with expanded recording at 5-minute intervals for infants who score 7 or less at 5 minutes, and in those requiring resuscitation as a method for monitoring response. Scores of 7 to 10 are considered reassuring.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 54
Incorrect
-
From which germ layer does the myenteric plexus of the GI tract developed:
Your Answer: Endoderm
Correct Answer: Neural crest of Ectoderm
Explanation:During the 5th week, the neural crest cells migrate along each side of the spinal cord where they form ganglions located dorsolateral to the aorta. Some of these cells migrate ventrally and form neurons in the preaortic ganglia as the celiac and mesenteric ganglia.
-
This question is part of the following fields:
- Embryology
-
-
Question 55
Correct
-
A 34-year-old woman presents to your clinic with a chief complaint of vague stomach pain. A unilocular cyst (3.8 x 4.3 x 3.0 cm) was discovered in the left ovary during a trans-abdominal ultrasound. What is the best management strategy?
Your Answer: Reassurance, no further action required
Explanation:In premenopausal women, watchful waiting usually involves monitoring for symptoms (pelvic pain or pressure) and repeating the pelvic ultrasound after six to eight weeks. If the ovarian cyst does not enlarge or if it resolves during the period of watchful waiting, it does not usually require surgical removal. Some premenopausal women will be advised to take a birth control pill during this time to help prevent new ovarian cysts from developing.
If a cyst decreases in size or does not change, the ultrasound is often repeated at regular intervals until your healthcare provider is certain that the cyst is not growing. If the cyst resolves, no further testing or follow-up is required.
Surgery may be recommended in the following situations:
– A cyst is causing persistent pain or pressure, or may rupture or twist.
– A cyst appears on ultrasound to be caused by endometriosis and is removed for fertility reasons.
– Large cysts (>5 to 10 cm) are more likely to require surgical removal compared to smaller cysts. However, a large size does not predict whether a cyst is cancerous.
– If the cyst appears suspicious for cancer. If you have risk factors for ovarian cancer or the cyst looks potentially cancerous on imaging studies, your healthcare provider may recommend surgery.
– If the suspicion for ovarian cancer is low but the cyst does not resolve after several ultrasounds, you may choose to have it removed after a discussion with your healthcare provider. However, surgical removal is not usually necessary in this case. -
This question is part of the following fields:
- Gynaecology
-
-
Question 56
Incorrect
-
A 25-year old Asian woman comes to your clinic at 36 weeks of gestation. She was diagnosed with breech at 32 weeks. She is not in labor and a manual examination of the uterus is suggestive of breech position. Which one of the following would be the next best step in management of this patient?
Your Answer: Cesarean delivery
Correct Answer: Pelvic ultrasound
Explanation:An ultrasonography is performed for confirmation, as well as for the evaluation of maternal pelvis, fetal size and viability in cases were breech presentation is suspected on manual examination. As there is a chance for spontaneous correction of breech presentation into cephalic during 36 to 37 weeks, this should be considered in every future visit. The chances for spontaneous version reduces to 25% if breech position persists beyond this period of time.
It an external cephalic version should be offered to all women with breech presentation, provided there are no contraindications or indication for cesarean delivery due to other reasons.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 57
Correct
-
Tamoxifen is associated with an increased risk of which of the following?
Your Answer: Endometrial cancer
Explanation:Tamoxifen is a SERM that is effective in treating hormone-responsive breast cancer, it acts as an antagonist to prevent receptor activation by endogenous oestrogen. As agonist of the endometrial receptors it promotes endometrial hyperplasia and hence increases the risk of endometrial cancer.
-
This question is part of the following fields:
- Pharmacology
-
-
Question 58
Correct
-
Stages of labour
Your Answer: The third stage ends with the delivery of the placenta and membranes
Explanation:First stage: The latent phase is generally defined as beginning at the point at which the woman perceives regular uterine contractions. A definition of active labour in a British journal was having contractions more frequent than every 5 minutes, in addition to either a cervical dilation of 3 cm or more or a cervical effacement of 80% or more.
Second stage: fetal expulsion begins when the cervix is fully dilated, and ends when the baby is born.
Third stage: placenta delivery – The period from just after the foetus is expelled until just after the placenta is expelled is called the third stage of labour or the involution stage.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 59
Correct
-
In twin deliveries: Which is true?
Your Answer: There is increased risk of postpartum haemorrhage
Explanation:Twin gestations are at increased risk for postpartum haemorrhage (PPH). A number of maternal and peripartum factors are associated with PPH requiring blood transfusion in twin gestations. Reducing the rate of caesarean delivery in twin pregnancies may decrease maternal hemorrhagic morbidity.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 60
Incorrect
-
Which of the following ultrasound findings form part of the Rotterdam criteria for diagnosis of PCOS (Polycystic Ovary Syndrome) ?
Your Answer: 10 or more peripheral ovarian follicles
Correct Answer: Increased ovarian volume >10cm3
Explanation:The Rotterdam criteria for the diagnosis of PCOS is based on a score of two out of the three criteria:
1) Oligo or anovulation
2) Hyperandrogenism – clinical (hirsutism or less commonly male pattern alopecia) or biochemical (raised FAI or free testosterone)
3) on ultrasound – contain 12 or more follicles measuring 2 to 9 mm in diameter and/or have an increased volume of 10 cm3 or greater. -
This question is part of the following fields:
- Clinical Management
-
-
Question 61
Correct
-
What percentage of pregnant women have asymptomatic vaginal colonisation with candida?
Your Answer: 40%
Explanation:Vulvovaginal candidiasis is the most common genital infections and it is caused by candida albicans in 80-92% of the cases. It colonise the vaginal flora in 20% of non pregnant and 40% pregnant women.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 62
Correct
-
A 24 year old lady is rushed to the emergency department complaining of vaginal spotting and abdominal cramping. Her 6 week pregnancy was confirmed by ultrasound scan last week. On speculum examination, the cervical os is open with blood noted around it. Which of the following is the most likely diagnosis?
Your Answer: Inevitable Miscarriage
Explanation:A miscarriage is defined as the spontaneous loss of a pregnancy before the age of viability at 24 weeks in the UK. An inevitable miscarriage occurs with the usual symptoms of a miscarriage such as menstrual-like cramping, vaginal bleeding and a dilated cervix. The gestational sac has ruptured but products of conception have not been passed. The products of conception will eventually pass.
A missed miscarriage is described as a loss of pregnancy without vaginal bleeding, loss of tissue, cervical changes or abdominal pain. During a scan, a fetal heartbeat is not observed, and the gestational sac may be small.
A threatened miscarriage is when the cervix dilates and uterine bleeding is seen; the pregnancy could still be viable.
A complete miscarriage occurs when all the products of conception are expelled from the uterus, bleeding has stopped, and the cervix has closed up after dilation. Recurrent miscarriages are described as spontaneous pregnancy loss of more than 2 to 3 consecutive times.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 63
Correct
-
A 30-year-old G2P1 woman presented to the maternity unit, in labour at 38 weeks gestation. During her previous pregnancy she delivered a healthy baby through caesarean section. The current pregnancy had been uneventful without any remarkable problems in antenatal visits except for the first trimester nausea and vomiting. On arrival, she had a cervical dilation of 4 cm and the fetal head was at -1 station. After 5 hours, the cervical length and fetal head station are still the same despite regular uterine contractions. Suddenly, there is a sudden gush of blood, which is approximately 1000 ml and the fetal heart rate have dropped to 80 bpm on CTG. Which of the following could be the most likely cause for this presentation?
Your Answer: Ruptured uterus
Explanation:Due to the previous history of caesarean section, uterine rupture would be the most likely cause of bleeding in this patient who is at a prolonged active phase of first stage of labour.
Maternal manifestations of uterine rupture are highly variable but some of its common features includes:
– Constant abdominal pain, where the pain may not be present in sufficient amount, character, or location suggestive of uterine rupture and may be masked partially or completely by use of regional analgesia.
– Signs of intra abdominal hemorrhage is a strong indication. Although hemorrhage is common feature, but signs and symptoms of intra-abdominal bleeding in cases of uterine rupture especially in those cases not associated with prior surgery may be subtle.
– Vaginal bleeding is not considered as a cardinal symptom as it may be modest, despite major intra-abdominal hemorrhage.
– Maternal tachycardia and hypotension
– Cessation of uterine contractions
– Loss of station of the fetal presenting part
– Uterine tenderness
As seen in this case, fetal bradycardia is the most common and characteristic clinical manifestation of uterine rupture, preceded by variable or late decelerations, but there is no other fetal heart rate pattern pathognomonic of rupture. Furthermore, fetal heart rate changes alone have a low sensitivity and specificity for diagnosing a case as uterine rupture.
Pain and persistent vaginal bleeding despite the use of uterotonic agents are characteristic for postpartum uterine rupture. If the rupture extends into the bladder hematuria may also occur.
A definite diagnosis of uterine rupture can be made only after laparotomy. Immediate cesarean section should be performed to save both the mother and the baby in cases where uterine rupture is suspected. -
This question is part of the following fields:
- Obstetrics
-
-
Question 64
Correct
-
Which of the following procedures allow the earliest retrieval of DNA for prenatal diagnosis in pregnancy:
Your Answer: Chorionic Villi Sampling (CVS)
Explanation:CVS has decreased in frequency with the recent increased uptake of cell-free DNA screening. It remains the only diagnostic test available in the first trimester and allows for diagnostic analyses, including fluorescence in situ hybridization (FISH), karyotype, microarray, molecular testing, and gene sequencing. CVS is performed between 10 and 14 weeks’ gestation. CVS has been performed before 9 weeks in the past, though this has shown to increase the risk of limb deformities and, therefore, is no longer recommended.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 65
Correct
-
A 28 year old women is seen in the early pregnancy unit. She has had a positive pregnancy test but is uncertain of her LMP. Ultrasound doesn't visualise a pregnancy. You perform bHCG tests 48 hours apart. The first bHCG is 400mIU/ml. The second is 190mIU/ml. What is the likely diagnosis
Your Answer: Non-viable pregnancy
Explanation:B-HCG levels almost double every 48 hours. A B-HCG levels of less than 5 mIU/ml is considered negative and anything above 25 is considered positive. As the foetus was not visualized on ultrasound in the uterus, there is possibility that this might be an ectopic pregnancy. But since the B-HCG levels also continued to fall the pregnancy becomes non-viable.
-
This question is part of the following fields:
- Biochemistry
-
-
Question 66
Correct
-
A 32-year-old woman visited your clinic at her 30th week of gestation, complaining of left lower limb pain. The doppler ultrasound findings had confirmed proximal deep vein thrombosis and she was treated with low molecular weight heparin. Now she is at her 34 weeks of gestation, and is expecting delivery in next four weeks. What would be your advice for her today?
Your Answer: Low molecular weight heparin should be switched to unfractionated heparin
Explanation:This patient has developed deep vein thrombosis during pregnancy and required anti-coagulation as part of treatment for up to 3-6 months. Enoxaparin, which is a low molecular weight heparin, is preferred over heparin due to the once or twice a day therapeutic dosing. Also monitoring of aPTT is not required in this case.
There is an association between Enoxaparin and an increased risk for epidural hematoma in women receiving epidural anaesthesia during labour. Considering that the patient mentioned is expected to go for delivery in 4 weeks and the possibility of her needing an epidural anaesthesia or general anaesthesia in case of undergoing a cesarean section, enoxaparin should be switched to unfractionated heparin, four weeks prior to the anticipated delivery. This is because of the fact that heparin can be antidoted with protamine sulphate.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 67
Incorrect
-
A 31-year-old woman's blood results after having secondary amenorrhoea that lasted for 6 months are: Testosterone = 3.4 nmol/L (<1.6), Oestradiol = 144 pmol/L (100-500), LH = 12 U/L and FSH = 4 U/L. What sign or symptom is she likely to have?
Your Answer: Hirsutism
Correct Answer:
Explanation:Biochemical features suggest that this patient has polycystic ovary syndrome (PCOS). It is associated with signs and symptoms of hyperandrogenism (oligomenorrhea, irregular menstruation, hirsutism, hair loss, and acne) and elevated testosterone. PCOS patients are often overweight or obese, have insulin resistance (treated with Metformin) and an adverse risk profile for cardiovascular disease.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 68
Correct
-
A 29 year old female presented at her 38th week of gestation to the ER with severe hypertension (210/100) and proteinuria (+++). Soon after admission, she developed generalized tonic clonic fits. What is the first line of management in this case?
Your Answer: Magnesium sulphate IV
Explanation:Magnesium Sulphate is the drug of choice in eclamptic patients. A loading dose of 4g magnesium sulphate in 100mL 0.9% saline IVI over 5min followed by maintenance IVI of 1g/h for 24h. Signs of toxicity include respiratory depression and jerky tendon reflexes. In recurrent fits additional 2g can be given. Magnesium should be stopped when the respiratory rate is <14/min, absent tendon reflexes, or urine output is <20mL/h.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 69
Correct
-
Looking at the picture below what is the diagnosis?
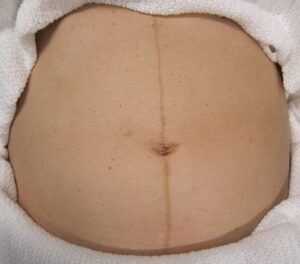
Your Answer: Linea Nigra
Explanation:This is Linea Nigra. It occurs in 3/4 of pregnancies and is due to increased melanocyte-stimulating hormone production by the placenta. This also causes melasma and darkening of the nipples.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 70
Incorrect
-
A 29 year old female who is 32 weeks pregnant, has been admitted to hospital with very severe hypertension. This is her second pregnancy. In the United Kingdom, what is the first line of treatment for hypertension whilst pregnant?
Your Answer: Labetalol
Correct Answer:
Explanation:Atenolol is considered teratogenic and has two main risks: fetal bradycardia and neonatal apnoea. ACE inhibitors and angiotensin II receptor blockers are also known to be teratogenic (even though large-scale studies are difficult to conduct during pregnancies).
-
This question is part of the following fields:
- Obstetrics
-
-
Question 71
Correct
-
A 30-year-old female is being investigated for subfertility. At what day of her menstrual cycle should blood be collected for progesterone, if she has a regular 28-day menstrual cycle?
Your Answer: Day 21
Explanation:Maximum levels of progesterone are detected at day 21 of 28 days in the menstrual cycle, assuming that ovulation has occurred at day 14. A value of >30nmol/l indicates an ovulatory cycle.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 72
Correct
-
A pregnant patient who is needle phobic has her nuchal translucency (NT) scan but refuses serum markers. You advise her the False Positive Rate of the scan is 5%. What would you advise the mother regarding the detection rate of Down Syndrome using NT alone?
Your Answer: 70%
Explanation:The nuchal lucency measurement is the measure of the nuchal pad thickness. Children with down syndrome have an increased thickness of the nuchal pad. The risk of down’s syndrome increases with maternal age. The nuchal lucency test has an accuracy rate of 70%.
-
This question is part of the following fields:
- Genetics
-
-
Question 73
Incorrect
-
Patients with high risk pregnancy should have a:
Your Answer: Follow-up in ANC every 6 weeks
Correct Answer: Fetal biophysical profile
Explanation:The BPP is performed in an effort to identify babies that may be at risk of poor pregnancy outcome, so that additional assessments of wellbeing may be performed, or labour may be induced or a caesarean section performed to expedite birth.
-
This question is part of the following fields:
- Biophysics
-
-
Question 74
Correct
-
A patient is being discharged following a termination of pregnancy at 14 weeks. She had been taking a combined oral contraceptive pill in the past but stopped taking this 6 months prior to falling pregnant as she wasn't in a serious relationship. When should she start again?
Your Answer: Start immediately
Explanation:Following an abortion or miscarriage, combined oral contraceptive pills should be started immediately.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 75
Incorrect
-
Which of the following changes would you expect in pregnancy?
Your Answer: Increased TSH Decreased Total T3 and T4
Correct Answer: Decreased TSH Increased Total T3 and T4
Explanation:Human chorionic gonadotrophin (hCG) has thyrotrophic activity owing to subunit homology with thyroid-stimulating hormone (TSH) and maternal TSH production is suppressed during the first trimester of pregnancy, when hCG levels are highest. The TSH response to thyrotrophin-releasing hormone (TRH) is reduced during the first trimester but returns to normal after this. Thyroid binding globulin increases in the first 2 weeks of pregnancy and reaches a plateau by 20 weeks. This leads to increased production of total T3 (tri-iodothyronine) and T4 (thyroxine).
-
This question is part of the following fields:
- Endocrinology
-
-
Question 76
Correct
-
A 53-year-old lady had mild vaginal bleeding for the previous 18 hours following sexual engagement. It's been a year since she had her last menstrual cycle. Her previous cervical screening test was 12 months ago, and everything came back normal. For the past year, she had not engaged in any sexual activity. She wasn't on any hormone replacement treatment at the time. Which of the following is the most likely cause of her symptoms?
Your Answer: Atrophic vaginitis
Explanation:Postmenopausal haemorrhage has started in this patient. Menopause is defined as the permanent cessation of menstruation and fertility that occurs 12 months after the previous menstrual period.
Atrophic vaginitis caused by oestrogen insufficiency is the most likely reason for this woman’s postmenopausal haemorrhage. It can also induce vaginal dryness and soreness during sexual intercourse.
Endometrial hyperplasia is unlikely to develop without hormone replacement therapy or oestrogen stimulation of the endometrium.
Similarly, endometrial cancer is a less likely cause of this patient’s post-menopausal bleeding.
A year ago, this woman received a normal cervical screening test. Cervical cancer is extremely unlikely to occur. After 12 months of no oestrogen, it’s also unlikely that you’ll have any irregular periods.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 77
Correct
-
A 35-year-old female went to a contraception clinic because she does not want to conceive for the next 2 years. She also has a history of heavy menstrual bleeding and pelvic pain. Imaging revealed fibroids. What is the best method of contraception for the patient in this case?
Your Answer: IUS
Explanation:IUS or Intra Uterine System/Device releases progestin. The progestin thickens the cervix, preventing the sperm from penetrating the cervix, and it also causes the uterine lining to become thinner, preventing any implantation. IUS may also prevent excessive bleeding and can help women with fibroids.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 78
Correct
-
A 21-year-old woman at 39 weeks of gestation in her second pregnancy is admitted in the hospital for severe abdominal pain. She notes that also has been having vaginal bleeding of about one litre and uterine contractions are present. Her previous pregnancy was a vaginal, without any complications. Her current blood pressure is 95/50 mmHg with a pulse rate of 120 beats/min. On physical examination, the uterus is palpable at the level of the xiphisternum and is firm. It is acutely tender to palpation. Fetal heart sounds cannot be heard on auscultation or with Doppler assessment. The cervix is 4 cm dilated and fully effaced. Immediate resuscitative measures are taken. Which of the following is the most appropriate next step in management for this patient?
Your Answer: Amniotomy
Explanation:This patient is presenting with a severe placental abruption causing fetal death and shock in the mother. The most appropriate initial management for the patient is to treat her shock with blood transfusions and exclude or treat any coagulation disorder resulting from the abruption. Delivery also needs to be expedited to remove the dead foetus. An amniotomy is usually all that is required to induce spontaneous labour as the uterus is usually very irritable. Spontaneous labour is likely to occur in this case, where the cervix is already 4 cm dilated and fully effaced.
Caesarean section is rarely needed to be done when the foetus is already dead.
Vaginal prostaglandin and an oxytocin (Syntocin®) infusion are not needed and unlikely to be required.
Ultrasound examination to confirm the diagnosis and fetal death is also unnecessary given the clinical and Doppler findings.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 79
Correct
-
Which of the following hormones are required for alveolar morphogenesis during pregnancy?
Your Answer: Progesterone, Prolactin and hPL
Explanation:The changes seen in breast tissue with the menstrual cycle are accentuated during pregnancy. Deposition of fat around glandular tissue occurs, and the number of glandular ducts is increased by oestrogen, while progesterone and human placental lactogen (hPL) increase the number of gland alveoli. Prolactin is essential for the stimulation of milk secretion and during pregnancy prepares the alveoli for milk production. Although prolactin concentration increases throughout pregnancy, it does not then result in lactation since it is antagonized at an alveolar receptor level by oestrogen.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 80
Correct
-
On the sixth day of her menstrual cycle, a 25-year-old lady comes to your clinic with slight lower abdomen pain. She has no children and lives with her male companion. Her blood pressure is 110/70 mmHg, her pulse is 90 beats per minute, and her temperature is 37.5°C. On vaginal examination, no adnexal lump is palpated, however cervical motion pain is noticed. Which of the following is the most appropriate next step in management?
Your Answer: Cervical swabs for culture
Explanation:Pain upon movement of the cervix with the health care provider’s gloved fingers is suggestive of an inflammatory process of the pelvic organs. CMT, when present, is classically found on bimanual examination of the cervix and uterus. While CMT is often associated with pelvic inflammatory disease, it can be present in other disease entities such as ectopic pregnancy, endometriosis, ovarian torsion, appendicitis, and perforated abdominal viscus.
PID is not a singular disease entity but describes a spectrum of disease. It is an upper genital tract infection, which may affect the uterus, fallopian tubes, ovaries, and peritoneum. PID can begin as cervicitis, progress to endometritis, followed by involvement of the fallopian tubes as pyosalpinx, and ultimately involve the ovary as a tubo-ovarian abscess (TOA). The two most common causative pathogens are N. gonorrhoeae and C. trachomatis although the infection is often polymicrobial.
Documentation of infection with either of these two organisms must be done by cervical swabs for culture.
Transvaginal ultrasound or CT scan can be done to confirm diagnosis however the absence of findings in these investigations doesn’t rule out the possibility of PID.
Urinalysis can be done to exclude urinary tract infection, one of the possible differential diagnosis for PID.
Thyroid stimulating hormone has no role in the diagnosis of PID.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 81
Correct
-
In a pregnant lady with polyhydramnios, the cause could be:
Your Answer: Foetus with oesophageal-atresia
Explanation:An underlying disease is only found in 17 % of cases in mild polyhydramnios. In contrast, an underlying disease is detected in 91 % of cases in moderate to severe polyhydramnios. The literature lists the following potential aetiologies: fetal malformations and genetic anomalies (8–45 %), maternal diabetes mellitus (5–26 %), multiple pregnancies (8–10 %), fetal anaemia (1–11 %), other causes, e.g. viral infections, Bartter syndrome, neuromuscular disorders, maternal hypercalcemia. Viral infections which can lead to polyhydramnios include parvovirus B19, rubella, and cytomegalovirus. Other infections, e.g. toxoplasmosis and syphilis, can also cause polyhydramnios.
-
This question is part of the following fields:
- Physiology
-
-
Question 82
Incorrect
-
Aromatase is key to Oestradiol production in the ovaries. Which of the following statements is true?
Your Answer: LH induces the theca cells to make aromatase
Correct Answer: FSH induces the granulosa cells to make aromatase
Explanation:The two main cell types of the ovaries:
1. The theca cells produce androgen in the form of androstenedione. The theca cells are not able to convert androgen to oestradiol themselves. The produced androgen is therefore taken up by granulosa cells.
2. The neighbouring granulosa cells then convert the androgen into oestradiol under the enzymatic action of aromatase FSH induces the granulosa cells to produce aromatase for this purpose -
This question is part of the following fields:
- Endocrinology
-
-
Question 83
Correct
-
The arterial blood supply to the bladder is via branches of which artery?
Your Answer: Internal Iliac
Explanation:The bladder is supplied by branches of the internal iliac artery, including the superior vesical artery, branches of the gluteal and obturator arteries and the inferior vesical artery in males and the vaginal and the uterine arteries in females.
-
This question is part of the following fields:
- Anatomy
-
-
Question 84
Correct
-
You are called to assist in an initially midwife led delivery. Upon delivering a female baby you notice the baby has partial fusion of the labioscrotal folds. You suspect congenital adrenal hyperplasia. Which of the following genes is most likely to be mutated?
Your Answer: CYP21A
Explanation:CAH leads to virilization of the female foetus. It occurs to an enzyme deficiency (21-hydroxylase). This results in a reduced levels of corticosteroids from being circulated resulting in hyperplasia of the adrenal glands and increased progesterone production. The CYP21A gene has been implicated in causes this deficiency.
-
This question is part of the following fields:
- Genetics
-
-
Question 85
Incorrect
-
A 42 year old smoker attends clinic due to vulval soreness and shows you a number of vulval lumps. Biopsy is taken and reported as showing
Your Answer: Lichen Simplex
Correct Answer: Vulval intraepithelial neoplasia (VIN)
Explanation:This is VIN. Smoking is a risk factor. It is also more common in immunocompromised patients.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 86
Correct
-
Lactogenesis at term is stimulated by which hormone?
Your Answer: Prolactin
Explanation:Prolactin is the hormone that is responsible for the production of milk (Lactogenesis). Oxytocin is responsible for the let down reflex during suckling.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 87
Correct
-
Endometrial ablation is a medical technique that removes or destroys the endometrial lining in women who have severe monthly flow. Endometrial ablation is not contraindicated by which of the following?
Your Answer: Completed family
Explanation:Endometrial ablation is primarily intended to treat premenopausal women with heavy menstrual bleeding (HMB) who do not desire future fertility. Women who choose endometrial ablation often have failed or declined medical management.
Absolute contraindications to endometrial ablation include pregnancy, known or suspected endometrial hyperplasia or cancer, desire for future fertility, active pelvic infection, IUD currently in situ, and being post-menopausal. In general, endometrial ablation should be avoided in patients with congenital uterine anomalies, severe myometrial thinning, and uterine cavity lengths that exceed the capacity of the ablative technique (usually greater than 10-12 cm).
-
This question is part of the following fields:
- Gynaecology
-
-
Question 88
Correct
-
You are called to review a baby with cyanosis when feeding immediately after birth. Subsequent investigation and imaging reveals choanal atresia. Upon questioning the mother reveals she had been getting repeat prescriptions from her GP in Poland without her UK GPs' or your knowledge. Which of the following medication was most likely to cause this?
Your Answer: Carbimazole
Explanation:This is one of the defects attributable to Carbimazole use.
-
This question is part of the following fields:
- Pharmacology
-
-
Question 89
Incorrect
-
Normally, pregnancy in 2nd trimester is characterized by all of the following, EXCEPT:
Your Answer: Decreased fasting plasma glucose
Correct Answer: Elevated fasting plasma glucose
Explanation:Elevated fasting plasma glucose means gestational diabetes mellitus and is not considered to be in the spectrum of a normal pregnancy. In normal pregnancy however, maternal tissues become progressively insensitive to insulin. This is believed to be caused partly by hormones from the placenta and partly by other obesity and pregnancy related factors that are not fully understood. Gestational diabetes mellitus (GDM) occurs in about 5% of pregnancies but figures vary considerably depending upon the criteria used and demographic characteristics of the population.
-
This question is part of the following fields:
- Physiology
-
-
Question 90
Correct
-
Regarding gestational diabetes which of the following is NOT a recognised risk factor
Your Answer: High polyunsaturated fat intake
Explanation:Gestational diabetes (GDM) occurs in 2–9 per cent of all pregnancies. Screening for diabetes in pregnancy can be justify ed to diagnose previously unrecognized cases of pre-existing diabetes and to identify a group of women who are at risk of developing NIDDM later in life. No single screening test has been shown to be perfect in terms of high sensitivity and specific city for gestational diabetes. Urinary glucose is unreliable, and most screening tests now rely on blood glucose estimation, with an oral glucose tolerance test commonly used. The aim of glucose control is to keep fasting levels between 3.5 and 5.5 mmol/L and postprandial levels 7.1 mmol/L, with insulin treatment usually indicated outside these ranges. There are various risk factors for gestational diabetes including increasing age, ethnicity, previous still births etc.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 91
Correct
-
The number of chromosomes in the human somatic cell is:
Your Answer: 46
Explanation:In eukaryotes, the genome comprises several double-stranded, linear DNA molecules bound with proteins to form complexes called chromosomes. Each species of eukaryote has a characteristic number of chromosomes in the nuclei of its cells. Human body cells (somatic cells) have 46 chromosomes.
-
This question is part of the following fields:
- Cell Biology
-
-
Question 92
Correct
-
A 26-year-old woman with irregular menstrual cycle has a positive pregnancy test. She wants to know the age of her baby. Which of the following methods is considered the most accurate for estimating gestational age?
Your Answer: Transvaginal ultrasound at 8 weeks
Explanation:Ultrasound has emerged as the more accurate method of assessing fetal gestational age, especially in the first trimester. Both transvaginal and transabdominal probe assessments are used to obtain a more accurate measurement of gestational age. Transvaginal is more helpful in first trimester pregnancies.
A transvaginal ultrasound exam should not be performed in a pregnant patient with vaginal bleeding and known placenta previa, a pregnant patient with premature rupture of membranes, and a patient who refuses exam despite informed discussion.
Sonographic assessment within the first 13 weeks and 6 days will provide the most accurate estimate of gestational age. Both transvaginal and transabdominal approaches may be used. However, the transvaginal approach may provide a more clear and accurate view of early embryonic structures. Although the gestational sac and yolk sac are the first measurable markers visible on ultrasound, these poorly correlate with gestational age.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 93
Correct
-
A 28-year-old woman who recently got married presents to your clinic. She has a history of extremely irregular menstrual cycles with the duration varying between four and ten weeks. She had attended her routine review appointment one week prior to her current presentation. At that time she had stated that her last period had occurred six weeks previously. You had recommended the following tests for which the results are as shown below: Serum follicle-stimulating hormone (FSH): 3 IU/L (<13), Serum luteinising hormone (LH): *850 IU/L (4-10 in follicular phase, 20-100 at mid-cycle), Serum prolactin (PRL): 475 mU/L (50-500). Which one of the following is the most probable reason for her amenorrhoea?
Your Answer: Early pregnancy.
Explanation:All of the options provided could cause amenorrhoea and therefore need to be evaluated.
The luteinising hormone (LH) level reported here is exceedingly elevated. A patient with polycystic ovarian syndrome (PCOS) is unlikely to have such a raised level, but it could be because of a LH-producing adenoma. Such tumours are, however, extremely rare.
Early pregnancy (correct answer) is the most likely cause of this woman’s elevated LH level. This would be due to the presence of beta human chorionic gonadotropin (hCG) hormone that is produced during pregnancy.
LH and beta-HCG both have similar beta-subunits and cross-reactions are commonly noted in LH assays.
The serum prolactin (PRL) level is at the upper end of the normal range and this correlates to the levels observed in the early stages of pregnancy.
The follicle-stimulating hormone (FSH) levels remain low during early pregnancy.
If her amenorrhea had been caused by stress from her recent marriage, the LH level would have been normal or low.
If the cause was premature ovarian failure, the FSH level would have been significantly higher.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 94
Correct
-
You see a 23 year old women in clinic complaining of vaginal discharge. The lab phone to tell you microscopy and staining shows a gram negative diplococcus. Which organism is most likely to be responsible?
Your Answer: Neisseria gonorrhoeae
Explanation:The most common gram negative diplococci include Neisseria, haemophilus and Moraxella.
-
This question is part of the following fields:
- Microbiology
-
-
Question 95
Correct
-
Which of the following is known to increase the risk of endometrial cancer?
Your Answer: PCOS
Explanation:The risk factors of endometrial cancer include obesity, diabetes, late menopause, unopposed oestrogen therapy, tamoxifen therapy, HRT and a family history of colorectal and ovarian carcinoma.
-
This question is part of the following fields:
- Epidemiology
-
-
Question 96
Correct
-
A 33-year-old female, who is 14 weeks pregnant, presented to your office for antenatal follow-up. On examination, the fundal height is found to be18 cm. which among the following would be the best next step in the management of this patient?
Your Answer: Perform an ultrasound scan
Explanation:At 12 weeks gestation the fundus is expected to be palpable above the pubis symphysis and it is expected to be felt at the level of umbilicus by 20 weeks. Though the uterine fundus stands in between from 12 and 20 weeks, the height of the fundus in centimeters is equivalent to the weeks of pregnancy after 20 weeks.
For 14-week pregnant uterus a fundal height of 18cm is definitely large and dating errors is considered as the most common cause for such a discrepancy. Hence, it is better to perform an ultrasound scan for more accurately estimating the gestational age. Also if the case is not a simple dating error, ultrasonography can provide definitive additional information about other possible conditions such as polyhydramnios, multiple gestation, etc that might have led to a large-for-date uterus.
A large-for-gestational-age uterus are most commonly found in conditions like:
– Dating errors which is the most common cause
– Twin pregnancy
– Gestational diabetes
– Polyhydramnios
– Gestational trophoblastic disease, also known as molar pregnancy -
This question is part of the following fields:
- Obstetrics
-
-
Question 97
Correct
-
A 28 year old woman presents for a scan at 13 weeks. Though this is her second pregnancy, the first ended in a 1st trimester miscarriage. She has not reported any problems with the current pregnancy. The ultrasound scan showed a small gestational sac and no fetal cardiac activity. Which of the following is the most likely diagnosis?
Your Answer: Missed Miscarriage
Explanation:A miscarriage is defined as the spontaneous loss of a pregnancy before the age of viability at 24 weeks in the UK.
A missed miscarriage is described as a loss of pregnancy without vaginal bleeding, loss of tissue, cervical changes or abdominal pain. During a scan, a fetal heartbeat is not observed, and the gestational sac may be small.
A threatened miscarriage is when the cervix dilates and uterine bleeding is seen; the pregnancy could still be viable. A complete miscarriage occurs when all the products of conception are expelled from the uterus, bleeding has stopped, and the cervix has closed up after dilation.
An inevitable miscarriage occurs with the usual symptoms of a miscarriage and a dilated cervix, suggesting that the passage of the fetal tissue is inevitable.
Recurrent miscarriages are described as spontaneous pregnancy loss of more than 2 to 3 consecutive times.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 98
Correct
-
A 66-year-old lady comes to your clinic complaining of a brownish vaginal discharge that has been bothering her for the previous three months. Atrophic vagina is seen on inspection. Which of the following diagnoses is the most likely?
Your Answer: Vaginal atrophy
Explanation:Endometrial cancer should always be the first diagnosis to rule out in a 65-year-old lady with brownish vaginal discharge. The inquiry focuses on the most likely source of the symptoms, rather than the most significant diagnosis to explore.
Blood typically causes the dark hue of vaginal discharge. The uterine cavity or the vagina can both be the source of bleeding. Only 5-10% of postmenopausal women with vaginal bleeding were found to have endometrial cancer. Around 60% of the women had atrophic vaginitis.Urogenital atrophy is caused by oestrogen insufficiency in postmenopausal women. Urogenital atrophy can cause the following symptoms:
– Dry vaginal skin
– Vaginal inflammation or burning
– Vaginal lubrication is reduced during sexual activity.
– Vulvar or vaginal pain, as well as dyspareunia (at the introitus or within the vagina)
– Vaginal or vulvar bleeding (e.g. postcoital bleeding. fissures)
– Vaginal discharge from the cervix (leukorrhea or yellow and malodorous)
– A vaginal bulge or pelvic pressure
– Symptoms of the urinary tract (e.g. urinary frequency, dysuria, urethral discomfort, haematuria). -
This question is part of the following fields:
- Gynaecology
-
-
Question 99
Correct
-
You review a patient in the fertility clinic. The ultrasound and biochemical profile are consistent with PCOS. She has been trying to conceive for 2 years. Her BMI is 26 kg/m2. She is a non-smoker. You plan to initiate Clomiphene. According to NICE guidance how long should treatment continue for (assuming patient remains non-pregnant)?
Your Answer: 6 months
Explanation:Treatment with Clomiphene should not exceed 6 months.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 100
Correct
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)