-
Question 1
Incorrect
-
A 65-year-old man comes to the clinic complaining of lethargy. He denies any other systemic symptoms. During the physical examination, a non-pulsatile mass is palpated in the right lower quadrant of his abdomen, which does not move with respiration. Additionally, he has pale conjunctivae. What is the best course of action for management?
Your Answer: Ultrasound abdomen
Correct Answer: Urgent referral to local colorectal service
Explanation:The presence of an abdominal mass along with symptoms of lethargy and pallor may indicate the likelihood of colorectal cancer, which could also lead to anaemia.
Referral Guidelines for Colorectal Cancer
Colorectal cancer is a serious condition that requires prompt diagnosis and treatment. In 2015, the National Institute for Health and Care Excellence (NICE) updated their referral guidelines for patients suspected of having colorectal cancer. According to these guidelines, patients who are 40 years or older with unexplained weight loss and abdominal pain, 50 years or older with unexplained rectal bleeding, or 60 years or older with iron deficiency anemia or change in bowel habit should be referred urgently to colorectal services for investigation. Additionally, patients who test positive for occult blood in their feces should also be referred urgently.
An urgent referral should also be considered for patients who have a rectal or abdominal mass, unexplained anal mass or anal ulceration, or are under 50 years old with rectal bleeding and any of the following unexplained symptoms/findings: abdominal pain, change in bowel habit, weight loss, or iron deficiency anemia.
The NHS offers a national screening program for colorectal cancer, which involves sending eligible patients aged 60 to 74 years in England and 50 to 74 years in Scotland FIT tests through the post. FIT is a type of fecal occult blood test that uses antibodies to detect and quantify the amount of human blood in a single stool sample. Patients with abnormal results are offered a colonoscopy.
The FIT test is also recommended for patients with new symptoms who do not meet the 2-week criteria listed above. For example, patients who are 50 years or older with unexplained abdominal pain or weight loss, under 60 years old with changes in their bowel habit or iron deficiency anemia, or 60 years or older who have anemia even in the absence of iron deficiency. Early detection and treatment of colorectal cancer can significantly improve patient outcomes, making it important to follow these referral guidelines.
-
This question is part of the following fields:
- Surgery
-
-
Question 2
Incorrect
-
A 35-year-old woman who is a heavy smoker presents with recurring infections in her right breast. During examination, an indurated area is found at the lateral aspect of the nipple areolar complex. Imaging reveals no mass lesions. What is the probable diagnosis?
Your Answer: Paget's disease of the nipple
Correct Answer: Periductal mastitis
Explanation:Recurrent infections are a common symptom of periductal mastitis in smokers, which can be treated with co-amoxiclav. Additionally, Mondor’s disease of the breast is characterized by a localized thrombophlebitis of a breast vein.
Understanding Mastitis: Inflammation of the Breast Tissue
Mastitis is a condition that refers to the inflammation of the breast tissue, which is commonly associated with breastfeeding. It affects around 1 in 10 women and is characterized by a painful, tender, and red hot breast. Other symptoms may include fever and general malaise.
The first-line management of mastitis is to continue breastfeeding, as simple measures such as analgesia and warm compresses can help alleviate the symptoms. However, if the patient is systemically unwell, has a nipple fissure, or if symptoms do not improve after 12-24 hours of effective milk removal, treatment with antibiotics may be necessary. The first-line antibiotic for mastitis is oral flucloxacillin, which should be taken for 10-14 days. This reflects the fact that the most common organism causing infective mastitis is Staphylococcus aureus.
It is important to note that breastfeeding or expressing should continue during antibiotic treatment. If left untreated, mastitis may develop into a breast abscess, which generally requires incision and drainage. Therefore, it is crucial to seek medical attention if symptoms persist or worsen. Understanding mastitis and its management can help ensure the health and well-being of both the mother and the baby.
-
This question is part of the following fields:
- Surgery
-
-
Question 3
Incorrect
-
A 62-year-old man presents to the pre-admission clinic for assessment prior to an elective prostatectomy. You find no adverse past medical history and examination is unremarkable. An electrocardiogram (ECG) is indicated in all pre-operative patients undergoing major surgery who are over the age of 60. The ECG is shown below.
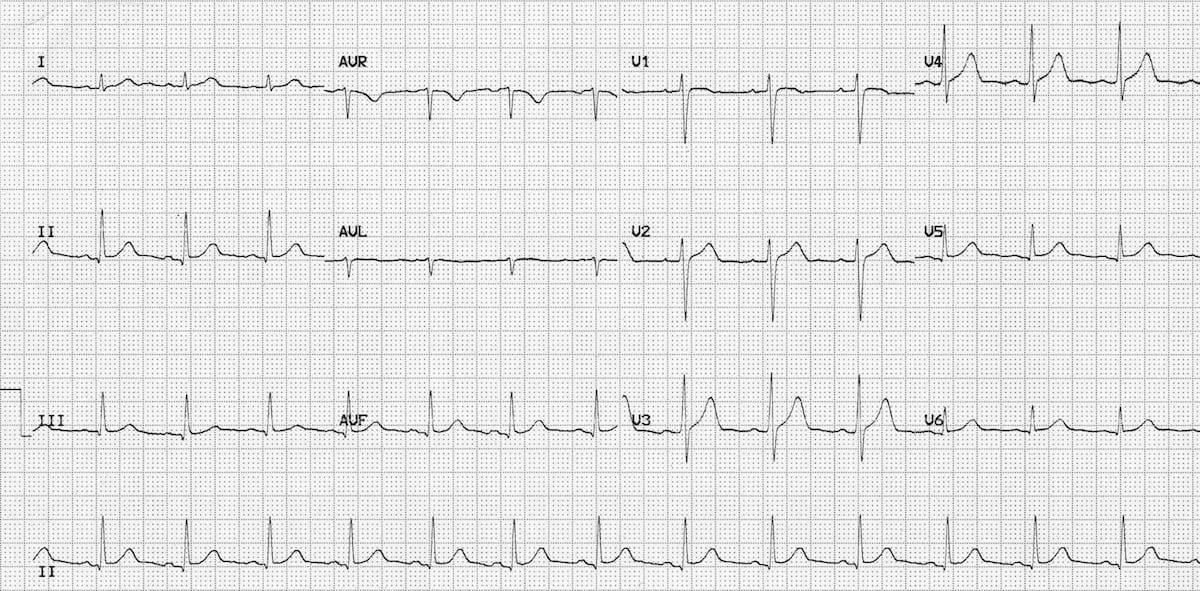 After having reviewed the ECG, what is the next best step to take with this patient?
After having reviewed the ECG, what is the next best step to take with this patient? Your Answer: Discuss the patient with the list anaesthetist
Correct Answer: No further assessment is required
Explanation:Assessing Cardiac Risk in Preoperative Patients: Common Misconceptions
There are several misconceptions when it comes to assessing cardiac risk in preoperative patients. One common mistake is assuming that all patients require extensive cardiac testing, even when there are no significant risk factors or symptoms present. For example, if a patient has no significant past medical history and their examination is unremarkable, an echocardiogram is not necessary.
On the other hand, some clinicians may be too cautious and cancel a patient’s procedure based on a perceived cardiac risk that is not supported by evidence. If the patient’s ECG is normal and there are no cardiac risk factors, cancelling the procedure would be unreasonable.
It is important to recognise that not all preoperative patients require extensive cardiac testing. Instead, clinicians should focus on identifying patients with specific cardiac conditions that require closer monitoring and management. By avoiding unnecessary testing and interventions, clinicians can improve patient outcomes and reduce healthcare costs.
-
This question is part of the following fields:
- Surgery
-
-
Question 4
Incorrect
-
A 70-year-old female presents to breast clinic following a left total mastectomy and sentinel lymph node biopsy for breast cancer. The histological analysis reveals complete excision of the tumour and clear malignancy in all 3 lymph nodes. The tumour is an invasive ductal carcinoma of grade 1, with ER and PR positivity and HER2 negativity. What additional treatment options should be considered for this patient?
Your Answer: Tamoxifen
Correct Answer: Anastrozole
Explanation:The recommended adjuvant hormonal therapy for postmenopausal women with ER+ breast cancer is anastrozole. This medication is an aromatase inhibitor that reduces estrogen levels in the body and is typically given for 5 years. Common side effects include hot flashes, insomnia, and low mood.
Axillary node clearance (ANC) is not necessary in this case since the lymph nodes sampled from the sentinel lymph node biopsy (SLNB) did not show any evidence of malignancy. ANC can increase the risk of lymphoedema, so it should only be performed if needed to clear disease.
Herceptin (trastuzumab) is a type of adjuvant therapy for breast cancer that is used for patients with HER2+ breast cancer. However, since the patient in this case had HER2 receptor status that was negative, Herceptin is not indicated.
Radiotherapy is also not necessary in this case since the patient had a total mastectomy, the lesion was completely removed, and no lymph nodes were involved. Therefore, radiotherapy would unlikely provide any benefit.
Breast cancer management varies depending on the stage of the cancer, type of tumor, and patient’s medical history. Treatment options may include surgery, radiotherapy, hormone therapy, biological therapy, and chemotherapy. Surgery is typically the first option for most patients, except for elderly patients with metastatic disease who may benefit more from hormonal therapy. Prior to surgery, an axillary ultrasound is recommended for patients without palpable axillary lymphadenopathy, while those with clinically palpable lymphadenopathy require axillary node clearance. The type of surgery offered depends on various factors, such as tumor size, location, and type. Breast reconstruction is also an option for patients who have undergone a mastectomy.
Radiotherapy is recommended after a wide-local excision to reduce the risk of recurrence, while mastectomy patients may receive radiotherapy for T3-T4 tumors or those with four or more positive axillary nodes. Hormonal therapy is offered if tumors are positive for hormone receptors, with tamoxifen being used in pre- and perimenopausal women and aromatase inhibitors like anastrozole in postmenopausal women. Tamoxifen may increase the risk of endometrial cancer, venous thromboembolism, and menopausal symptoms. Biological therapy, such as trastuzumab, is used for HER2-positive tumors but cannot be used in patients with a history of heart disorders. Chemotherapy may be used before or after surgery, depending on the stage of the tumor and the presence of axillary node disease. FEC-D is commonly used in the latter case.
-
This question is part of the following fields:
- Surgery
-
-
Question 5
Incorrect
-
A 45-year-old man with a history of alcohol abuse presents to your clinic after being diagnosed with chronic pancreatitis. You inform him that this diagnosis increases his likelihood of developing diabetes mellitus. What tests should you suggest to assess his risk for this condition?
Your Answer:
Correct Answer: Annual HbA1c
Explanation:Type 3c diabetes mellitus is a rare complication of pancreatitis that is more difficult to manage than type 1 or 2 diabetes mellitus due to the accompanying exocrine insufficiency, which leads to malabsorption and malnutrition. The development of diabetes mellitus may take years after the onset of pancreatitis, necessitating lifelong monitoring through annual HbA1c measurements. An ultrasound of the pancreas will not provide any indication of diabetes development. Additionally, it is crucial to counsel the patient on their alcohol misuse, as it may exacerbate their pancreatitis.
Understanding Chronic Pancreatitis
Chronic pancreatitis is a condition characterized by inflammation that can affect both the exocrine and endocrine functions of the pancreas. While alcohol excess is the leading cause of this condition, up to 20% of cases are unexplained. Other causes include genetic factors such as cystic fibrosis and haemochromatosis, as well as ductal obstruction due to tumors, stones, and structural abnormalities like pancreas divisum and annular pancreas.
Symptoms of chronic pancreatitis include pain that worsens 15 to 30 minutes after a meal, steatorrhoea, and diabetes mellitus. Abdominal x-rays can show pancreatic calcification in 30% of cases, while CT scans are more sensitive at detecting calcification with a sensitivity of 80% and specificity of 85%. Functional tests like faecal elastase may be used to assess exocrine function if imaging is inconclusive.
Management of chronic pancreatitis involves pancreatic enzyme supplements, analgesia, and antioxidants, although the evidence base for the latter is limited. It is important to understand the causes, symptoms, and management of chronic pancreatitis to effectively manage this condition.
-
This question is part of the following fields:
- Surgery
-
-
Question 6
Incorrect
-
Which of the following is not a diagnostic criteria for brain death?
Your Answer:
Correct Answer: No response to sound
Explanation:Criteria and Testing for Brain Stem Death
Brain death occurs when the brain and brain stem cease to function, resulting in irreversible loss of consciousness and vital functions. To determine brain stem death, certain criteria must be met and specific tests must be performed. The patient must be in a deep coma of known cause, with reversible causes excluded and no sedation. Electrolyte levels must be normal.
The testing for brain stem death involves several assessments. The pupils must be fixed and unresponsive to changes in light intensity. The corneal reflex must be absent, and there should be no response to supraorbital pressure. The oculovestibular reflexes must be absent, which is tested by injecting ice-cold water into each ear. There should be no cough reflex to bronchial stimulation or gagging response to pharyngeal stimulation. Finally, there should be no observed respiratory effort in response to disconnection from the ventilator for at least five minutes, with adequate oxygenation ensured.
It is important that the testing is performed by two experienced doctors on two separate occasions, with at least one being a consultant. Neither doctor can be a member of the transplant team if organ donation is being considered. These criteria and tests are crucial in determining brain stem death and ensuring that the patient is beyond recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 7
Incorrect
-
A 53-year-old man presents to the GUM clinic with a swollen, tender, and red glans penis that he has been experiencing for the past five days. He is unable to retract his foreskin fully and is experiencing pain while urinating. He has no sexual activity. This is his fourth presentation for balanitis in the last year, and he has tested negative for sexually transmitted infections and bacterial infections on each occasion. He has been successfully managed with saline baths and topical clotrimazole. He has a medical history of diabetes mellitus.
After treating this acute episode with saline baths and topical clotrimazole, what is the most appropriate next step in management?Your Answer:
Correct Answer: Refer for circumcision
Explanation:Circumcision is recommended for patients with recurrent balanitis.
Balanitis, which is characterized by inflammation of the glans penis, can be caused by various factors such as sexually transmitted infections, dermatitis, bacterial infections, and opportunistic fungal infections like Candida. In this case, the patient’s diabetes is likely the underlying cause of the fungal infection. Acute infections are typically treated with saline baths and addressing the root cause. Topical treatments are also recommended, depending on the cause of the infection. However, for patients with recurrent balanitis, circumcision is the most appropriate course of action to prevent future occurrences.
Understanding Circumcision
Circumcision is a practice that has been carried out in various cultures for centuries. Today, it is mainly practiced by people of the Jewish and Islamic faith for religious or cultural reasons. However, it is important to note that circumcision for these reasons is not available on the NHS.
The medical benefits of circumcision are still a topic of debate. However, some studies have shown that it can reduce the risk of penile cancer, urinary tract infections, and sexually transmitted infections, including HIV.
There are also medical indications for circumcision, such as phimosis, recurrent balanitis, balanitis xerotica obliterans, and paraphimosis. It is crucial to rule out hypospadias before performing circumcision as the foreskin may be needed for surgical repair.
Circumcision can be performed under local or general anesthesia. It is a personal decision that should be made after careful consideration of the potential benefits and risks.
-
This question is part of the following fields:
- Surgery
-
-
Question 8
Incorrect
-
A 50-year-old man experiences polytrauma and necessitates a massive transfusion of packed red cells and fresh frozen plasma. After three hours, he presents with significant hypoxia and a CVP reading of 5 mmHg. A chest x-ray reveals diffuse pulmonary infiltrates in both lungs. What is the probable diagnosis?
Your Answer:
Correct Answer: Transfusion associated lung injury
Explanation:Plasma components pose the highest risk for transfusion associated lung injury.
When plasma components are infused, there is a possibility of transfusion lung injury. This can cause damage to the microvasculature in the lungs, resulting in diffuse infiltrates visible on imaging. Unfortunately, mortality rates are often high in such cases. It is worth noting that a normal central venous pressure (which should be between 0-6 mmHg) is not necessarily indicative of fluid overload.
Understanding Massive Haemorrhage and its Complications
Massive haemorrhage is defined as the loss of one blood volume within 24 hours, the loss of 50% of the circulating blood volume within three hours, or a blood loss of 150ml/minute. In adults, the blood volume is approximately 7% of the total body weight, while in children, it is between 8 and 9% of their body weight.
Massive haemorrhage can lead to several complications, including hypothermia, hypocalcaemia, hyperkalaemia, delayed type transfusion reactions, transfusion-related lung injury, and coagulopathy. Hypothermia occurs because the blood is refrigerated, which impairs homeostasis and shifts the Bohr curve to the left. Hypocalcaemia may occur because both fresh frozen plasma (FFP) and platelets contain citrate anticoagulant, which may chelate calcium. Hyperkalaemia may also occur because the plasma of red cells stored for 4-5 weeks contains 5-10 mmol K+.
Delayed type transfusion reactions may occur due to minor incompatibility issues, especially if urgent or non-cross-matched blood is used. Transfusion-related lung injury is the leading cause of transfusion-related deaths and poses the greatest risk with plasma components. It occurs as a result of leucocyte antibodies in transfused plasma, leading to aggregation and degranulation of leucocytes in lung tissue. Finally, coagulopathy is anticipated once the circulating blood volume is transfused. One blood volume usually drops the platelet count to 100 or less, and it will both dilute and not replace clotting factors. The fibrinogen concentration halves per 0.75 blood volume transfused.
In summary, massive haemorrhage can lead to several complications that can be life-threatening. It is essential to understand these complications to manage them effectively and prevent adverse outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 9
Incorrect
-
A 50-year-old man presents to his GP with complaints of left flank pain. He has a history of smoking a pack of cigarettes a day for 25 years. On physical examination, there is tenderness in the left flank but no palpable mass. Urine dipstick testing reveals the presence of blood. A CT scan of the abdomen shows a complex cystic mass with solid and liquid components, arising from the parenchyma of the left kidney and with septations. What is the most probable diagnosis?
Your Answer:
Correct Answer: Renal cell carcinoma
Explanation:Clear cell carcinoma is the most frequent histological type of malignant renal cancer. The classic triad of renal cancer includes flank pain, mass, and haematuria, but it is unusual for all three symptoms to be present at the initial diagnosis. Clear cell carcinoma can be distinguished from a simple cyst by its variegated, septated interior. Transitional cell carcinomas are less common and typically originate from the ureter. Angiomyolipomas are also infrequent and are linked to tuberous sclerosis.
Understanding Renal Cell Cancer
Renal cell cancer, also known as hypernephroma, is a primary renal neoplasm that accounts for 85% of cases. It typically arises from the proximal renal tubular epithelium, with the clear cell subtype being the most common. This type of cancer is more prevalent in middle-aged men and is associated with smoking, von Hippel-Lindau syndrome, and tuberous sclerosis. While renal cell cancer is only slightly increased in patients with autosomal dominant polycystic kidney disease, it can present with a classical triad of haematuria, loin pain, and abdominal mass. Other features include pyrexia of unknown origin, endocrine effects, and paraneoplastic hepatic dysfunction syndrome.
The T category criteria for renal cell cancer are based on the size and extent of the tumour. For confined disease, a partial or total nephrectomy may be recommended depending on the tumour size. Patients with a T1 tumour are typically offered a partial nephrectomy, while those with larger tumours may require a total nephrectomy. Treatment options for renal cell cancer include alpha-interferon, interleukin-2, and receptor tyrosine kinase inhibitors such as sorafenib and sunitinib. These medications have been shown to reduce tumour size and treat patients with metastases. It is important to note that renal cell cancer can have paraneoplastic effects, such as Stauffer syndrome, which is associated with cholestasis and hepatosplenomegaly. Overall, early detection and prompt treatment are crucial for improving outcomes in patients with renal cell cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 10
Incorrect
-
A 45-year-old female patient complains of a painless lump in her right groin. She denies any changes in bowel habits or abdominal discomfort. Her medical history includes asthma and three previous vaginal deliveries. Upon examination, a soft swelling is palpable with a positive cough impulse. The lump is located inferolateral to the right pubic tubercle, fully reducible, and non-tender. Both femoral pulses are palpated separately and are normal. What is the best course of action for managing this patient's condition?
Your Answer:
Correct Answer: Refer to the surgical team for consideration of surgical repair
Explanation:Surgical referral for repair is necessary for femoral hernias, regardless of symptoms, due to the risk of strangulation. In this case, the patient’s history and examination suggest a hernia, potentially a femoral hernia, and surgical repair is necessary. The use of a support belt could increase the risk of strangulation, and a duplex scan, while a good idea, is not the most appropriate management for this patient. No action is unsafe, and antibiotics are not currently indicated.
Understanding Femoral Hernias
Femoral hernias occur when a part of the bowel or other abdominal organs pass through the femoral canal, which is a potential space in the anterior thigh. This can result in a lump in the groin area that is mildly painful and typically non-reducible. Femoral hernias are less common than inguinal hernias, accounting for only 5% of abdominal hernias, and are more prevalent in women, especially those who have had multiple pregnancies. Diagnosis is usually clinical, but ultrasound may be used to confirm the presence of a femoral hernia and exclude other possible causes of a lump in the groin area.
Complications of femoral hernias include incarceration, where the herniated tissue cannot be reduced, and strangulation, which is a surgical emergency. The risk of strangulation is higher with femoral hernias than with inguinal hernias and increases over time. Bowel obstruction and bowel ischaemia may also occur, leading to significant morbidity and mortality for the patient.
Surgical repair is necessary for femoral hernias, and it can be done laparoscopically or via a laparotomy. Hernia support belts or trusses should not be used for femoral hernias due to the risk of strangulation. In an emergency situation, a laparotomy may be the only option. It is essential to distinguish femoral hernias from inguinal hernias, as they have different locations and require different management approaches.
-
This question is part of the following fields:
- Surgery
-
-
Question 11
Incorrect
-
A 44-year-old man presents with symptoms of urinary colic. He has suffered from recurrent episodes of frank haematuria over the past few days. On examination he has a right loin mass and a varicocele. What is the most likely diagnosis?
Your Answer:
Correct Answer: Renal adenocarcinoma
Explanation:Renal Adenocarcinoma, also known as a Grawitz tumour, can present with symptoms such as haematuria and clot colic. It has the potential to metastasize to bone.
Renal Cell Carcinoma: Characteristics, Diagnosis, and Management
Renal cell carcinoma is a type of adenocarcinoma that develops in the renal cortex, specifically in the proximal convoluted tubule. It is a solid lesion that may be multifocal, calcified, or cystic. The tumor is usually surrounded by a pseudocapsule of compressed normal renal tissue. Spread of the tumor may occur through direct extension into the adrenal gland, renal vein, or surrounding fascia, or through the hematogenous route to the lung, bone, or brain. Renal cell carcinoma accounts for up to 85% of all renal malignancies, and it is more common in males and in patients in their sixth decade.
Patients with renal cell carcinoma may present with various symptoms, such as haematuria, loin pain, mass, or symptoms of metastasis. Diagnosis is usually made through multislice CT scanning, which can detect the presence of a renal mass and any evidence of distant disease. Biopsy is not recommended when a nephrectomy is planned, but it is mandatory before any ablative therapies are undertaken. Assessment of the functioning of the contralateral kidney is also important.
Management of renal cell carcinoma depends on the stage of the tumor. T1 lesions may be managed by partial nephrectomy, while T2 lesions and above require radical nephrectomy. Preoperative embolization and resection of uninvolved adrenal glands are not indicated. Patients with completely resected disease do not benefit from adjuvant therapy with chemotherapy or biological agents. Patients with transitional cell cancer will require a nephroureterectomy with disconnection of the ureter at the bladder.
-
This question is part of the following fields:
- Surgery
-
-
Question 12
Incorrect
-
A 42-year-old woman undergoes a gastric bypass surgery and visits the clinic with complaints of vertigo and crampy abdominal pain after meals. What could be the possible underlying cause?
Your Answer:
Correct Answer: Dumping syndrome
Explanation:Dumping syndrome is a possible consequence of gastric surgery, and it can be categorized as early or late. This condition arises when a hyperosmolar load enters the proximal jejunum too quickly. The process of osmosis causes water to be drawn into the lumen, leading to lumen distension and pain, followed by diarrhea. Additionally, excessive insulin is released, which can cause symptoms of hypoglycemia.
Understanding Post Gastrectomy Syndromes
Post gastrectomy syndromes can vary depending on whether a total or partial gastrectomy is performed. The type of reconstruction also plays a role in the functional outcomes. Roux en Y reconstruction is generally considered the best option. In cases where a gastrojejunostomy is performed following a distal gastrectomy, gastric emptying is improved if the jejunal limbs are tunneled in the retrocolic plane.
There are several post gastrectomy syndromes that patients may experience. These include small capacity, also known as early satiety, dumping syndrome, bile gastritis, afferent loop syndrome, efferent loop syndrome, anaemia due to B12 deficiency, and metabolic bone disease. It is important for patients to be aware of these potential complications and to discuss any concerns with their healthcare provider. With proper management and care, many of these syndromes can be effectively treated.
-
This question is part of the following fields:
- Surgery
-
-
Question 13
Incorrect
-
A 50-year-old woman visits her general practitioner complaining of a rash on her left nipple. She has no significant medical or family history. Upon examination, the doctor observes an erythematosus rash on the left nipple with thickening. The areola appears normal, and there are no palpable masses in the breast or axillary tail. The right breast is also unremarkable. What is the best course of action for this patient?
Your Answer:
Correct Answer: Urgent referral to breast clinic
Explanation:If a patient presents with reddening and thickening of the nipple and areola, it is important to consider Paget’s disease of the breast. This condition can be similar to nipple eczema, but the key difference is that nipple eczema starts in the areola and spreads to the nipple, while Paget’s disease starts at the nipple and spreads to the areola in later stages. Regardless of whether a mass can be felt, Paget’s disease of the nipple is strongly suggestive of breast cancer and requires an urgent referral to the breast clinic. Therefore, the correct answer is urgent referral to the breast clinic. Routine referral is not sufficient as this condition requires urgent attention. Topical corticosteroids and emollients may be used to manage moderate nipple eczema, but they are not appropriate for Paget’s disease. Similarly, topical emollients and tacrolimus are not effective treatments for Paget’s disease.
Paget’s disease of the nipple is a condition that affects the nipple and is associated with breast cancer. It is present in a small percentage of patients with breast cancer, typically around 1-2%. In half of these cases, there is an underlying mass lesion, and 90% of those patients will have an invasive carcinoma. Even in cases where there is no mass lesion, around 30% of patients will still have an underlying carcinoma. The remaining cases will have carcinoma in situ.
One key difference between Paget’s disease and eczema of the nipple is that Paget’s disease primarily affects the nipple and later spreads to the areolar, whereas eczema does the opposite. Diagnosis of Paget’s disease involves a punch biopsy, mammography, and ultrasound of the breast. Treatment will depend on the underlying lesion causing the disease.
-
This question is part of the following fields:
- Surgery
-
-
Question 14
Incorrect
-
A 68-year-old man presents to the Emergency Department with worsening abdominal pain over the past two days. The pain started in the lower left side of his abdomen and he has been experiencing diarrhoea. He has a medical history of hypertension, chronic kidney disease, and diverticular disease. On examination, his heart rate is 120 bpm, blood pressure is 135/80 mmHg, temperature is 38.5ºC, and oxygen saturation is 96% on air. His abdomen is tender throughout with involuntary guarding and rebound tenderness. Blood tests reveal the following results:
Hb 140 g/l Na+ 140 mmol/l Bilirubin 9 µmol/l
Platelets 730 * 109/l K+ 4.2 mmol/l ALP 70 u/l
WBC 18.9 * 109/l Urea 6.3 mmol/l ALT 36 u/l
Neuts 16.1 * 109/l Creatinine 115 µmol/l γGT 57 u/l
Lymphs 2.0 * 109/l Amylase 8 u/l Albumin 35 g/l
Which diagnostic test would be most appropriate to confirm the diagnosis?Your Answer:
Correct Answer: Erect chest x-ray
Explanation:To detect bowel perforation, an erect chest x-ray is commonly used. This is particularly useful in cases of suspected perforated diverticulitis, as it can reveal the presence of pneumoperitoneum (air under the diaphragm). A supine chest x-ray is not as effective in detecting this. While an abdominal x-ray can also suggest pneumoperitoneum, it is less sensitive than an erect chest x-ray. An intravenous urogram is not necessary in this case, as the patient’s symptoms do not align with those of ureteric colic, which is the most likely diagnosis. Ultrasound may also reveal air in the abdominal cavity, but its accuracy and image quality can vary greatly, making it a less optimal choice.
An erect chest x-ray is a useful tool for diagnosing an acute abdomen, as it can reveal the presence of free air in the abdomen, also known as pneumoperitoneum. This abnormal finding is indicative of a perforated abdominal viscus, such as a perforated duodenal ulcer. On an abdominal film, Rigler’s sign, also known as the double wall sign, may be visible. However, CT scans are now the preferred method for detecting free air in the abdomen.
The image used on license from Radiopaedia shows an erect chest x-ray with air visible under the diaphragm on both sides. Another image from Radiopaedia demonstrates an abdominal x-ray with numerous loops of small bowel outlined by gas, both within the lumen and free within the peritoneal cavity. Ascites, or fluid in the abdomen, is also visible, with mottled gas densities over bilateral paracolic gutters. In a normal x-ray, only the luminal surface should be visible outlined by gas, while the serosal surface should not be visible as it is normally in contact with other intra-abdominal content of similar density. However, in this case, gas abuts the serosal surface, making it visible. As this film was obtained supine, ascites pools in the paracolic gutters, with fluid mixed in with gas bubbles.
-
This question is part of the following fields:
- Surgery
-
-
Question 15
Incorrect
-
A 50-year-old woman visits her GP with a complaint of sudden anal pain. During the examination, the doctor notices a tender, oedematous, purplish subcutaneous perianal lump. What is the probable diagnosis?
Your Answer:
Correct Answer: Thrombosed haemorrhoids
Explanation:The posterior midline is where anal skin tags are commonly found. Genital warts, caused by HPV types 6 & 11, are small fleshy bumps that may be pigmented and cause itching or bleeding. Pilonidal sinus can cause pain and discharge in cycles due to hair debris creating sinuses in the skin, and if located near the anus, may cause anal discomfort.
Thrombosed haemorrhoids are characterized by severe pain and the presence of a tender lump. Upon examination, a purplish, swollen, and tender subcutaneous perianal mass can be observed. If the patient seeks medical attention within 72 hours of onset, referral for excision may be necessary. However, if the condition has progressed beyond this timeframe, patients can typically manage their symptoms with stool softeners, ice packs, and pain relief medication. Symptoms usually subside within 10 days.
-
This question is part of the following fields:
- Surgery
-
-
Question 16
Incorrect
-
A 35-year-old man with a past medical history of internal hemorrhoids presents with a recent exacerbation of symptoms. He reports having to manually reduce his piles after bowel movements. What grade of hemorrhoids is he experiencing?
Your Answer:
Correct Answer: Grade III
Explanation:Understanding Haemorrhoids
Haemorrhoids are a normal part of the anatomy that contribute to anal continence. They are mucosal vascular cushions found in specific areas of the anal canal. However, when they become enlarged, congested, and symptomatic, they are considered haemorrhoids. The most common symptom is painless rectal bleeding, but pruritus and pain may also occur. There are two types of haemorrhoids: external, which originate below the dentate line and are prone to thrombosis, and internal, which originate above the dentate line and do not generally cause pain. Internal haemorrhoids are graded based on their prolapse and reducibility. Management includes softening stools through dietary changes, topical treatments, outpatient procedures like rubber band ligation, and surgery for large, symptomatic haemorrhoids. Acutely thrombosed external haemorrhoids may require excision if the patient presents within 72 hours, but otherwise can be managed with stool softeners, ice packs, and analgesia.
Overall, understanding haemorrhoids and their management is important for individuals experiencing symptoms and healthcare professionals providing care.
-
This question is part of the following fields:
- Surgery
-
-
Question 17
Incorrect
-
A 29-year-old man has been waiting for surgery to repair a right inguinal hernia. He is now admitted with abdominal distension and colicky pain, along with vomiting bile and no bowel movements for two days. He is typically healthy and not on any medication. On examination, he appears dehydrated with a red, tender swelling in the right groin. X-rays confirm a small bowel obstruction, and a nasogastric tube is inserted. What is the most appropriate course of treatment for this patient?
Your Answer:
Correct Answer: Surgery with decompression of the bowel and hernia repair
Explanation:Management of Small Bowel Obstruction
Small bowel obstruction is a condition that requires a certain diagnosis before surgery. However, in cases where the cause of the obstruction is an obstructed groin hernia, a contrast study or ultrasound scan of the groin is unnecessary. The patient should be well resuscitated and undergo surgery to reduce and inspect the bowel for viability. Repair of the hernia should proceed, and inspection of incarcerated bowel is important.
In cases of adhesional obstruction, expectant drip and suck management may be appropriate, as the obstruction may settle with adequate decompression of the bowel. A contrast study may also be helpful in incomplete obstruction, as gastrografin has a therapeutic laxative effect. However, indications for surgery in bowel obstruction are an obstructed hernia and signs of peritonism, which indicate ischaemic bowel.
In summary, the management of small bowel obstruction depends on the cause of the obstruction. In cases of an obstructed groin hernia, surgery is necessary, while expectant management may be appropriate in adhesional obstruction. A contrast study may also be helpful in incomplete obstruction. It is important to consider the indications for surgery, such as signs of peritonism, to prevent further complications.
-
This question is part of the following fields:
- Surgery
-
-
Question 18
Incorrect
-
A 28-year-old man visits his doctor with a complaint of a painless lump he discovered on his right testicle while showering. He has no other symptoms or significant family history except for his father's death from pancreatic cancer two years ago. During the examination, the doctor identifies a hard nodule on the right testicle that does not trans-illuminate. An ultrasound is performed, and the patient is eventually referred for an inguinal orchiectomy for a non-invasive stage 1 non-seminoma germ cell testicular tumor. Based on this information, which tumor marker would we anticipate to be elevated in this patient?
Your Answer:
Correct Answer: AFP
Explanation:The correct tumor marker for non-seminoma germ cell testicular cancer is not serum gamma-glutamyl transpeptidase (gamma-GT), as it is only elevated in 1/3 of seminoma cases. PSA, which is a marker for prostate cancer, and CA15-3, which is produced by glandular cells of the breast and often raised in breast cancer, are also not appropriate markers for this type of testicular cancer.
Understanding Testicular Cancer
Testicular cancer is a type of cancer that commonly affects men between the ages of 20 and 30. Germ-cell tumors are the most common type of testicular cancer, accounting for around 95% of cases. These tumors can be divided into seminomas and non-seminomas, which include embryonal, yolk sac, teratoma, and choriocarcinoma. Other types of testicular cancer include Leydig cell tumors and sarcomas. Risk factors for testicular cancer include infertility, cryptorchidism, family history, Klinefelter’s syndrome, and mumps orchitis.
The most common symptom of testicular cancer is a painless lump, although some men may experience pain. Other symptoms may include hydrocele and gynaecomastia, which occurs due to an increased oestrogen:androgen ratio. Tumor markers such as hCG, AFP, and beta-hCG may be elevated in germ cell tumors. Ultrasound is the first-line diagnostic tool for testicular cancer.
Treatment for testicular cancer depends on the type and stage of the tumor. Orchidectomy, chemotherapy, and radiotherapy may be used. Prognosis for testicular cancer is generally excellent, with a 5-year survival rate of around 95% for seminomas and 85% for teratomas if caught at Stage I. It is important for men to perform regular self-examinations and seek medical attention if they notice any changes or abnormalities in their testicles.
-
This question is part of the following fields:
- Surgery
-
-
Question 19
Incorrect
-
An 81-year-old man has fallen off his bike and hit his head. His friend at the scene reports that he was unconscious for less than a minute. The man was cycling slowly on a path beside a canal. Upon initial assessment, he has some bruising on his upper and lower limbs, a Glasgow coma score (GCS) of 15, and no neurological deficit. He has not experienced vomiting or seizures since the accident and was able to describe the incident. He takes antihypertensives but has no significant medical history. What would be the most appropriate next step?
Your Answer:
Correct Answer: Perform a CT head scan within 8 hours
Explanation:When it comes to detecting significant brain injuries in the acute setting, CT imaging of the head is currently the preferred method of investigation. MRI is not typically used due to safety concerns, logistical challenges, and resource limitations.
According to NICE guidelines, patients over the age of 65 who experience a head injury resulting in loss of consciousness or amnesia should undergo a CT head scan within 8 hours. However, if there is an indication for a CT head scan within 1 hour, that should take priority. The specific indications for CT head scans within 1 hour and 8 hours can be found below.
Reference:
NICE (2014): Head injury: assessment and early management.NICE Guidelines for Investigating Head Injuries in Adults
Head injuries can be serious and require prompt medical attention. The National Institute for Health and Care Excellence (NICE) has provided clear guidelines for healthcare professionals to determine which adult patients need further investigation with a CT head scan. Patients who require immediate CT head scans include those with a Glasgow Coma Scale (GCS) score of less than 13 on initial assessment, suspected open or depressed skull fractures, signs of basal skull fractures, post-traumatic seizures, focal neurological deficits, and more than one episode of vomiting.
For patients with any loss of consciousness or amnesia since the injury, a CT head scan within 8 hours is recommended for those who are 65 years or older, have a history of bleeding or clotting disorders, experienced a dangerous mechanism of injury, or have more than 30 minutes of retrograde amnesia of events immediately before the head injury. Additionally, patients on warfarin who have sustained a head injury without other indications for a CT head scan should also receive a scan within 8 hours of the injury.
It is important for healthcare professionals to follow these guidelines to ensure that patients receive appropriate and timely care for their head injuries. By identifying those who require further investigation, healthcare professionals can provide the necessary treatment and support to prevent further complications and improve patient outcomes.
-
This question is part of the following fields:
- Surgery
-
-
Question 20
Incorrect
-
As a healthcare professional in the emergency department, you come across an elderly overweight man who appears to be in a drowsy state. Upon calling out his name, you hear a grunting sound. The patient has periorbital ecchymosis and clear fluid leaking from one nostril. Additionally, his oxygen saturation levels are at 82% on air.
Which airway adjunct should you avoid using in this patient?Your Answer:
Correct Answer: Nasopharyngeal airway
Explanation:If a patient is suspected or known to have a basal skull fracture, nasopharyngeal airways should not be used. This is because there is a rare risk of inserting the airway into the cranial cavity. Signs of a basal skull fracture include periorbital ecchymosis (raccoon eyes), CSF rhinorrhoea, haemotympanum, and mastoid process bruising (battle’s sign). While ET tubes, i-gels, and LMAs do not have contraindications, they should not be the first-line option and should only be inserted by a trained professional, typically an anaesthetist.
Nasopharyngeal Airway for Maintaining Airway Patency
Nasopharyngeal airways are medical devices used to maintain a patent airway in patients with decreased Glasgow coma score (GCS). These airways are inserted into the nostril after being lubricated, and they come in various sizes. They are particularly useful for patients who are having seizures, as an oropharyngeal airway (OPA) may not be suitable for insertion.
Nasopharyngeal airways are generally well-tolerated by patients with low GCS. However, they should be used with caution in patients with base of skull fractures, as they may cause further damage. It is important to note that these airways should only be inserted by trained medical professionals to avoid any complications. Overall, nasopharyngeal airways are an effective tool for maintaining airway patency in patients with decreased GCS.
-
This question is part of the following fields:
- Surgery
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)