-
Question 1
Correct
-
The pelvis includes which of the following bones:
Your Answer: Ilium, ischium, pubis, sacrum & coccyx
Explanation:The pelvic skeleton is formed posteriorly (in the area of the back), by the sacrum and the coccyx and laterally and anteriorly (forward and to the sides), by a pair of hip bones. Each hip bone consists of 3 sections, ilium, ischium, and pubis.
-
This question is part of the following fields:
- Anatomy
-
-
Question 2
Incorrect
-
Changes in the urinary tract system in pregnancy include:
Your Answer: Marked increase in both GFR & RPF when the patient is supine
Correct Answer: Increase in the glomerular filtration rate (GFR)
Explanation:Pregnancy involves remarkable orchestration of physiologic changes. The kidneys are central players in the evolving hormonal milieu of pregnancy, responding and contributing to the changes in the environment for the pregnant woman and foetus. The functional impact of pregnancy on kidney physiology is widespread, involving practically all aspects of kidney function. The glomerular filtration rate increases 50% with subsequent decrease in serum creatinine, urea, and uric acid values.
-
This question is part of the following fields:
- Physiology
-
-
Question 3
Incorrect
-
After six weeks of amenorrhoea, a 25-year-old woman appears with stomach discomfort and vaginal bleeding. If she has a tubal ectopic pregnancy, which of the following combinations of physical indications is most likely?
Your Answer: Profound shock with a rapid pulse and low BP.
Correct Answer: Little guarding but marked rebound tenderness in the suprapubic region.
Explanation:Blood in the peritoneal cavity rarely causes rigidity like that of a board (this is generally only found when chemical or purulent peritonitis is present).
When there is blood, there is usually a lot of rebound soreness and a lot of guarding.
A tubal ectopic pregnancy causes discomfort and tenderness in the lower abdomen, but it is not always localised to the side of the disease.
Shock is uncommon since the diagnosis is usually recognised before there is enough blood loss to elicit such signs.
Pelvic soreness is more prevalent than a pelvic mass that may be seen on a clinical exam.
Where a mass is visible, it could be an ectopic pregnancy, but it’s more likely to be a pregnancy surrounded by a blood clot caused by a leaking ectopic pregnancy. -
This question is part of the following fields:
- Gynaecology
-
-
Question 4
Incorrect
-
Which of the following is an appropriate treatment for Diazepam overdose?
Your Answer: Protamine
Correct Answer: Flumazenil
Explanation:Flumazenil is used for benzodiazepine overdose.
Naloxone is used for opioid overdose.
Parvolex (N-acetyl cysteine) is used for paracetamol overdose.
Protamine can be used for Heparin reversal.
Beriplex can be used for Warfarin reversal. -
This question is part of the following fields:
- Pharmacology
-
-
Question 5
Incorrect
-
What is the contraception of choice for epileptics on enzyme inducing antiepileptic drugs?
Your Answer: Barrier methods
Correct Answer: Levonorgestrel-releasing intrauterine contraceptive device
Explanation:Clinical decision making which contraceptive regimen is optimal for an individual woman with epilepsy is one of the most challenging tasks when taking care of women with epilepsy. The bidirectional interactive potential of antiepileptic drugs (AEDs) and hormonal contraceptives needs to be taken into account. Enzyme inducing (EI)-AEDs may reduce the contraceptive efficacy of hormonal contraceptives.
If combined oral contraceptives (COCs) are used in combination with EI-AEDs, it is recommended to choose a COC containing a high progestin dose, well above the dose needed to inhibit ovulation, and to take the COC pill continuously (“long cycle therapy”). But even with the continuous intake of a COC containing a higher progestin dose contraceptive safety cannot be guaranteed, thus additional contraceptive protection may be recommended.
Progestin-only pills (POPs) are likely to be ineffective, if used in combination with EI-AEDs.
Subdermal progestogen implants are not recommended in patients on EI-AEDs, because of published high failure rates.
Depot medroxyprogesterone-acetate (MPA) injections appear to be effective, however they may not be first choice due to serious side effects (delayed return to fertility, impaired bone health).
The use of intrauterine devices is an alternative method of contraception in the majority of women, with the advantage of no relevant drug–drug interactions. The levonorgestrel intrauterine system (IUS) appears to be effective, even in women taking EI-AEDs. Likelihood of serious side effects is low in the IUS users.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 6
Incorrect
-
A 56 year old lady presents with a vulval itch and discolouration. A biopsy conforms Lichen Sclerosis (LS). What is the risk of developing squamous cell carcinoma compared to patients with a normal vulval biopsy?
Your Answer: <5%
Correct Answer:
Explanation:Lichen Sclerosis is a destructive inflammatory condition that effects the anogenital region of women. It effects around 1 in 300 women. It destroys the subdermal layers of the skin resulting in hyalinization of the skin leading to parchment paper appearance of the skin. It is associated with vulval cancer and it is estimated that the risk of developing vulval cancer after lichen sclerosis is around 3-5%.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 7
Correct
-
All the following are possible causes of polyhydramnios, EXCEPT:
Your Answer: IUGR
Explanation:An underlying disease is only found in 17 % of cases in mild polyhydramnios. In contrast, an underlying disease is detected in 91 % of cases in moderate to severe polyhydramnios. The literature lists the following potential aetiologies: fetal malformations and genetic anomalies (8–45 %), maternal diabetes mellitus (5–26 %), multiple pregnancies (8–10 %), fetal anaemia (1–11 %), other causes, e.g. viral infections, Bartter syndrome, neuromuscular disorders, maternal hypercalcemia. Viral infections which can lead to polyhydramnios include parvovirus B19, rubella, and cytomegalovirus. Other infections, e.g. toxoplasmosis and syphilis, can also cause polyhydramnios.
-
This question is part of the following fields:
- Physiology
-
-
Question 8
Incorrect
-
A 21-year-old woman at 39 weeks of gestation in her second pregnancy is admitted in the hospital for severe abdominal pain. She notes that also has been having vaginal bleeding of about one litre and uterine contractions are present. Her previous pregnancy was a vaginal, without any complications. Her current blood pressure is 95/50 mmHg with a pulse rate of 120 beats/min. On physical examination, the uterus is palpable at the level of the xiphisternum and is firm. It is acutely tender to palpation. Fetal heart sounds cannot be heard on auscultation or with Doppler assessment. The cervix is 4 cm dilated and fully effaced. Immediate resuscitative measures are taken. Which of the following is the most appropriate next step in management for this patient?
Your Answer: A Caesarean section.
Correct Answer: Amniotomy
Explanation:This patient is presenting with a severe placental abruption causing fetal death and shock in the mother. The most appropriate initial management for the patient is to treat her shock with blood transfusions and exclude or treat any coagulation disorder resulting from the abruption. Delivery also needs to be expedited to remove the dead foetus. An amniotomy is usually all that is required to induce spontaneous labour as the uterus is usually very irritable. Spontaneous labour is likely to occur in this case, where the cervix is already 4 cm dilated and fully effaced.
Caesarean section is rarely needed to be done when the foetus is already dead.
Vaginal prostaglandin and an oxytocin (Syntocin®) infusion are not needed and unlikely to be required.
Ultrasound examination to confirm the diagnosis and fetal death is also unnecessary given the clinical and Doppler findings.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 9
Correct
-
Which one of the following statements is true regarding androgen insensitivity syndrome?
Your Answer: They have no uterus
Explanation:Androgen insensitivity syndrome means that patients are phenotypically males but they are resistant or insensitive to male androgen hormones. They do not have a uterus. Due to insensitivity to androgens these patients often have female traits but their genetic makeup is of male, 46XY.
-
This question is part of the following fields:
- Embryology
-
-
Question 10
Correct
-
Regarding molding of the fetal head, which one is true?
Your Answer: Does NOT have time to occur in breech delivery
Explanation:Molding allows the skull bones of the fetal head some mobility during the normal delivery of foetus as the skull changes its shape to accommodate passage through the mothers pelvis. However this does not occur in breach delivery where the skull is in circular shape. Babies born breech typically have craniofacial and limb deformations resulting from their in utero position. These babies characteristically have a long, narrow head, (“dolichocephaly” or “type 1”), with a prominent occipital shelf, redundant skin over the neck, overlapping lambdoidal sutures, and an indentation below their ears (from shoulder compression).
-
This question is part of the following fields:
- Anatomy
-
-
Question 11
Correct
-
What is the anterior boundary of the pelvic outlet?
Your Answer: pubic arch
Explanation:Pelvic Outlet Boundaries Anteriorly: Pubic arch Laterally: Ischial tuberosities Posterolaterally: Inferior margin of the sacrotuberous ligament Posteriorly: Tip of the coccyx Note: The pelvis outlet is also called the inferior aperture. The pelvic brim is the superior aperture
-
This question is part of the following fields:
- Anatomy
-
-
Question 12
Correct
-
A 21-year-old primigravida female presents to the emergency department at 41 weeks gestation. She complains of a nine hour history of irregular painful contractions. On examination of her pelvis, her cervix is fully effaced, but only 2 - 3 cm dilated. The fetal head is at the level of the ischial spines in a left occipito-posterior (LOP) position. The membranes ruptured an hour ago. What would be the best next line of management?
Your Answer: Oxytocic (Syntocinon4) infusion.
Explanation:The best next line of management is to administer an oxytocic (Syntocinon) infusion.
This is because the progress of labour is slow, and it necessary to augment it. As the membranes have already ruptured, the next step is to increase the contractions and induce labour using an infusion of oxytocic (Syntocinon) infusion.
Extra fluid is also required, but this will be administered alongside the Syntocinon infusion.
A lumbar epidural block is indicated in patients with an occipito-posterior (OP) position. This should not be attempted until more pain relief is required and the progress of labour is reassessed.
A Caesarean section may be necessary due to obstructed labour or fetal distress, it is not indicated at this stage.
Taking blood and holding it in case cross-matching is ultimately required is common, but most patients do not have blood cross-matched prophylactically in case there is a need to be delivered by Caesarean section and require a transfusion.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 13
Correct
-
A 32 year old patient has a transvaginal ultrasound scan that shows a mass in the left ovary. It is anechoic, thin walled, is without internal structures and measures 36mm in diameter. What is the likely diagnosis?
Your Answer: Functional cyst
Explanation:The diagnosis of functional ovarian cyst is made when the cyst measures more than 3 cm and rarely grows more than 10 cm. It appears as a simple anechoic unilocular cyst on USS. It is usually asymptomatic. If it is symptomatic then laparoscopic cystectomy should be performed.
-
This question is part of the following fields:
- Data Interpretation
-
-
Question 14
Correct
-
A 52 years old patient wants to see her options of HRT for menopausal symptoms. Which statement is true about continues use of combined HRT?
Your Answer: It increases the risk of breast cancer
Explanation:Most types of HRT increase the risk of breast cancer. But the risk is higher for those using combined HRT, which uses both oestrogen and progestogen. Vaginal oestrogens are not linked to an increased risk of breast cancer, whereas tibolone is. Taking HRT for 1 year or less only slightly increases breast cancer risk. However, the longer you take HRT the greater the risks are, and the longer they last.
Evidence is insufficient to conclude that long-term oestrogen therapy or hormone therapy use improves cardiovascular outcomes.
HRT containing oestrogen alone increases risk of endometrial cancer. However, this is not the case when using combined HRT.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 15
Correct
-
What is the most common cause of sepsis in the puerperium?
Your Answer: Endometritis
Explanation:Significant puerperal pyrexia is defined as a temperature of 38ºC or higher on any two of the first 10 days postpartum, exclusive of the first 24 hours. A mixed flora normally colonizes the vagina with low virulence. Puerperal infection is usually polymicrobial and involves contaminants from the bowel that colonize the perineum and lower genital tract. Following delivery, natural barriers to infection are temporarily removed and therefore organisms with a pathogenic potential can ascend from the lower genital tract into the uterine cavity. Placental separation exposes a large raw area equivalent to an open wound, and retained products of conception and blood clots within the uterus can provide an excellent culture medium for infection.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 16
Correct
-
The vulva is mainly supplied by which one of the following vessels?
Your Answer: Pudendal artery
Explanation:Vulva is defined by the area which is located outside the female vagina and comprises of the labia majora, labia minora, clitoris, mons pubis and Bartholin glands. It is supplied by the vestibula branch of pudental artery.
Inferior hemorrhoidal artery supplies the lower part of the rectum.
Femoral artery is the continuation of external iliac artery and supplies most of the leg. -
This question is part of the following fields:
- Anatomy
-
-
Question 17
Incorrect
-
An 18 year old girl presented with dysmenorrhea and irregular cycles. The most appropriate management in this case would be?
Your Answer: Mini pill
Correct Answer: Combined pill
Explanation:Combined oral contraceptive pills have an anti ovulatory function and also reduce the pain of menstruation.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 18
Correct
-
A 34 year old patient who has just undergone a C-section delivery has lost almost 1 litre of blood. You suspect uterine atony as the likely cause, and have bimanually compressed the uterus. Which of the following pharmacological interventions should follow?
Your Answer: Syntocin 5u by slow intravenous injection
Explanation:In the management of postpartum haemorrhage, it is essential that the bleeding is first mechanically prevented, followed by the administration of oxytocic drugs, which cause the uterine smooth muscle to contract and clamping off bleeding sites in the endometrium. The drug of choice in the treatment protocol of PPH is 5 units of syntocin, a synthetic oxytocin uterotonic, by slow intravenous infusion. This is particularly suitable in the case of uterine atony. Other uterotonics, misoprostol, carboprost, ergometrine, can be used, but are not as effective in an emergency setting.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 19
Correct
-
Which of the following is the primary source of oestrogen ?
Your Answer: Granulosa cells
Explanation:Ovarian granulosa cells (GC) are the major source of oestradiol synthesis. Induced by the preovulatory luteinizing hormone (LH) surge, cells of the theca and, in particular, of the granulosa cell layer profoundly change their morphological, physiological, and molecular characteristics and form the progesterone-producing corpus luteum that is responsible for maintaining pregnancy.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 20
Correct
-
A 39-year-old woman comes to your clinic for assessment and advice as she is planning to conceive over past three months with no success. She has a history of obesity with BMI 40 and type 2 diabetes mellitus with latest HbA1c value of 11%. She had her last eye check six months ago which shows no evidence of retinopathy, and she does not have diabetic nephropathy. Among the following which is a contraindication to pregnancy in this case?
Your Answer: History of type 2 diabetes mellitus with HBA1C above 10
Explanation:In patients who have an HbA1C value above 10%, it is better to postpone pregnancy until diabetes is under control. Also in those patients with type 2 diabetes mellitus, who are suffering from severe gastroparesis, those with advanced retinopathy, with severe diabetic renal disease and severe ischemic heart disease with uncontrolled hypertension pregnancy is contraindicated.
All the other options mentioned are incorrect.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 21
Correct
-
Question 22
Incorrect
-
A 32-year-old woman visited your clinic at her 30th week of gestation, complaining of left lower limb pain. The doppler ultrasound findings had confirmed proximal deep vein thrombosis and she was treated with low molecular weight heparin. Now she is at her 34 weeks of gestation, and is expecting delivery in next four weeks. What would be your advice for her today?
Your Answer: Cease all anti-coagulants
Correct Answer: Low molecular weight heparin should be switched to unfractionated heparin
Explanation:This patient has developed deep vein thrombosis during pregnancy and required anti-coagulation as part of treatment for up to 3-6 months. Enoxaparin, which is a low molecular weight heparin, is preferred over heparin due to the once or twice a day therapeutic dosing. Also monitoring of aPTT is not required in this case.
There is an association between Enoxaparin and an increased risk for epidural hematoma in women receiving epidural anaesthesia during labour. Considering that the patient mentioned is expected to go for delivery in 4 weeks and the possibility of her needing an epidural anaesthesia or general anaesthesia in case of undergoing a cesarean section, enoxaparin should be switched to unfractionated heparin, four weeks prior to the anticipated delivery. This is because of the fact that heparin can be antidoted with protamine sulphate.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 23
Correct
-
A 28-year-old woman who is at the 18th week of gestation presented to the medical clinic due to a vaginal discharge. Upon history taking, it was revealed that she had a history of preterm labour at 24 weeks of gestation during her last pregnancy. Upon examination, the presence of a clear fluid coming out of the vagina was noted. Which of the following is considered to be the best in predicting pre-term labour?
Your Answer: Cervical length of 15mm
Explanation:Preterm birth is the leading cause of neonatal morbidity and mortality not attributable to congenital anomalies or aneuploidy. It has been shown that a shortened cervix is a powerful indicator of preterm births in women with singleton and twin gestations – the shorter the cervical length, the higher the risk of spontaneous preterm birth. Ultrasound measurements of the cervix are a more accurate way of determining cervical length (CL) than using a digital method.
25 mm has been chosen as the ‘cut off’ at above which a cervix can be regarded as normal, and below which can be called short. A cervix that is less than 25 mm may be indicative of preterm birth.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 24
Correct
-
Congenital Cytomegalovirus (CMV) infection effects how many pregnancies?
Your Answer: 1 in 150
Explanation:CMV effects 1 in 200 pregnancies of which 30% will transmit the virus to the foetus and of which 30% foetus will be effected.
-
This question is part of the following fields:
- Microbiology
-
-
Question 25
Correct
-
Which Immunoglobulin (or antibody) is secreted in large amounts in breast milk?
Your Answer: IgA
Explanation:When considering immunoglobulins in neonates. There are only a few key points you are likely to be tested on. 1. IgA is resistant to stomach acid and found in large amounts in breast milk. 2. IgG is the only Ig that can cross the placenta so is key for passive neonatal immunity 3. When the neonate starts synthesising its own Ig it is IgM that is produced first.
-
This question is part of the following fields:
- Immunology
-
-
Question 26
Correct
-
A 41-year-old woman (gravida 2, para 1) presents at eight weeks gestation for her first antenatal visit. This is her second pregnancy. She is worried about Down syndrome risk in her foetus. From the following options listed, select the safest test (i.e., the one with least risk of causing adverse consequences in the pregnancy) that will provide an accurate diagnosis regarding the presence or absence of Trisomy 21 in the foetus.
Your Answer: Amniocentesis at 16 weeks of gestation.
Explanation:Nuchal translucency scans and maternal screening tests simply aid in determining a risk percentage for the presence of Trisomy 21, but an accurate diagnosis cannot be reached.
Chorionic villous biopsy (CVB), amniocentesis, and cordocentesis, are all prenatal diagnostic tests that can provide a definitive diagnosis regarding the presence of foetal abnormalities.
Amniocentesis performed at 16 weeks of gestation is associated with the lowest risk for miscarriage and hence is the safest test and should be recommended to the mother (correct answer).
The miscarriage risk from a CVB is at least double the risk following amniocentesis.
Nowadays, cordocentesis is rarely used for sampling of foetal material to detect chromosomal abnormalities as the test poses an even higher risk of miscarriage compared to the other procedures discussed above.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 27
Correct
-
a 24 year old female patient comes to your office with a chief complaint of painless vaginal bleeding of 1 week duration. She had 3 episodes of bleeding and is on contraceptive pills. Her Pap smear screening is up to date with normal findings. Which is the cause for her bleeding?
Your Answer: A cervical ectropion
Explanation:Cervical ectropion occurs when glandular cells develop on the outside of the cervix. Many individuals with cervical ectropion do not experience symptoms.
However, the primary symptom of cervical ectropion is a red, inflamed patch at the neck of the cervix.
The transformation zone appears this way because the glandular cells are delicate and irritate easily.
Other symptoms a woman may experience include:
pain and bleeding during or after sex
pain during or after cervical screening
light discharge of mucus
spotting between periods
Symptoms may range from mild to severe when they appear.This patient has normal pap smear and is unlikely to have cervical cancer. She has no fever and vaginal discharge which would be the presentation of Chlamydia infection.
Endometrial cancer affects mainly post menopausal women and presents with vaginal bleeding, weight loss, dysuria and dyspareunia.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 28
Incorrect
-
The inguinal canal is reinforced anterolaterally by which structure?
Your Answer: Aponeurosis external oblique
Correct Answer: Internal oblique
Explanation:The Conjoint tendon AKA Inguinal falx reinforces the posterior wall of the inguinal canal. The inguinal ligament is part of the floor.
The aponeurosis of external oblique is the major component of the anterior wall with fibres of internal oblique reinforcing the lateral part -
This question is part of the following fields:
- Anatomy
-
-
Question 29
Incorrect
-
What percentage of infants will have permanent neurological dysfunction as a result of brachial plexus injury secondary to shoulder dystocia?
Your Answer: 50%
Correct Answer:
Explanation:Shoulder dystocia occurs when the anterior or posterior fetal shoulder impacts on the maternal symphysis or sacrum and may require additional manevours to release the shoulders after gentle downward traction has failed. The most common injury that can occur, is to the brachial plexus due to lateral flexion of the head during traction. This may cause a neurological disability, Erb’s Palsy ( injury to C5 and C6 of the brachial plexus) in which there is a less than 10% chance that this injury would be permanent.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 30
Correct
-
Regarding the uterine artery which of the following statements are TRUE?
Your Answer: It arises from the internal iliac artery
Explanation:The uterine artery arises from the internal iliac artery, in particular the anterior division of the internal iliac artery. Some older texts refer to the internal iliac as the hypogastric artery. The vaginal artery typically arises as its own branch of the internal iliac artery. The ovarian arteries are branches of the aorta
-
This question is part of the following fields:
- Anatomy
-
-
Question 31
Correct
-
Regarding lymph drainage of the lower vagina where does the majority of lymph drain to?
Your Answer: Inguinal nodes
Explanation:Lymphatic vessels from the vagina drain from the parts of the vagina as follows:
• Superior part: to the internal and external iliac lymph nodes.
• Middle part: to the internal iliac lymph nodes.
• Inferior part: to the sacral and common iliac nodes. -
This question is part of the following fields:
- Anatomy
-
-
Question 32
Incorrect
-
A 35-year-old lady with a 4-year history of hypertension is planning to conceive. She has never been pregnant before and has stopped using contraception recently. She has a past medical history of asthma and the only medication she is on is ramipril 10 mg daily. On examination her blood pressure is found to be 130/85 mm/Hg. From the following which is the most appropriate initial management of her hypertension?
Your Answer: Cease ramipril and start irbesartan
Correct Answer: Cease ramipril and start methyldopa
Explanation:In the given case pre-pregnancy counselling and management of chronic hypertension is very much essential.
Some commonly prescribed antihypertensive drugs like ACE inhibitors, angiotensin receptor antagonists, diuretics and most beta blockers are contraindicated or is best to be avoided before conception and during pregnancy.
Methyldopa is considered as the first line drug for the management of mild to moderate hypertension in pregnancy and is the most commonly prescribed antihypertensive for this indication.
Hydralazine can be used during any hypertensive emergencies in pregnancy.
Intake of Angiotensin receptor blockers and ACE inhibitors during the first trimester can lead to complications as they are both teratogenic; use of these drugs during second and third trimesters can result in foetal renal dysfunction, oligohydramnios and skull hypoplasia.
Diuretics can cause foetal electrolyte disturbances and significant reduction in maternal blood volume.
All beta blockers, except labetalol, can result in foetal bradycardia, and growth restriction in case its long-term use.
Calcium channel antagonists, except nifedipine, are avoided during pregnancy due to its high risk for maternal hypotension and foetal hypoxia. -
This question is part of the following fields:
- Obstetrics
-
-
Question 33
Correct
-
A 30-year-old woman who is at 38 weeks gestation presented to the emergency department due to complaints of not feeling fetal movements since yesterday. Upon investigations, fetal demise was confirmed. Induced delivery was done and she gave birth to a dead foetus. Which of the following is least likely to reveal the cause of the fetal death?
Your Answer: Chromosomal analysis of the mother
Explanation:Stillbirth has many causes: intrapartum complications, hypertension, diabetes, infection, congenital and genetic abnormalities, placental dysfunction, and pregnancy continuing beyond forty weeks.
In 5% of normal-appearing stillborns, a chromosomal abnormality will be detectable. With an autopsy and a chromosomal study, up to 35% of stillborns are found to have a major structural pathology, and 8% have abnormal chromosomes. After a complete evaluation, term stillbirth remains unexplained about 30% of the time. The chance of finding a cause is impacted by the age of the foetus, the experience of the caregiver, and the thoroughness of the exam. Chromosome testing for aneuploidy should be offered for all stillbirths to confirm or to seek a cause of the stillbirth. Genetic amniocentesis or chorionic villus sampling before delivery offers the highest yield.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 34
Correct
-
A young couple, both 26 years of age, presents to you with 11 months’ duration of infertility. On investigation, she is found to be ovulating, and her hysterosalpingogram is normal. On semen analysis, the following results were found: Semen volume 5mL (2-6 mL) Sperm count 1 million/mL * (>20 million) Motility 15% (>40%) Abnormal forms 95% (<60%) A second specimen three months later confirms the above results. Which would be the most suitable next step in management?
Your Answer: Carry out in vitro fertilisation (IVF) using intracytoplasmic sperm injection (ICSI).
Explanation:Achieving spontaneous pregnancy is rare in cases where a couple have been infertile with abnormal semen analysis (count <5million/mL and reduced motility), hence there is generally an indication for treatment. FSH injection usually would not be expected to improve the semen specimen. Rate of pregnancy would be much lower if at the time of intrauterine insemination, the total motile count is less 5 million. In this case, his count is 1 million. Pregnancy is likely to be achieved with donor sperm but as it would not contain the husband’s genetic material, it would be only considered later on once all other methods involving his own sperm have failed. Out of all the options, IVF would most likely result in a pregnancy, in which it allows the husband’s sperm to spontaneously fertilise the oocyte. Rate of pregnancy would roughly be 2% per treatment cycle. This rate would increase to roughly 20% if ISCI is also used.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 35
Correct
-
Question 36
Incorrect
-
During early pregnancy, a pelvic examination may reveal that one adnexa is slightly enlarged. This is most likely due to:
Your Answer: A parovarian cyst
Correct Answer: Corpus luteal cyst
Explanation:Adnexa refer to the anatomical area adjacent to the uterus, and contains the fallopian tube, ovary, and associated vessels, ligaments, and connective tissue. The reported incidence of adnexal masses in pregnancy ranges from 1 in 81 to 1 in 8000 pregnancies. Most of these adnexal masses are diagnosed incidentally at the time of dating or first trimester screening ultrasound (USS). Functional cyst is the most common adnexal mass in pregnancy, similar to the nonpregnant state. A corpus luteum persisting into the second trimester accounts for 13-17% of all cystic adnexal masses. Pain due to rupture, haemorrhage into the cyst, infection, venous congestion, or torsion may be of sudden onset or of a more chronic nature.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 37
Correct
-
You review a 28 year old patient in the fertility clinic. She has a diagnosis of PCOS. She has been trying to conceive for 2 years. Her BMI is 26 kg/m2. She is a non-smoker. She has been taking Clomiphene and metformin for the past 6 months. What is the next most appropriate treatment?
Your Answer: Gonadotrophins
Explanation:Clomiphene shouldn’t be continued for more than 6 months. The second line options are Gonadotrophins or ovarian drilling.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 38
Incorrect
-
Which of the following changes would you expect in pregnancy?
Your Answer: Increased TSH Decreased Total T3 and T4
Correct Answer: Decreased TSH Increased Total T3 and T4
Explanation:Human chorionic gonadotrophin (hCG) has thyrotrophic activity owing to subunit homology with thyroid-stimulating hormone (TSH) and maternal TSH production is suppressed during the first trimester of pregnancy, when hCG levels are highest. The TSH response to thyrotrophin-releasing hormone (TRH) is reduced during the first trimester but returns to normal after this. Thyroid binding globulin increases in the first 2 weeks of pregnancy and reaches a plateau by 20 weeks. This leads to increased production of total T3 (tri-iodothyronine) and T4 (thyroxine).
-
This question is part of the following fields:
- Endocrinology
-
-
Question 39
Correct
-
Which of the following is true about the origin of the ovarian artery?
Your Answer: It arises from the Abdominal Aorta
Explanation:The ovarian arteries are considered the main blood supply for the ovaries. The ovarian arteries usually arise from the lateral aspect of the abdominal artery, though in some instances they may arise from the renal or iliac arteries.
-
This question is part of the following fields:
- Anatomy
-
-
Question 40
Incorrect
-
Which one of the following statements regarding Turner's syndrome is true?
Your Answer: Genetically is 46 XO
Correct Answer: Usually presents with primary amenorrhea
Explanation:Turner syndrome patients present with primary amenorrhea, have non functional or streak ovaries and cant conceive. They are 45X genetically.
-
This question is part of the following fields:
- Embryology
-
-
Question 41
Incorrect
-
A 37-year-old primigravid woman is admitted to labor unit at 39 weeks of gestation, due to regular uterine contractions. Her cervix is 8 cm dilated and 100% effaced, with the fetus’ vertex at +1 station. Initially the fetal heart rate was 150 bpm, as the labor progressed, it falls to 80 bpm without any changes in the mother’s general condition. Which among the following options would be the best next step in management of this case?
Your Answer: Emergency delivery by cesarean section
Correct Answer: Cardiotocography
Explanation:Bradycardia of <100 bpm for more than 5 minutes or <80 for more than 3 minutes is always considered abnormal. The given case describes fetal bradycardia detected on fetal heart auscultation and the most common causes for severe bradycardia are prolonged cord compression, cord prolapse, epidural and spinal anesthesia, maternal seizures and rapid fetal descent. Immediate management including identification of any reversible causes for the abnormality and initiation of appropriate actions like maternal repositioning, correction of maternal hypotension, rehydration with intravenous fluid, cessation of oxytocin, tocolysis for excessive uterine activity, and initiation or maintenance of continuous CTG should be considered in clinical situations where abnormal fetal heart rate patterns are noticed. Consideration of further fetal evaluation and delivery if a significant abnormality persists are very important. The next step in this scenario where the baby is in 1+ station, with an abnormal fetal heart rate detected on auscultation would be to perform a confirmatory cardiotocography (CTG) and if the CTG findings confirm the condition despite initial measures obtained, prompt action should be taken. Cord compression or prolapse should come on the top of the differential diagnoses list as the the mother shows normal general conditions, but since the cervix is 8 cm dilated, 100% effaced and the fetal head is already engaged, cord prolapse would be unlikely; therefore, repeating vaginal exam is not as important as confirmatory CTG. However a vaginal exam should be done, if the scenario indicates any possibility of cord prolapse, to exclude cord compression or prolapse. NOTE– In cases of severe prolonged bradycardia, immediate delivery is recommended, if the cause cannot be identified and corrected.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 42
Correct
-
A 33-year-old lady seeks counsel from your clinic since she has a history of deep vein thrombosis. She was on progesterone-only tablets (POP) until fivemonths ago, when she decided to get pregnant. However, the pregnancy turned out to be ectopic. Thankfully, she made it through. She doesn't want to get pregnant again and asks if she may resume taking the tablets. Which of the following is the best piece of advise you could give?
Your Answer: She cannot take progesterone only pills
Explanation:Oestrogen-containing contraceptives are not recommended for this woman since she has a history of DVT. This is most likely why she was started on POP instead of standard combination tablets prior. Progesterone is also contraindicated with a history of ectopic pregnancy and should never be used again. Barrier approaches, for example, could be applied in this woman’s case.
The following are absolute contraindications to taking just progesterone pills:
– Pregnancy
– Breast cancer
– Vaginal bleeding that hasn’t been diagnosed
– Ectopic pregnancy history or a high risk of ectopic pregnancyProgesterone-only pills have the following relative contraindications:
– Active viral hepatitis
– Severe chronic liver disease
– Malabsorption syndrome
– Severe arterial disease
– Successfully treated breast cancer more than 5 years ago
– Concomitant use of hepatic enzyme inducing medications. -
This question is part of the following fields:
- Gynaecology
-
-
Question 43
Correct
-
Oxytocin binds to what receptor type?
Your Answer: G-protein-coupled receptors
Explanation:Oxytocin binds to the G protein coupled receptors that triggers the IP3 mechanism leading to an elevated intracellular calcium ion.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 44
Correct
-
A 26-year-old woman had a history of dilation and curettage for septic abortion. Currently, she has developed amenorrhea for 6 months already. It was also noted that she smokes 10 cigarettes and drinks 2 standard alcoholic drinks every day. She was tested for beta-hCG but it was not detectable. Which of the following is considered the most appropriate next step to establish a diagnosis?
Your Answer: Transvaginal ultrasound
Explanation:Asherman syndrome (intrauterine adhesions or intrauterine synechiae) occurs when scar tissue forms inside the uterus and/or the cervix. These adhesions occur after surgery of the uterus or after a dilatation and curettage.
Patients with Asherman syndrome may have light or absent menstrual periods (amenorrhea). Some have normal periods based on the surface area of the cavity that is affected. Others have no periods but have severe dysmenorrhea (pain with menstruation).
Although two-dimensional sonography may suggest adhesive disease, Asherman syndrome is more often evaluated initially with saline sonography or hysterosalpingography to demonstrate the adhesions.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 45
Correct
-
Looking at the picture below what is the diagnosis?
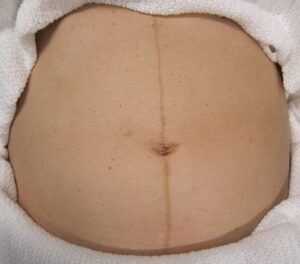
Your Answer: Linea Nigra
Explanation:This is Linea Nigra. It occurs in 3/4 of pregnancies and is due to increased melanocyte-stimulating hormone production by the placenta. This also causes melasma and darkening of the nipples.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 46
Incorrect
-
Regarding the closure of the ductus arteriosus (DA) after birth which of the following most accurately describes the mechanisms leading to closure of the DA?
Your Answer: Increased arterial pO2, increased bradykinin & increased Prostaglandin E2
Correct Answer: Increased arterial pO2, increased bradykinin & decreased Prostaglandin E2
Explanation:Functional closure of the ductus arteriosus is neonates is completed within the first few days after birth. It normally occurs by the 12th postnatal week. It has been suggested that persistent patency of DA results from a failure of the TGF-B induction after birth. Due to increased arterial pO2, constriction of the DA occurs. In addition to this on inflation the bradykinin system is activated with cause the smooth muscles in the DA to constrict. A decrease in the E2 prostaglandin is also an important factor as raised levels have been indicated in keeping the patency of the DA.
-
This question is part of the following fields:
- Embryology
-
-
Question 47
Incorrect
-
A 21-year-old woman, 9 weeks of gestation, has been admitted due to intractable vomiting with concurrent ketonuria. Past medical is unremarkable except for an appendectomy at the age of 12 years. Which of the following is the next best step in this investigation?
Your Answer: Pelvic ultrasound examination.
Correct Answer: Serum electrolytes, urea and creatinine.
Explanation:The finding of ketonuria in this patient indicates profound dehydration and electrolyte loss. Immediate investigation with baseline serum electrolytes, urea, and creatinine is recommended for aid In intravenous resuscitation and rehydration.
All other assessments listed are appropriate, however, baseline electrolyte concentration is important before initiating intravenous resuscitation.
Other causes that can lead to vomiting in early pregnancy include normal pregnancy, multiple pregnancies, molar pregnancies, or urinary tract infection. Urine culture is necessary to exclude urinary tract infection, pelvic ultrasound to confirm singleton or multiple pregnancy and rule out a molar pregnancy.
An erect abdominal Xray may help to rule out an organic intestinal obstruction in this patient. Her history of an appendectomy predisposes this patient to adhesions leading to small bowel obstruction. However, it is not the immediate assessment in this case.
Before the advent of ultrasound, a quantitative hCG analysis was indicated to assess the presence of molar pregnancy. However, ultrasound is now preferred to confirm this diagnosis.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 48
Correct
-
What is the average anteroposterior distance of the female pelvic outlet?
Your Answer: 13 cm
Explanation:The pelvic outlet is bounded in front by the lower margin of the symphysis pubis, on each side by the descending ramus of the pubic bone, the ischial tuberosity and the sacrotuberous ligament, and posteriorly by the last piece of the sacrum. The AP diameter of the pelvic outlet is 13.5 cm and the transverse diameter is 11 cm.
-
This question is part of the following fields:
- Anatomy
-
-
Question 49
Correct
-
Regarding feto-maternal blood circulation, which of the following statements is false?
Your Answer: At term the placenta receives 70% of uterine blood flow
Explanation:The placenta is important for regulating feto-maternal blood circulation, ensuring that the two circulatory systems do not come into direct contact. The placenta receives 70-80% of the uterine blood flow into the decidual spiral arteries where nutrient, waste and gaseous exchange with fetal blood takes place via the villous core fetal vessels. Deoxygenated blood arrives at the placenta via two uterine arteries while oxygenated, nutrient-rich blood is circulated back to the foetus via a single umbilical vein. The pressure in the umbilical vein is about 20 mmHg.
-
This question is part of the following fields:
- Embryology
-
-
Question 50
Incorrect
-
You are asked to see a 26 year old patient following her first visit to antenatal clinic. She is 9 weeks pregnant and bloods have shown her to be non-immune to Rubella. She is concerned about congenital rubella syndrome (CRS). What is the most appropriate advice to give?
Your Answer: Advise vaccination prior to 16 weeks gestation
Correct Answer: Advise vaccination after birth regardless of breast feeding status
Explanation:Congenital rubella infection that occurs after 16 weeks gestation does not typically cause fetal abnormalities. This however plays no part in vaccination advice. Rubella vaccine is live and should not be given during pregnancy. The mother should be offered vaccination after giving birth. It is safe for the vaccine (typically given as combined MMR) to be administered if the mother is breastfeeding.
-
This question is part of the following fields:
- Microbiology
-
-
Question 51
Incorrect
-
A 33 year old lady presented with complaints of heavy menstrual bleeding. She is otherwise well and her US abdomen is normal. What is the best treatment option?
Your Answer: Combined Oral Contraceptive Pill (COCP)
Correct Answer: Mirena coil
Explanation:Mirena coil is used for contraception and for long term birth control. It causes stoppage of menstrual bleeding however, in a few cases there may be inter-menstrual spotting.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 52
Correct
-
Question 53
Incorrect
-
When is the highest risk of maternal-fetal transmission of Toxoplasma Gondii during pregnancy?
Your Answer: 0-10 weeks
Correct Answer: 26-40 weeks
Explanation:The risk of transplacental transmission from mother to foetus is greater in later pregnancy i.e. 26-40 weeks. Although the risk of transmission is lower in early pregnancy, if infection does occur earlier, particularly before 10 weeks, then complications are typically more severe.
-
This question is part of the following fields:
- Microbiology
-
-
Question 54
Incorrect
-
Question 55
Incorrect
-
A 27-year-old woman complains of a hard, irregular lump in her right breast that presented after a car accident 2 weeks ago. Which is the most likely diagnosis?
Your Answer: Mastalgia
Correct Answer:
Explanation:Since the car crash happened two weeks prior, breast trauma is suggested and thus fat necrosis is the most probable diagnosis. Phyllodes tumours are typically a firm, palpable mass. These tumours are very fast-growing, and can increase in size in just a few weeks. Occurrence is most common between the ages of 40 and 50, prior to menopause.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 56
Correct
-
Polyhydramnios is associated with which one of the following conditions?
Your Answer: Tracheo-oesophageal fistula
Explanation:Oesophageal atresia/TE fistula may be suspected prenatally with ultrasound findings of polyhydramnios, absence of fluid in the stomach, small sized abdomen, or the presence of a dilated proximal oesophageal pouch. An underlying disease is only found in 17 % of cases in mild polyhydramnios. In contrast, an underlying disease is detected in 91 % of cases in moderate to severe polyhydramnios. The literature lists the following potential aetiologies: fetal malformations and genetic anomalies (8–45 %), maternal diabetes mellitus (5–26 %), multiple pregnancies (8–10 %), fetal anaemia (1–11 %), other causes, e.g. viral infections, Bartter syndrome, neuromuscular disorders, maternal hypercalcemia. Viral infections which can lead to polyhydramnios include parvovirus B19, rubella, and cytomegalovirus. Other infections, e.g. toxoplasmosis and syphilis, can also cause polyhydramnios.
-
This question is part of the following fields:
- Physiology
-
-
Question 57
Correct
-
A woman comes to your office two weeks after undergoing a total vaginal hysterectomy with anterior colporrhaphy and the Burch surgery for uterine prolapse and stress urine incontinence. Throughout the day, she complains of a continual loss of urine. She denies having any dysuria or urgency. Which of the following is the most likely cause of the problem?
Your Answer: Vesicovaginal fistula
Explanation:Vesicovaginal fistula (VVF) is a subtype of female urogenital fistula (UGF). VVF is an abnormal fistulous tract extending between the bladder and the vagina that allows the continuous involuntary discharge of urine into the vaginal vault. The uncontrolled leakage of urine into the vagina is the hallmark symptom of patients with UGFs. Patients may complain of urinary incontinence or an increase in vaginal discharge following pelvic surgery or pelvic radiotherapy with or without antecedent surgery. The drainage may be continuous; however, in the presence of a very small UGF, it may be intermittent. Increased postoperative abdominal, pelvic, or flank pain; prolonged ileus; and fever should alert the physician to possible urinoma or urine ascites and mandates expeditious evaluation. Recurrent cystitis or pyelonephritis, abnormal urinary stream, and haematuria also should initiate a workup for UGF.
Urinary trace infection presents with dysuria and urgency.
Detrusor instability causes urge incontinence.
Neurogenic bladder from diabetic neuropathy would also have urgency. -
This question is part of the following fields:
- Gynaecology
-
-
Question 58
Incorrect
-
A 26 year old lady comes to see you in the antenatal clinic. She is 8 weeks pregnant and is concerned as she has a new cat and her friend told her she shouldn't be changing cat litter when pregnant. You send bloods which show high IgM for toxoplasmosis gondii. Which of the following is an appropriate treatment option?
Your Answer: Metronidazole
Correct Answer: Spiramycin
Explanation:Toxoplasma gondii is a protozoan parasite found in cat faeces, soil or uncooked meat. Infection occurs by ingestion of the parasite from undercooked meat or from unwashed hands. Spiramycin treatment can be used in pregnancy (a 3-week course of 2–3 g per day). This reduces the incidence of transplacental infection but has not been shown to definitively reduce the incidence of clinical congenital disease. If toxoplasmosis is found to be the cause of abnormalities detected on ultrasound scan of the foetus, then termination of pregnancy can be offered.
-
This question is part of the following fields:
- Microbiology
-
-
Question 59
Correct
-
A 34 year old patient is being investigated in the infertility clinic and is offered Hysterosalpingography (HSG). She has 28 day cycles. Which of the following statements regarding HSG is correct?
Your Answer: Typically performed using iodine based water soluble contrast
Explanation:Hysterosalpingography is used to assess the patency of the fallopian tubes. It is performed by injection of a radio-opaque iodine based contrast. This test is contraindicated in pelvic inflammatory disease and during pregnancy. Should be performed in Follicular phase of menstrual cycle after cessation of menstrual bleeding and prior to ovulation (days 6-12).
-
This question is part of the following fields:
- Biophysics
-
-
Question 60
Incorrect
-
A patient undergoes surgery for a vaginal vault prolapse. After surgery she complains of numbness and groin pain. You assess her and find the numb area is the anterior aspect of the labia. Which nerve has likely been damaged during surgery?
Your Answer: Perineal
Correct Answer: Ilioinguinal
Explanation:This describes the sensory area supplied by the ilioinguinal nerve. This is a potential complication with pelvic surgery.
-
This question is part of the following fields:
- Anatomy
-
-
Question 61
Correct
-
During difficult labour, mediolateral episiotomy is favoured to midline episiotomy because?
Your Answer: Less extension of the incision
Explanation:Mediolateral episiotomy is favoured to midline episiotomy because there is less extension of the incision and decreased chances of injury to the anal sphincter and rectum.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 62
Correct
-
If your patient is 8 weeks pregnant which one of the following USS measurements is most useful?
Your Answer: Crown rump length
Explanation:Fetal crown-rump length (CRL) is recommended over last menstrual period for estimating GA when measured in early pregnancy i.e. before 9 to 13+6 weeks.
-
This question is part of the following fields:
- Anatomy
-
-
Question 63
Correct
-
The β-hCG curve in maternal serum in a normal pregnancy peaks at:
Your Answer: 10 weeks of pregnancy
Explanation:During the first 8 weeks of pregnancy, concentrations of hCG in the blood and urine usually double every 24 hours. Levels of the hormone typically peak at around 10 weeks, decline until 16 weeks, then remain constant.
-
This question is part of the following fields:
- Physiology
-
-
Question 64
Correct
-
A 20-year-old female patient who is experiencing pelvic pain is being cared for at your clinic. She describes bilateral pain that began gradually and was accompanied by fever, vaginal discharge, and mild dysuria. Her pelvic examination demonstrates uterine, adnexal, and cervical motion tenderness. Which of the following is the most likely cause of the pain?
Your Answer: PID
Explanation:Pelvic inflammatory disease (PID) refers to acute and subclinical infection of the upper genital tract in women, involving any or all of the uterus, fallopian tubes, and ovaries; this is often accompanied by involvement of the neighbouring pelvic organs. It results in endometritis, salpingitis, oophoritis, peritonitis, perihepatitis, and/or tubo-ovarian abscess.
Lower abdominal pain is the cardinal presenting symptom in women with PID. The abdominal pain is usually bilateral and rarely of more than two weeks’ duration. The character of the pain is variable, and in some cases, may be quite subtle. The recent onset of pain that worsens during coitus or with jarring movement may be the only presenting symptom of PID. The onset of pain during or shortly after menses is particularly suggestive.
Other non-specific complaints include urinary frequency and abnormal vaginal discharge.
Ovarian cyst, uterine leiomyoma, appendicitis or ectopic pregnancy do not present with fever and vaginal discharge although tenderness is noted in appendicitis and ectopic pregnancy. Therefore, these options do not explain the patient’s symptoms.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 65
Correct
-
Which of the following factors as shown to decrease ovarian cancer risk?
Your Answer: Taking statins
Explanation:Factors shown to decrease risk of ovarian cancer are:
– Oral contraceptive use
– Higher Parity
– Breast feeding
– Hysterectomy
– Tubal Ligation
– Statins
– SLE -
This question is part of the following fields:
- Epidemiology
-
-
Question 66
Incorrect
-
Which of the following is probably responsible for physiologic hyperventilation during pregnancy?
Your Answer: Large fluctuations in plasma bicarbonate
Correct Answer: Increased progesterone production
Explanation:Progesterone gradually increases during the course of pregnancy, from 25 ng⋅mL−1 at 6 weeks’ to 150 ng⋅mL−1 at 37 weeks’ gestation. Progesterone acts as trigger of the primary respiratory centre by increasing the sensitivity of the respiratory centre to carbon dioxide, as indicated by the steeper slope of the ventilation curve in response to alveolar carbon dioxide changes. Progesterone alters the smooth muscle tone of the airways resulting in a bronchodilator effect. It also mediates hyperaemia and oedema of mucosal surfaces, causing nasal congestion.
-
This question is part of the following fields:
- Physiology
-
-
Question 67
Correct
-
Which one of the following muscles is the most important muscle forming the pelvic floor?
Your Answer: Levator ani
Explanation:Levator ani muscle is composed of three different muscles i.e. iliococcygeus, pubococcygeus and the puborectalis muscle. It is the main muscle that supports the organs of the pelvic cavity.
Bulbocavernosus and Ischiocavernosus muscles are located in-between the anus and scrotum and play an important role in sexual response in males.
Superficial and deep transverse perineal muscles are located in the perinium and pass in front of the anus. -
This question is part of the following fields:
- Anatomy
-
-
Question 68
Incorrect
-
A 29-year-old lady comes to your clinic for a refill on her oral contraceptive tablets (Microgynon 30®). You discover she has a blood pressure of 160/100mmHg during your examination, which is confirmed by a second reading 20 minutes later. Her husband and she are expecting a child in six months. Which of the following recommendations is the best for her?
Your Answer: She should stop the OCP and be started on methyldopa for hypertension
Correct Answer: She should stop OCP, use condoms for contraception and reassess her blood pressure in 3 months
Explanation:Overt hypertension, developing in about 5% of Pill users, and increases in blood pressure (but within normal limits) in many more is believed to be the result of changes in the renin-angiotensin-aldosterone system, particularly a consistent and marked increase in the plasma renin substrate concentrations. The mechanisms for the hypertensive response are unclear since normal women may demonstrate marked changes in the renin system. A failure of the kidneys to fully suppress renal renin secretion could thus be an important predisposing factor.
These observations provide guidelines for the prescription of oral contraceptives. A baseline blood pressure measurement should be obtained, and blood pressure and weight should be followed at 2- or 3-month intervals during treatment. Oral contraceptive therapy should be contraindicated for individuals with a history of hypertension, renal disease, toxaemia, or fluid retention. A positive family history of hypertension, women for whom long-term therapy is indicated, and groups such as blacks, especially prone to hypertensive phenomena, are all relative contraindications for the Pill.
All other options are incorrect.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 69
Incorrect
-
All of the following statements are true regarding Turner's syndrome except?
Your Answer: Have raised FSH levels
Correct Answer: The streak ovaries should be removed surgically due to 25% tendency to be malignant
Explanation:Girls with Turner’s syndrome (45,X) are not at risk for malignancy. Patients with feminizing testicular syndrome with XY chromosome composition and patients with mixed gonadal dysgenesis are at risk for malignancy, and bilateral gonadectomy is performed.
-
This question is part of the following fields:
- Embryology
-
-
Question 70
Correct
-
A 32-year-old mother with a 9-year-old child is considering having a second child. Her first pregnancy was complicated by puerperal psychosis. Following electroconvulsive therapy (ECT), she promptly recovered and has been well until now. She is in excellent health and her husband has been very supportive. According to patient files, she was noted to be an excellent mother. What would be the most appropriate advice?
Your Answer: There is a 15-20% chance of recurrence of psychosis postpartum.
Explanation:Puerperal psychosis seems to be mainly hereditary and closely associated with bipolar disorder especially the manic type, rather than being a distinct condition with a group of classical symptoms or course. Postpartum psychoses typically have an abrupt onset within 2 weeks of delivery and may have rapid progression of symptoms. Fortunately, it is generally a brief condition and responds well to prompt management. If the condition is threatening the mother and/or baby’s safety, hospital admission is warranted. A patient can present with a wide variety of psychotic symptoms ranging from delusion, passivity phenomenon, catatonia, and hallucinations. While depression and mania may be the predominating features, it is not surprising to see symptoms such as confusion and stupor. Although the rate of incidence is about 1 in 1000 pregnancies, it is seen in about 20% of women who previously had bipolar episodes prior to pregnancy. It has not been shown to be linked with factors such as twin pregnancies, stillbirth, breastfeeding or being a single parent. However, it might be more commonly seen in women who are first-time mothers and pregnancy terminations.
The risk of recurrence is 20%. Unfortunately, there is no specific treatment guideline but organic causes should first be ruled out. First generation/typical anti-psychotics are often associated with extrapyramidal symptoms. Nowadays, atypical antipsychotics such as risperidone or olanzapine can be used along with lithium which is a mood stabiliser. As of now, there hasn’t been any significant side effects as a result of second generation antipsychotic use in pregnancy. While women are usually advised to stop breast-feeding, it might be unnecessary except if the mother is being treated with lithium which has been reported to cause side effects on the infants in a few instances. ECT is considered to be highly efficacious for all types of postpartum psychosis and may be necessary if the mother’s condition is life-threatening to herself or/and the baby. If untreated, puerperal psychosis might persist for 6 months or even longer.
The options of saying ‘in view of her age and previous problem, further pregnancies are out of the question’ and so is ‘By all means start another pregnancy and see how she feels about it. If she has misgivings, then have the pregnancy terminated.’ are inappropriate.
As mentioned earlier, considering there is a 20% chance of recurrence it is not correct to say that since she had good outcomes with her first pregnancy, the risk of recurrence is minimal.
Anti-psychotics are not recommended to be used routinely both during pregnancy and lactation due to the absence of long-term research on children with intrauterine and breastmilk exposure to the drugs. Hence it is not right to conclude that ‘if she gets pregnant then she should take prophylactic antipsychotics throughout the pregnancy’ as it contradicts current guidelines. Each case should be individualised and the risks compared with the benefits to decide whether anti-psychotics should be given during pregnancy. It is important to obtain informed consent from both the mother and partner with documentation.
Should the mother deteriorates during the pregnancy that she no longer is capable of making decisions about treatment, then an application for temporary guardianship should be carried out to ensure that she can be continued on the appropriate treatment.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 71
Incorrect
-
A 29 year old is diagnosed with stage 1A2 cervical cancer. Which of the following is the most appropriate treatment option?
Your Answer: Cryotherapy
Correct Answer: LLETZ
Explanation:The treatment of stage 1A cervical cancer is excision of the margins using the Loop electrical excision procedure (LLETZ). Hysterectomy is not necessary. This treatment enables fertility to be preserved.
2010 FIGO classification of cervical carcinoma
0 – Carcinoma in situ
1 – Confined to the cervix (diagnosed microscopy)
1A1 – Less than 3mm depth & 7mm lateral spread
1A2 – 3mm to 5mm depth & less than 7mm lateral spread
1B1 – Clinically visible lesion or greater than A2 & less than 4 cm in greatest dimension
1B2 – Clinically visible lesion, greater than 4 cm in greatest dimension
2 – Invades beyond uterus but not to pelvic wall or lower 1/3 vagina
2A1 – Involvement of the upper two-thirds of the vagina, without parametrical invasion & Less than 4cm
2A2 – Greater than 4 cm in greatest dimension
2B – Parametrial involvement
3 – Extends to Pelvic side wall or lower 1/3 vagina or hydronephrosis
3A – No pelvic side wall involvement
3B – Pelvic side wall involved or hydronephrosis
4 – Extends beyond true pelvis 4A Invades mucosa bladder and rectum
4B – Distant Metastasis -
This question is part of the following fields:
- Clinical Management
-
-
Question 72
Correct
-
A 23-year-old woman with diffuse pelvic pain and vaginal bleeding presents to the emergency room. She claims that it is around the time that she usually has her period. She has previously experienced defecation discomfort, dyspareunia, and dysmenorrhea. The patient claims that she has previously experienced similar symptoms, but that the agony has suddenly become unbearable. Her abdomen is soft, with normal bowel sounds and no rebound soreness, according to her physical examination. There is no costovertebral discomfort and the patient does not guard. Blood in the posterior vaginal vault, a closed os, and no palpable masses or cervical motion pain are all findings on her pelvic examination. What is the most likely diagnosis?
Your Answer: Endometriosis
Explanation:Endometriosis is defined as the presence of normal endometrial mucosa (glands and stroma) abnormally implanted in locations other than the uterine cavity. Approximately 30-40% of women with endometriosis will be sub fertile. About one third of women with endometriosis remain asymptomatic. When they do occur, symptoms, such as the following, typically reflect the area of involvement:
– Dysmenorrhea
– Heavy or irregular bleeding
– Pelvic pain
– Lower abdominal or back pain
– Dyspareunia
– Dyschezia (pain on defecation) – Often with cycles of diarrhoea and constipation
– Bloating, nausea, and vomiting
– Inguinal pain
– Pain on micturition and/or urinary frequency
– Pain during exercisePregnancy, appendicitis, ureteral colic and ruptured ectopic pregnancy all do not present with dysmenorrhea, pain on defecation and dyspareunia. Presence of a non tender, soft abdomen also rules out these conditions.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 73
Incorrect
-
The femoral triangle contains all of the following structures EXCEPT which one?
Your Answer: Saphenofemoral Junction
Correct Answer: Genital branch of the genitofemoral nerve
Explanation:The contents of the femoral triangles are femoral nerve, artery and the vein. Along with the femoral sheath and lymphatics.
-
This question is part of the following fields:
- Anatomy
-
-
Question 74
Incorrect
-
Which of the following factors causes the greatest increase in risk of developing bladder cancer?
Your Answer: Taking daily rosiglitazone
Correct Answer: Smoking
Explanation:Transitional cell carcinoma of the bladder is most commonly caused by cigarette smoke. Other risk factors include naphthylamine, azodyes and long term cyclophosphamide use.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 75
Incorrect
-
In which situation would you prescribe COCs?
Your Answer: A 38 year old woman with history of smoking
Correct Answer: A 20 year old woman with blood pressure 135/80mmHg
Explanation:Absolute contraindications to OCs include breast cancer, history of deep venous thrombosis or pulmonary embolism, active liver disease, use of rifampicin, familial hyperlipidaemia, previous arterial thrombosis, and pregnancy, while relative contraindications include smoking, age over 35, hypertension, breastfeeding, and irregular spontaneous menstruation.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 76
Correct
-
A 32-year-old woman at 33 weeks of gestation presents with vaginal bleeding. A pelvic ultrasound was done, which confirms the diagnosis of placenta praevia and you are planning a cesarean section as it is the most appropriate mode of delivery. Which among the following is considered a possible outcome of cesarean section delivery?
Your Answer: Increase risk of adhesions
Explanation:Obstetric complications during or following a cesarean section delivery include:
-Increased risk of maternal mortality.
-Increased need for cesarean sections in the subsequent pregnancies.
-Increased risk for damage to adjacent visceral organs especially bowels and bladder.
-Increased risk of infections.Increased risk for formation of adhesions is a complication after cesarean section and this is the correct response for the given question.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 77
Incorrect
-
A 66-year-old lady comes to your clinic complaining of a brownish vaginal discharge that has been bothering her for the previous three months. Atrophic vagina is seen on inspection. Which of the following diagnoses is the most likely?
Your Answer: Chlamydia infection
Correct Answer: Vaginal atrophy
Explanation:Endometrial cancer should always be the first diagnosis to rule out in a 65-year-old lady with brownish vaginal discharge. The inquiry focuses on the most likely source of the symptoms, rather than the most significant diagnosis to explore.
Blood typically causes the dark hue of vaginal discharge. The uterine cavity or the vagina can both be the source of bleeding. Only 5-10% of postmenopausal women with vaginal bleeding were found to have endometrial cancer. Around 60% of the women had atrophic vaginitis.Urogenital atrophy is caused by oestrogen insufficiency in postmenopausal women. Urogenital atrophy can cause the following symptoms:
– Dry vaginal skin
– Vaginal inflammation or burning
– Vaginal lubrication is reduced during sexual activity.
– Vulvar or vaginal pain, as well as dyspareunia (at the introitus or within the vagina)
– Vaginal or vulvar bleeding (e.g. postcoital bleeding. fissures)
– Vaginal discharge from the cervix (leukorrhea or yellow and malodorous)
– A vaginal bulge or pelvic pressure
– Symptoms of the urinary tract (e.g. urinary frequency, dysuria, urethral discomfort, haematuria). -
This question is part of the following fields:
- Gynaecology
-
-
Question 78
Incorrect
-
A 27-year-old pregnant woman visits to you at 17 weeks of gestation with complaint of eruption or rash, followed by a 2-day history of malaise, low grade fever and rhinorrhea. You suspect measles and order serology tests for her. Serology report shows that lgM against measles is positive with a negative lgG. Among the following which is the most appropriate next step in management of this case?
Your Answer: Administration of natural human immunoglobulin (NHIG) within 6 days
Correct Answer: Contact tracing
Explanation:The given case scenario describes a typical case of measles in a pregnant woman, which is confirmed by serologic studies. Positive lgM in serology is suggestive of acute infection, while a negative lgG confirms that the infection is in early phase without any seroconversion.
Conservative management of the symptoms and its potential complications is the only management plan therapeutically available after contracting measles. ‘Notification’ and contact tracing are the other very important issues to be considered.
Measles is a notifiable disease and healthcare professionals are mandated on reporting all the identified cases of measles to the authorized public health units. The main objective of this notification is to conduct a contact tracing.MMR vaccine is not useful once measles is contracted, as the vaccine is used for prevention of measles and as prophylaxis in post-exposure cases. For those with contact to a case of measles, MMR vaccine within 72 hours of contact may have a protective effect, but all measles-containing vaccines like MMR and MM RV are contraindicated throughout pregnancy even as prophylaxis.
As the circulating maternal antibodies will cross placenta and enters into the fetal circulation, a positive test does not confirm infection in the fetus. So serologic testing of the fetus is not useful.
NHIG is not useful in treating an established case of measles, as it is used as a post-measles exposure prophylactic for patients such as pregnant women, premature babies, etc who are contraindicated to MMR vaccine.
As both symptoms and lgM levels indicate measles infection, repeating measles-specific serologic test is not useful in this case. In general no test is indicated, unless its result has an impact on the further management of the case or any prognostic value.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 79
Correct
-
A 55-year-old female presents to her general practitioner. She complains of a three month history of amenorrhea, with recently added hot flushes 10 - 12 times a day, irritability and difficulty sleeping. What would be the best management strategy to relieve her symptoms, whilst minimising side effects?
Your Answer: Continuous daily oestrogen therapy, with medroxy progesterone acetate (MPA) given daily for 12 days each month.
Explanation:The best strategy is to commence cyclical hormone therapy using continuous daily oestrogen therapy, with medroxy progesterone acetate (MPA) given daily for 12 days each month.
This patient is most likely experiencing menopause, with symptoms caused by her oestrogen deficiency state.
Diazepam will help her to sleep and possibly alleviate her irritability, but would be unlikely to relieve the hot flushes.
Continuous therapy with oestrogen and MPA provides continuous progestogen therapy and has a high risk of causing unpredictable breakthrough vaginal bleeding, as it is only three months since the last menstrual period. This treatment is not recommended to be given within 1 – 2 years of the last period.
Oestrogen alone is not recommended for women who still have their uterus.
Progestogen alone would only be indicated in cases with contraindications to oestrogen administration.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 80
Correct
-
During wound healing collagen alignment along tension lines is part of which phase?
Your Answer: Remodelling
Explanation:Realignment of collagen is part of the remodelling phase. Remodelling is usually underway by week 3. Maximum tensile wound strength is typically achieved by week 12.
-
This question is part of the following fields:
- Physiology
-
-
Question 81
Correct
-
Question 82
Incorrect
-
Which of the following is the most common cause of maternal mortality?
Your Answer: Haemorrhage
Correct Answer: Cardiac disease
Explanation:The most common cause of maternal mortality is Cardiovascular deaths due to post partum bleeding followed by hypertensive disorders of pregnancy, sepsis and complications of labour.
-
This question is part of the following fields:
- Epidemiology
-
-
Question 83
Correct
-
A 30-year-old lady at 16 weeks of gestation who had histories of second-trimester pregnancy losses, presented with backache and pre-menstrual-like cramping along with increased vaginal discharge for the past one week. Pelvic examination shows that her cervix is dilated by 4 cm and effaced 80%. What will be the most likely diagnosis in this case?
Your Answer: Cervical insufficiency
Explanation:This woman has signs and symptoms suggestive of cervical insufficiency, whose clinical features include pelvic pressure, premenstrual-like cramping and backache with increased vaginal discharge. Usually these symptoms will persist for several days to weeks.
Cervical insufficiency is seen between 14 – 20 weeks of gestation, which is presented as soft effaced cervix, with minimal dilation on physical examination and a 4 cm dilated and more than 80% effaced cervix will be the clinical presentation in a more advanced case.Placental abruption presents with painful vaginal bleeding, whereas Placenta Previa presents as painless vaginal bleeding. Both cases will lead to shock but will not show any features of cervical insufficiency.
Anaemia, polyhydramnios, large for gestational age uterus and severe hyperemesis gravidarum are the commonly associated symptoms of a twin pregnancies.
New menstrual cycle after an abortion is expected to be presented with cervical dilation however signs of effacement will not be present along with it.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 84
Correct
-
Which immunoglobulin is the first to be synthesised by the neonate?
Your Answer: IgM
Explanation:Fetal production of immunoglobulin begins early on at about 10 weeks gestation with the production of IgM antibodies. Maternal IgG, which is a key component of fetal immunity is passed on to the foetus through the placenta from 12 weeks of gestation. Secretory IgA is not produced until after birth, through breast milk.
-
This question is part of the following fields:
- Immunology
-
-
Question 85
Incorrect
-
A woman visited the OPD with complaints of severe abdominal pain and light-headedness. There is history of fainting three days prior to consultation. She also has vaginal bleeding. In this case, which of the following investigations should be ordered to reach the diagnosis?
Your Answer: Beta HCG
Correct Answer:
Explanation:Testing for beta hCG should be the first test in this case. It will rule out any pregnancy that is strongly suspected based on the patient’s history and physical examination.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 86
Correct
-
A 48-year-old woman presented to you with a breast mass. On examination, it is hard, irregular and ill defined. The surface of the breast is slightly bruised however, there is no discharge. The most probable diagnosis is?
Your Answer: Fat necrosis
Explanation:Fat necrosis is often a result of a trauma or surgery. In fat necrosis the enzyme lipase releases fatty acids from triglycerides. The fatty acids combine with calcium to form soaps. These soaps appear as white chalky deposits which are firm lumps with no associated discharge. The given case has a bruise which indicates prior trauma.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 87
Correct
-
Which one of the following aetiological factors causes a reduction in the risk of fibroids?
Your Answer: Pregnancy
Explanation:Risk of fibroids is more common among African ethnicity and is also related to obesity and early puberty. The role of combined oral contraceptive pills is still debatable and its results are conflicting, whereas the risk of fibroids decreases with the increase in number of pregnancies. i.e. multiparous women have a lower risk of fibroids.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 88
Correct
-
Which one of the following factors commonly indicate repetitive late decelerations on cardiography (CTG)?
Your Answer: Fetal hypoxia
Explanation:Repetitive late decelerations can be caused by fetal hypoxia which results in constriction of the vessels to circulate blood from the peripheries to more important organs of the body like the brain and heart etc.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 89
Correct
-
Beta and Delta Thalassemia are associated with abnormalities to which chromosome
Your Answer: Chromosome 11
Explanation:Fetal haemoglobin (HBF) is the main haemoglobin type in the foetus and persists after birth for around 6 months. Fetal haemoglobin is composed of two alpha and two gamma subunits The alpha globulin chain is coded for by genes on Chromosome 16. Alpha Thalassemia are therefore associated with Chromosome16 defects The beta and delta globulin chains are coded for by genes on Chromosome 11. Beta and Delta Thalassemia are therefore associated with Chromosome 11 Defects
-
This question is part of the following fields:
- Endocrinology
-
-
Question 90
Correct
-
A patient asks you in clinic when she can start trying to conceive again. She has just completed chemotherapy for gestational trophoblastic disease (GTD)?
Your Answer: 1 year from completion of treatment
Explanation:According to the RCOG greentop guidelines, a women who have underdone chemotherapy for GTD are advised not to conceive for 1 years after completion of the chemotherapy.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 91
Correct
-
A 39-year-old woman who is 8 weeks pregnant presented to the medical clinic for consultation regarding the chance of her baby having Down syndrome. She mentioned that she has read somewhere that one of the risk factors for Down syndrome is advanced maternal age. She is concerned and asks if there are ways in which she can know whether her baby will be affected. Which of the following is considered as both the safest and the most accurate diagnostic tool for the exclusion of Down syndrome?
Your Answer: Amniocentesis at 16 weeks gestation
Explanation:Amniocentesis is a prenatal procedure performed on a pregnant woman to withdraw a small amount of amniotic fluid from the sac surrounding the foetus.
The goal of amniocentesis is to examine a small amount of this fluid to obtain information about the baby, including its sex, and to detect physical abnormalities such as Down syndrome or spina bifida.
Amniocentesis is only performed on women thought to be at higher risk of delivering a child with a birth defect.Amniocentesis is performed between 16 and 20 weeks into the pregnancy. By around this time, the developing baby is suspended in about 130ml of amniotic fluid, which the baby constantly swallows and excretes. A thin needle is used to withdraw a small amount of this fluid from the sac surrounding the foetus.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 92
Incorrect
-
Regarding placental anatomy:
Your Answer: The fetal side of the placenta is divided into 30-40 cotyledons
Correct Answer: Fetal blood vessels develop in the mesenchymal core of the chorionic villi
Explanation:The chorionic plate represents the fetal surface of the placenta, which in turn is covered by the amnion. The amnion is composed of a single layered epithelium and the amnionic mesenchyme, an avascular connective tissue. The amnionic mesenchyme is only weakly attached to the chorionic mesenchyme and can easily be removed from the delivered placenta. The chorionic mesenchyme contains the chorionic vessels that are continuous with the vessels of the umbilical cord. Within the mesoderm of secondary villi, haematopoietic progenitor cells develop and start to differentiate. At about day 20 post-conception, first placental blood cells and endothelial cells develop independent of the vascular system of the embryo proper.13 14 The development of first placental vessels transforms the respective villi into tertiary villi.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 93
Correct
-
Regarding ovarian cancer, which factors are thought to lower the risk?
Your Answer: Taking statins
Explanation:Ovarian cancer is a gynaecological cancer that commonly affects women over 40 years. Risk factors for ovarian cancer include: infertility, a family history of ovarian, breast or colorectal cancer. There are some protective factors, which include: high parity and breastfeeding, early age at menarche and late age at menopause, and combined oral contraceptives, and statins.
-
This question is part of the following fields:
- Epidemiology
-
-
Question 94
Incorrect
-
Among the following mentioned drugs, which one has reported the highest rate of congenital malformations if used in pregnancy?
Your Answer: Levetiracetam
Correct Answer: Sodium valproate
Explanation:Among all the antiepileptic drugs sodium valproate carries the highest teratogenicity rate. The potential congenital defects caused by sodium valproate are as below:
– Neural tube defects like spina bifida, anencephaly
– Cardiac complications like congenital ventricular septal defect, aortic stenosis, patent ductus arteriosus, aberrant pulmonary artery
– Limb defects like polydactyly were more than 5 fingers are present, oligodactyly were less than 5 fingers are present, absent fingers, overlapping toes, camptodactyly which is presented as a fixed flexion deformity of one or more proximal interphalangeal joints,split hand, ulnar or tibial hypoplasia.
– Genitourinary defects like hypospadias, renal hypoplasia, hydronephrosis, duplication of calyceal system.
– Brain anomalies like hydranencephaly, porencephaly, arachnoid cysts, cerebral atrophy, partial agenesis of corpus callosum, agenesis of septum pellucidum, lissencephaly of medial sides of occipital lobes, Dandy-Walker anomaly
– Eye anomalies like bilateral congenital cataract, optic nerve hypoplasia, tear duct anomalies, microphthalmia, bilateral iris defects, corneal opacities.
– Respiratory tract defects like tracheomalacia, lung hypoplasia,severe laryngeal hypoplasia, abnormal lobulation of the right lung, right oligemic lung which is presented with less blood flow.
– Abdominal wall defects like omphalocele
– Skin abnormalities capillary hemangioma, aplasia cutis congenital of the scalp. -
This question is part of the following fields:
- Obstetrics
-
-
Question 95
Correct
-
Which of the following increases the risk of endometrial hyperplasia?
Your Answer: Tamoxifen
Explanation:Tamoxifen increases risk of endometrial hyperplasia Aromatase inhibitors such as Letrozole and Anastrozole are not associated and have not been shown to increase the risk of endometrial pathology Whereas unopposed oestrogens increase endometrial cancer risk combined oral contraceptive decrease risk
-
This question is part of the following fields:
- Clinical Management
-
-
Question 96
Incorrect
-
How many days after fertilisation does the blastocyst hatch from the zone pellucida?
Your Answer: Oct-14
Correct Answer: 5-Jul
Explanation:Shortly after the morula enters the uterus, around the 4th day after fertilization, a clear cystic cavity starts forming inside the morula. The fluid passes through the zona pellucida from the uterine cavity and hence forms the blastocyst.
-
This question is part of the following fields:
- Embryology
-
-
Question 97
Correct
-
A patient undergoes oophorectomy and the ovarian veins are ligated. Which vein does the left ovary drain into?
Your Answer: Left renal
Explanation:The right ovarian vein ascends and enters the inferior vena cava and the left ovarian vein drains into the longer left renal vein.
-
This question is part of the following fields:
- Anatomy
-
-
Question 98
Incorrect
-
Which of the following statements regarding Management of Beta Thalassaemia in Pregnancy is not part of the RCOG guidelines?
Your Answer: All women with thalassaemia major should be receiving blood transfusions on a regular basis aiming for a pretransfusion haemoglobin of 100 g/l
Correct Answer: Folic acid 5 mg daily should be commenced 12 months prior to conception
Explanation:Women with Beta-Thalassaemia require significant extra input during pregnancy. Folic acid 5 mg daily should be commenced 3 months prior to conception in these patients. NOTE Women with thalassaemia who have undergone splenectomy OR have a platelet count >600 should continue or be commenced on Aspirin (75 mg/day)
-
This question is part of the following fields:
- Genetics
-
-
Question 99
Incorrect
-
You are reviewing a patient who is complaining of pain and numbness to the right anterior aspect of her labia following abdominal hysterectomy. You suspect ilioinguinal nerve injury. What spinal segment is the ilioinguinal nerve derived from?
Your Answer: L2,L3
Correct Answer: L1
Explanation:Ilioinguinal nerve injury is one of the most common nerve injuries associated with pelvic surgery.
-
This question is part of the following fields:
- Anatomy
-
-
Question 100
Correct
-
A baby with shoulder dystocia suffers a brachial plexus injury. You diagnose Erb-Duchenne palsy. Which nerve roots are typically affected?
Your Answer: C5 and C6
Explanation:Erb’s or Erb-Duchenne palsy is a type of brachial plexus injury. The brachial plexus comprises C5 to T1 nerve roots. In Erb’s palsy C5 and C6 are the roots primarily affected. Shoulder Dystocia is the most common cause of Erb’s palsy.
-
This question is part of the following fields:
- Clinical Management
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)