-
Question 1
Incorrect
-
A 30-year-old man reports experiencing a scratchy sensation in his eyes as the day goes on. He feels that his eyes become tired. These symptoms only occur during weekdays when he works as a computer programmer for a local business. During examination, there is mild conjunctival hyperemia, but the rest of the ocular examination is normal. Which nerve stimulation is linked to tear production?
Your Answer: Vagus nerve
Correct Answer: Intermediate nerve
Explanation:Cranial Nerves and Their Parasympathetic Functions
The cranial nerves play a crucial role in the parasympathetic nervous system, which is responsible for regulating various bodily functions. Here are some of the cranial nerves and their parasympathetic functions:
1. Intermediate Nerve: This nerve supplies secretomotor innervation to the lacrimal gland. The parasympathetic fibers originate from the geniculate ganglion of the facial nerve and travel through the greater petrosal nerve, deep petrosal nerve, Vidian nerve, and maxillary nerve to reach the lacrimal gland.
2. Oculomotor Nerve: The oculomotor nerve provides motor innervation to four of the six ocular muscles and parasympathetic innervation to the ciliary muscle and sphincter pupillae muscle of the iris.
3. Glossopharyngeal Nerve: This nerve provides secretomotor innervation to the parotid gland. The parasympathetic fibers travel through the tympanic branch of the glossopharyngeal nerve, tympanic plexus, lesser petrosal nerve, and auriculotemporal nerve to reach the parotid gland.
4. Vagus Nerve: The vagus nerve provides parasympathetic innervation to the heart, lung, and gastrointestinal tract.
5. Chorda Tympani: This branch of the facial nerve contains preganglionic parasympathetic fibers that synapse at the submandibular ganglion attached to the lingual nerve. The postganglionic parasympathetic fibers reach the submandibular and sublingual glands via the branches of the lingual nerve.
Understanding the parasympathetic functions of these cranial nerves is essential in diagnosing and treating various medical conditions.
-
This question is part of the following fields:
- Ophthalmology
-
-
Question 2
Correct
-
An 8-year-old boy arrives at the Emergency Department after falling on his outstretched hand. He is experiencing severe pain and cannot move his arm. An X-ray shows a fracture of the distal radius, along with dislocation of the distal radioulnar joint. The ulna appears to be intact. What is the most probable type of injury that this patient has suffered?
Your Answer: Galeazzi fracture-dislocation
Explanation:Common Fracture-Dislocations: Types and Characteristics
Fracture-dislocations are common injuries that occur due to falls or direct blows. Here are some of the most common types and their characteristics:
Galeazzi Fracture-Dislocation: This type of injury is most common in children and occurs when falling onto an outstretched hand with the elbow in flexion. It involves a radial shaft fracture with dorsal angulation, dislocation of the distal radioulnar joint, and radial shortening. Surgical fixation is required due to its instability.
Colles Fracture: This type of fracture occurs following a fall onto an outstretched hand and involves a fracture of the distal radius with dorsal angulation and impaction. There is no associated dislocation of the distal radioulnar joint.
Bankart Fracture: This type of fracture occurs as a complication of an anterior shoulder dislocation where the labrum and glenohumeral capsule/ligament are injured due to compression of the humeral head against the labrum. It is often seen with a Hill-Sachs lesion.
Monteggia Fracture-Dislocation: This type of injury involves a fracture of the ulnar shaft and dislocation of the radial head. It typically occurs following a fall onto an outstretched hand.
Smith’s Fracture: This type of fracture occurs due to a fall onto a flexed wrist or a direct blow to the back of the wrist. It involves a fracture of the distal radius with volar, not dorsal, angulation of the distal fragments.
In summary, fracture-dislocations are common injuries that require prompt medical attention and appropriate treatment to ensure proper healing and prevent long-term complications.
-
This question is part of the following fields:
- Trauma
-
-
Question 3
Incorrect
-
A 55-year-old man, with a history of moderate alcohol intake (20 units/week), presents with complaints of arthralgia and worsening erectile dysfunction over the past 6–9 months. On examination, he has a deep tan and evidence of chronic liver disease. The following investigations were conducted:
Investigation Result Normal value
Haemoglobin 145 g/l 135–175 g/l
White Cell Count 8.3 x 109/l 4–11 x 109/l
Platelets 164 x 109/l 150–400 x 109/l
Urea 6.0 mmol/l 2.5–6.5 mmol/l
Sodium 140 mmol/l 135–145 mmol/l
Potassium 4.2 mmol/l 3.5–5.0 mmol/l
Creatinine 95 μmol/l 50–120 µmol/l
Aspartate Aminotransferase (AST) 65 IU/l 10–40 IU/l
Alanine Aminotransferase (ALT) 82 IU/l 5–30 IU/l
Alkaline Phosphatase 135 IU/l 30–130 IU/l
Bilirubin 23 mmol/l 2–17 µmol/l
Lactate dehydrogenase (LDH) 326 IU/l 100–190 IU/l
Serum iron 45 μmol/l 0.74–30.43 μmol/l
Total iron-binding capacity 6.2 μmol/l 10.74–30.43 μmol/l
Ferritin 623 μg/ 20–250 µg/l
Glucose 8.8 mmol/l <7.0 mmol/l
What is the most likely diagnosis?Your Answer: Alcoholic cirrhosis
Correct Answer: Haemochromatosis
Explanation:Differential Diagnosis for a Patient with Iron Overload
A middle-aged man presents with skin discoloration, chronic liver disease, arthralgia, and erectile dysfunction. His serum ferritin level is significantly elevated at 623, indicating iron overload. However, liver disease can also cause an increase in serum ferritin.
Acute viral hepatitis is unlikely as his symptoms have been worsening over the past 6-9 months, and his transaminase levels are only moderately elevated. Alcoholic cirrhosis is also unlikely as his alcohol intake is modest.
Excess iron ingestion is a possibility, but it would require significant ingestion over a long period of time. Wilson’s disease, a recessively inherited disorder of copper metabolism, is also unlikely as it does not explain the symptoms of iron overload.
Overall, the differential diagnosis for this patient includes haemochromatosis, a genetic disorder that causes iron overload. Further testing and evaluation are necessary to confirm the diagnosis and determine the appropriate treatment plan.
-
This question is part of the following fields:
- Gastroenterology
-
-
Question 4
Incorrect
-
A 62-year-old man presents to the pre-admission clinic for assessment prior to an elective prostatectomy. You find no adverse past medical history and examination is unremarkable. An electrocardiogram (ECG) is indicated in all pre-operative patients undergoing major surgery who are over the age of 60. The ECG is shown below.
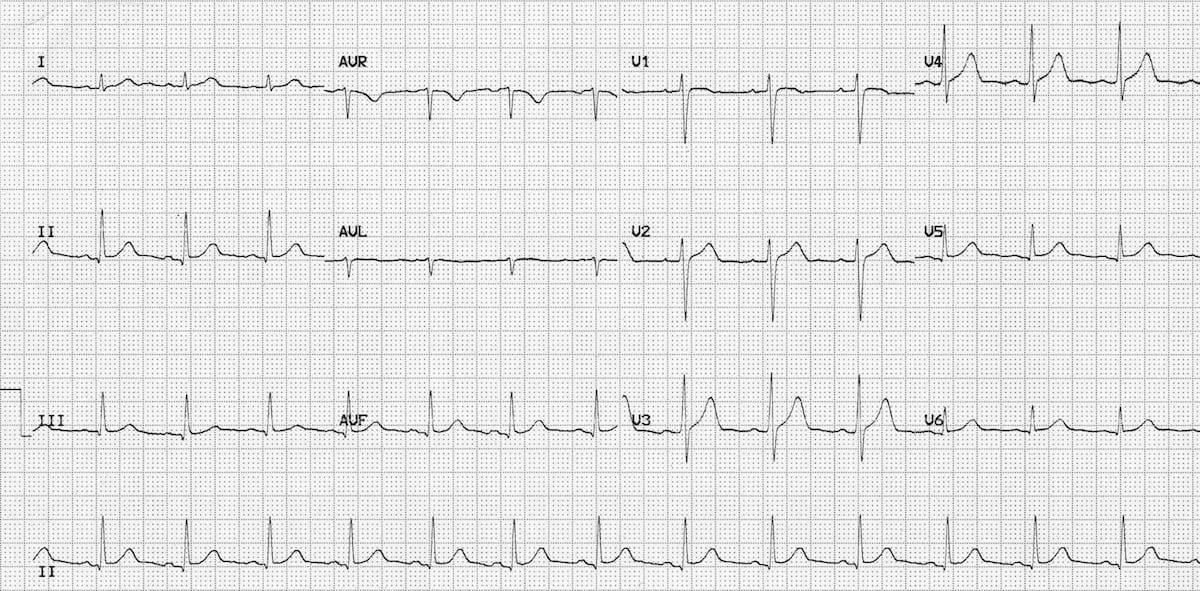 After having reviewed the ECG, what is the next best step to take with this patient?
After having reviewed the ECG, what is the next best step to take with this patient? Your Answer: Cancel the patient’s procedure as her current cardiac condition is too risky to proceed with major surgery
Correct Answer: No further assessment is required
Explanation:Assessing Cardiac Risk in Preoperative Patients: Common Misconceptions
There are several misconceptions when it comes to assessing cardiac risk in preoperative patients. One common mistake is assuming that all patients require extensive cardiac testing, even when there are no significant risk factors or symptoms present. For example, if a patient has no significant past medical history and their examination is unremarkable, an echocardiogram is not necessary.
On the other hand, some clinicians may be too cautious and cancel a patient’s procedure based on a perceived cardiac risk that is not supported by evidence. If the patient’s ECG is normal and there are no cardiac risk factors, cancelling the procedure would be unreasonable.
It is important to recognise that not all preoperative patients require extensive cardiac testing. Instead, clinicians should focus on identifying patients with specific cardiac conditions that require closer monitoring and management. By avoiding unnecessary testing and interventions, clinicians can improve patient outcomes and reduce healthcare costs.
-
This question is part of the following fields:
- Surgery
-
-
Question 5
Correct
-
A 42-year-old woman presents to her GP with concerns about symptoms that have been affecting her for several years but are now becoming more disruptive to her daily life. She has been experiencing obsessive thoughts about her loved ones being harmed and feels compelled to perform certain rituals to prevent this from happening. She spends hours each day checking and rechecking that appliances are turned off and doors are locked. Her relationships are suffering, and she is struggling to maintain her job. She is hesitant to take medication but is open to exploring other treatment options.
What is the most appropriate psychological approach for managing OCD in this case?Your Answer: Exposure response prevention (ERP) and cognitive behavioural therapy (CBT)
Explanation:Different Therapies for OCD: A Comparison
Obsessive-compulsive disorder (OCD) is a mental health condition that can be managed with various therapies. The most effective ones are exposure response prevention (ERP) and cognitive behavioural therapy (CBT), which are recommended by the National Institute for Health and Care Excellence (NICE). ERP involves exposing the patient to situations that trigger their compulsive behaviour while preventing them from acting on it. CBT, on the other hand, focuses on changing the patient’s thoughts, beliefs, and attitudes that contribute to their OCD.
Transactional analysis and psychoanalysis are not recommended for treating OCD as there is no evidence to support their use. Transactional analysis involves analysing social transactions to determine the ego state of the patient, while psychoanalysis involves exploring the unconscious to resolve underlying conflicts.
Counselling is also not appropriate for managing OCD as it is non-directive and does not provide specific coping skills.
Eye movement desensitisation and reprocessing (EMDR) is not effective for treating OCD either, as it is primarily used for post-traumatic stress disorder. EMDR combines rapid eye movement with cognitive tasks to help patients process traumatic experiences.
In conclusion, ERP and CBT are the most effective therapies for managing OCD, while other therapies such as transactional analysis, psychoanalysis, counselling, and EMDR are not recommended.
-
This question is part of the following fields:
- Psychiatry
-
-
Question 6
Correct
-
A 55-year-old man of black African origin presents to his GP for a review of his home blood pressure monitoring diary. The diary shows an average blood pressure of 140/90 mmHg, while his clinic reading today is 145/92 mmHg. The patient has a medical history of type two diabetes mellitus (T2DM) and takes metformin. He has no allergies and is not on any other medications. What is the best course of action for managing his blood pressure?
Your Answer: Prescribe losartan
Explanation:For black TD2M patients diagnosed with hypertension, the first-line antihypertensive should be an angiotensin II receptor blocker, such as Losartan. This is because ARBs are more effective at reducing blood pressure in black African or African-Caribbean patients with diabetes compared to ACE inhibitors. Amlodipine, bendroflumethiazide, and doxazosin are not recommended as first-line antihypertensives for this patient population. Thiazide-like diuretics are only used if blood pressure remains uncontrolled despite treatment with an ACE inhibitor or ARB and a calcium-channel blocker. Alpha-blockers are not used unless blood pressure is not controlled with multiple antihypertensive medications.
NICE updated its guidance on the management of type 2 diabetes mellitus (T2DM) in 2022, reflecting advances in drug therapy and improved evidence regarding newer therapies such as SGLT-2 inhibitors. The first-line drug of choice remains metformin, which should be titrated up slowly to minimize gastrointestinal upset. HbA1c targets should be agreed upon with patients and checked every 3-6 months until stable, with consideration for relaxing targets on a case-by-case basis. Dietary advice includes encouraging high fiber, low glycemic index sources of carbohydrates and controlling intake of foods containing saturated fats and trans fatty acids. Blood pressure targets are the same as for patients without type 2 diabetes, and antiplatelets should not be offered unless a patient has existing cardiovascular disease. Only patients with a 10-year cardiovascular risk > 10% should be offered a statin, with atorvastatin 20 mg as the first-line choice.
-
This question is part of the following fields:
- Medicine
-
-
Question 7
Correct
-
A 79-year-old man is admitted after a fall. On clinical examination, he is disorientated and appears neglected. He has a history of recurrent admissions after falls and infections. He lives alone and has severe dementia. Despite offers of assistance at home and suggestions to move to a care home, he has refused both. His daughter is worried about his safety and well-being. Which legal Act will be taken into account when deciding whether to move him to a care home?
Your Answer: Mental Capacity Act
Explanation:The Mental Capacity Act, passed in 2005, is a crucial legislation for healthcare professionals to understand. It upholds the principle that individuals over 16 years old have the right to make decisions about their life, including healthcare, as long as they meet certain criteria. Mental health disorders do not automatically mean a lack of capacity, and capacity can be reassessed over time. The Equality Act (2010) establishes equality duties for public sector bodies, while the Health and Social Care Act (2012) reformed the management and administration of the National Health Service, with Clinical Commissioning Groups allocating budgets for health services. The Mental Health Act (1983) guides healthcare professionals on when someone with a mental health disorder can be detained for their own and the public’s benefit. Finally, the Social Value Act (2012) requires policymakers to consider economic, environmental, and social factors when allocating public services contracts to promote the welfare of the population and reduce adverse impacts.
-
This question is part of the following fields:
- Ethics And Legal
-
-
Question 8
Correct
-
Among workers aged 18 to 30, which substance is most commonly associated with causing occupational accidents and injuries?
Your Answer: Alcohol
Explanation:Alcohol Consumption and Occupational Injuries
Workers who consume alcohol are almost twice as likely to experience an occupational injury compared to non-users. This is according to a study conducted by researchers who found that the personal and societal costs of even light and moderate drinking are significant. The study also revealed that most alcohol-related problems in the workplace are caused by light and moderate drinkers, not just those who drink on the job.
Aside from on-the-job drinking, heavy drinking outside of work also contributes to workplace problems. Hangover-related health issues such as an elevated risk of heart attacks, reduced cognitive abilities, and a psychiatric disorder called Elpenor syndrome, which is characterized by irrational behavior, are also associated with alcohol consumption.
In conclusion, alcohol consumption poses a significant risk to occupational safety and health. It is important for employers to implement policies and programs that promote responsible alcohol use and provide support for employees who may be struggling with alcohol-related issues.
-
This question is part of the following fields:
- Pharmacology
-
-
Question 9
Incorrect
-
A 29-year-old man visits his General Practitioner (GP) with complaints of painful red eye on one side. Upon examination, the GP observes reduced visual acuity, photophobia, eye watering, and a poorly reactive pupil. The patient is suspected to have uveitis. What is the most suitable course of action for managing this patient?
Your Answer: Chloramphenicol
Correct Answer: Same-day referral to an Ophthalmologist
Explanation:Management of Acutely Painful Red Eye with Suspected Uveitis
Explanation:
When a patient presents with an acutely painful red eye and suspected uveitis, it is crucial to refer them for same-day assessment by an Ophthalmologist. A slit-lamp examination is necessary to confirm the diagnosis, which cannot be performed by a GP. Non-infective anterior uveitis is treated with a combination of steroids and cycloplegics to reduce inflammation and ciliary spasm. In cases of infective uveitis, antimicrobials are also added.Chloramphenicol is used in the treatment of conjunctivitis, but it is not appropriate for uveitis. Conservative management with pain relief alone is not sufficient for this condition. Topical steroids are required to reduce inflammation, along with a cycloplegic such as atropine to reduce ciliary spasm. However, topical steroids should not be initiated in primary care, and patients require urgent assessment in secondary care.
Referral within two weeks is not appropriate for a patient with an acutely painful red eye and suspected uveitis. Any delay in treatment can result in adhesions within the eye and long-term damage. Therefore, same-day referral to an Ophthalmologist is necessary for prompt diagnosis and treatment.
-
This question is part of the following fields:
- Ophthalmology
-
-
Question 10
Correct
-
A 32-year-old woman presents with a sudden-onset, severe, sharp, colicky pain in the right iliac fossa, radiating to the right loin and her right labia. Her last menstrual period was two weeks ago.
Which of the following would be most useful as an initial investigation?Your Answer: Urine dipstick
Explanation:Medical Procedures and Conditions: A Brief Overview
Urine Dipstick
In cases of suspected renal colic, a urine dipstick should be performed to support the diagnosis and rule out a urinary tract infection. Microscopic haematuria is a common indicator of renal stones.
Diagnostic Peritoneal Lavage (DPL)
DPL is a surgical diagnostic procedure used to detect free-floating fluid in the abdominal cavity, usually blood. It is now performed less frequently due to the increased use of other imaging modalities such as FAST and CT.
Blood Sugar Levels
Hypoglycaemia symptoms occur when blood sugar levels fall below 4 mmol/l. Symptoms include hunger, trembling, sweating, confusion, and difficulty concentrating. However, the history provided does not suggest hypoglycaemia or diabetes.
Rectal Examination
Digital rectal examination is commonly used to assess the prostate, detect rectal bleeding, and investigate constipation, changes in bowel habit, and problems with urinary or faecal continence. In exceptional circumstances, it may be used to detect the uterus and cervix.
Vaginal Examination
Speculum vaginal examination is commonly used to diagnose pregnancy, assess gestational age, detect abnormalities in the genital tract, investigate vaginal discharge, examine the cervix, and take cervical cytology smears.
Urinary Tract Infections (UTIs)
UTIs are caused by the presence of bacteria in the urinary tract and can affect the bladder, prostate, or kidneys. Escherichia coli is the most common cause. Abacterial cystitis, or the urethral syndrome, is a type of UTI that does not involve bacteriuria. Complicated and uncomplicated UTIs are differentiated by the presence or absence of renal tract and function abnormalities.
Overview of Common Medical Procedures and Conditions
-
This question is part of the following fields:
- Urology
-
-
Question 11
Incorrect
-
Which death requires a report to be made to the coroner?
Your Answer: A 73-year-old female who had undergone a hip replacement two months previously presents with severe chest pain and breathlessness. She is diagnosed with pulmonary embolism but dies.
Correct Answer: A 69-year-old male with pneumoconiosis is admitted with fever and breathlessness. He dies two days later from pneumonia.
Explanation:Reporting Deaths to the Coroner
Pneumoconiosis is an occupational lung disease that may entitle the family to compensation if it has caused a reduction in the length or quality of life. In the UK, all deaths related to asbestos or pneumoconiosis should be reported to the coroner. It is the duty of the Registrar of Births, Deaths and Marriages to report a death to the coroner, but doctors should also be aware of the circumstances that require reporting. These include unknown causes of death, violent or unnatural deaths, deaths due to accidents, self-neglect or neglect by others, industrial illnesses or employment-related deaths, deaths due to abortion, deaths during or after an operation, suicides, deaths in police custody, and deaths due to acute intoxication.
Regarding deaths due to neglect, it is important to note that the fifth option does not necessarily require reporting to the coroner. When a patient dies, the paperwork asks whether they had an operation within the last year of life and whether it had a direct effect on shortening their life. Cases where a pulmonary embolism occurs two months after a procedure, for example, must be assessed individually to determine whether it is directly related to the operation. It is increasingly important to appropriately report deaths, particularly in light of recent inquiries and legislation.
-
This question is part of the following fields:
- Miscellaneous
-
-
Question 12
Correct
-
Which scenario results in a violation of an individual's autonomy?
Your Answer: An older man whose physician and family coerce him into having foot surgery
Explanation:The Importance of Autonomy in Medical Decision Making
Autonomy is the principle that individuals have the right to make decisions for themselves and be self-governing. In the context of medical decision making, this means that patients have the right to refuse medical procedures even if it may be in their best interests. It is important for doctors and relatives to respect this right and not coerce the patient into undergoing the procedure.
While it may be difficult for doctors and relatives to accept a patient’s refusal of a procedure, it is crucial to remember that autonomy is a fundamental principle in medical ethics. Patients have the right to make decisions about their own bodies and healthcare, and it is not up to others to make those decisions for them. It is the responsibility of healthcare providers to provide patients with all the necessary information to make informed decisions about their care.
In conclusion, autonomy is a vital aspect of medical decision making. Patients have the right to make decisions for themselves, and it is important for healthcare providers to respect and uphold this right. By doing so, patients can feel empowered and in control of their own healthcare, leading to better outcomes and a more positive healthcare experience.
-
This question is part of the following fields:
- Miscellaneous
-
-
Question 13
Correct
-
A 25-year-old female has been suffering from myalgias, pleural effusion, pericarditis, and arthralgias without any joint deformity for a few years now. What would be the most suitable next step in investigating her condition?
Your Answer: Anti-nuclear antibody
Explanation:The role of anti-nuclear antibody (ANA) in diagnosing systemic lupus erythematosus (SLE) is crucial. When a patient presents with symptoms such as polyarthropathy, myalgia, pericarditis, and effusions, SLE is often the suspected diagnosis. To confirm this, doctors may use a test called ANA.
However, ANA can also be positive in other autoimmune diseases such as scleroderma, Sjogren’s syndrome, Raynaud’s disease, juvenile chronic arthritis, RhA antiphospholipid antibody syndrome, and autoimmune hepatitis. If the ANA test is negative, it is unlikely that the person has SLE.
It is important to note that ANAs are present in approximately 5% of the normal population, usually in low titres, and these individuals have no disease. Titres of lower than 1:80 are less likely to be significant, and even higher titres are insignificant with aging over age 60 years. Therefore, doctors must interpret ANA results in the context of the patient’s symptoms and medical history to make an accurate diagnosis.
-
This question is part of the following fields:
- Clinical Sciences
-
-
Question 14
Incorrect
-
A 50-year-old woman presents to the surgical assessment unit with worsening upper right abdominal pain after dining out with friends. She reports experiencing this pain for the past few months, but it has never been this severe. The pain tends to worsen after dinner, especially with fast food, and occasionally radiates to her right shoulder. Upon examination, you note an increase in body weight. Her abdomen is soft and non-tender, and bowel sounds are present. She is currently not running a fever. What is the definitive treatment for this condition?
Your Answer: Elective ERCP
Correct Answer: Elective laparoscopic cholecystectomy
Explanation:Elective laparoscopic cholecystectomy is the preferred treatment for biliary colic.
Biliary colic is typically characterized by worsening pain after eating, but the patient is generally in good health, has no fever, and has a soft abdomen. In contrast, cholecystitis is associated with signs of infection, such as fever and tachycardia, and may involve palpable gallbladder and positive Murphy’s sign. If the patient is clinically stable and a good candidate for surgery, elective cholecystectomy is the appropriate management option. Cholecystostomy is reserved for cases of acute cholecystitis with pus accumulation, while ERCP is used to remove obstructing gallstones in patients with jaundice or risk of ascending cholangitis. MRCP is a diagnostic tool and not a treatment option.
Biliary colic is a condition that occurs when gallstones pass through the biliary tree. The risk factors for this condition are commonly referred to as the ‘4 F’s’, which include being overweight, female, fertile, and over the age of forty. Other risk factors include diabetes, Crohn’s disease, rapid weight loss, and certain medications. Biliary colic occurs due to an increase in cholesterol, a decrease in bile salts, and biliary stasis. The pain associated with this condition is caused by the gallbladder contracting against a stone lodged in the cystic duct. Symptoms include right upper quadrant abdominal pain, nausea, and vomiting. Diagnosis is typically made through ultrasound. Elective laparoscopic cholecystectomy is the recommended treatment for biliary colic. However, around 15% of patients may have gallstones in the common bile duct at the time of surgery, which can result in obstructive jaundice. Other possible complications of gallstone-related disease include acute cholecystitis, ascending cholangitis, acute pancreatitis, gallstone ileus, and gallbladder cancer.
-
This question is part of the following fields:
- Surgery
-
-
Question 15
Incorrect
-
A 45-year-old man has been admitted to hospital for pain management. The patient has metastatic lung cancer and is undergoing palliative radiotherapy. He received his last dose of analgesia 3 hours ago. On inspection, the patient is obtunded and has constricted pupils and a respiratory rate of 6 breaths per minute.
Which analgesia is the patient most likely to have received to cause this adverse reaction?Your Answer: Haloperidol
Correct Answer: Oxycodone
Explanation:Oxycodone is a strong synthetic opioid pain reliever that affects the brain’s respiratory and breathing centers. Overdose symptoms, known as the opiate triad, include pinpoint pupils, unconsciousness, and respiratory depression. Combining opioids with alcohol or sedatives increases the risk of respiratory depression and death. Naloxone can reverse the effects of an opiate overdose if administered promptly. Phenobarbital, an older anti-epileptic drug, can cause sedation and dilated pupils but is not used to treat lung cancer pain. Amitriptyline can cause sedation, but pupils will be dilated. Diazepam, an anxiolytic, can cause sedation and dilated pupils. Haloperidol, commonly used for end-of-life nausea, may cause pupil constriction but is less likely to cause respiratory depression.
-
This question is part of the following fields:
- Pharmacology
-
-
Question 16
Correct
-
You are on call overnight for orthogeriatrics when you receive a bleep to see a patient who is two days post-op from a left total hip replacement. You are not familiar with this patient. Upon arrival, you notice that the patient is drowsy and confused, and has a very fast heart rate. An electrocardiogram (ECG) reveals peaked T-waves, a PR interval of 230 ms, and a wide QRS. The patient's potassium level on ABG is 6.4 mmol. What is the most appropriate initial management?
Your Answer: Give calcium gluconate 10% 10 ml by slow iv injection
Explanation:Managing Hyperkalaemia: Immediate Treatment Steps
Hyperkalaemia is a serious condition that requires immediate treatment. The first step is to administer 10 ml of 10% calcium gluconate by slow IV injection to protect the cardiac myocytes from excess potassium. Next, 10 Units of Actrapid should be given in 100 ml of 20% glucose to draw potassium intracellularly. Salbutamol nebulisers can also be used. Finally, calcium resonium 15g orally or 30 g rectally can be given to mop up excess potassium in the gastrointestinal tract. It is important to note that this condition is life-threatening and requires immediate management, so waiting for a registrar is not an option.
-
This question is part of the following fields:
- Acute Medicine And Intensive Care
-
-
Question 17
Correct
-
A 50-year-old man comes to the Gastroenterology Clinic with a 6-month history of rectal bleeding, altered bowel habit and weight loss. Given his strong family history of colorectal cancer, the physician wants to investigate and rule out this diagnosis.
What would be the most suitable investigation to perform in a patient with suspected colorectal cancer?Your Answer: Colonoscopy
Explanation:Diagnostic Tools for Colorectal Cancer
Colorectal cancer is a prevalent malignancy in the western world, with symptoms varying depending on the location of the cancer within the intestinal tract. Colonoscopy is currently the preferred diagnostic tool for young, otherwise healthy patients. Management decisions are made after multidisciplinary team discussions, with surgical removal of the tumor being a common approach. Preoperative radiotherapy may be used to shrink tumors, and post-operative adjuvant chemotherapy can improve survival rates. Other diagnostic tools include endorectal ultrasound for staging rectal cancers, pelvic MRI for detailed staging and operative planning, and CT colonography as a sensitive diagnostic test when colonoscopy is high risk or incomplete. However, CT colonography cannot take biopsies or remove polyps. While raised CEA levels may indicate colorectal cancer, they can also be elevated for other reasons, and normal levels do not rule out the possibility of cancer.
-
This question is part of the following fields:
- Colorectal
-
-
Question 18
Correct
-
A 68-year-old man with known bronchial carcinoma presents to hospital with confusion. A computed tomography (CT) scan of the brain was reported as normal: no evidence of metastases. His serum electrolytes were as follows:
Investigation Result Normal value
Sodium (Na+) 114 mmol/l 135–145 mmol/l
Potassium (K+) 3.9 mmol/l 3.5–5.0 mmol/l
Urea 5.2 mmol/l 2.5–6.5 mmol/l
Creatinine 82 μmol/l 50–120 µmol/l
Urinary sodium 54 mmol/l
Which of the subtype of bronchial carcinoma is he most likely to have been diagnosed with?Your Answer: Small cell
Explanation:Different Types of Lung Cancer and Their Association with Ectopic Hormones
Lung cancer is a complex disease that can be divided into different types based on their clinical and biological characteristics. The two main categories are non-small cell lung cancers (NSCLCs) and small cell lung cancer (SCLC). SCLC is distinct from NSCLCs due to its origin from amine precursor uptake and decarboxylation (APUD) cells, which have an endocrine lineage. This can lead to the production of various peptide hormones, causing paraneoplastic syndromes such as the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) and Cushing syndrome.
Among NSCLCs, squamous cell carcinoma is commonly associated with ectopic parathyroid hormone, leading to hypercalcemia. Large cell carcinoma and bronchoalveolar cell carcinoma are NSCLCs that do not produce ectopic hormones. Adenocarcinoma, another type of NSCLC, also does not produce ectopic hormones.
Understanding the different types of lung cancer and their association with ectopic hormones is crucial for proper management and treatment of the disease.
-
This question is part of the following fields:
- Respiratory
-
-
Question 19
Correct
-
A father attends his GP to discuss concerns he has about his 12-year-old daughter. Since the age of three, she has had a lot of routines, such as how she organizes her toys and which way she walks to school, and is very rigid about following them. She does not cope at all well with changes to the routine. She struggles to make friends and seems very uncomfortable in social situations. Apart from going to school, she avoids meeting children; she has been to a few birthday parties, but she was very clingy to her father and demanded to be taken home after a few minutes. On examination, the GP is unable to build a rapport with the girl, as she refuses to speak and will not maintain eye contact. She appears fidgety and gets up and down out of her chair on several occasions to try and leave the room. You suspect a diagnosis but advise her father that more assessment will be needed to confirm a diagnosis.
The sign to support the diagnosis is the child's rigid adherence to routines and difficulty coping with changes to the routine, as well as their struggles with social situations and avoidance of meeting other children.Your Answer: Less than ten spoken words by age two years
Explanation:Developmental Milestones and Red Flags in Early Childhood
By the age of two years, children should be using 50 or more words. If they do not meet this milestone, there may be a social, speech or hearing issue that needs to be assessed by a paediatric team. Lack of spoken words could be a sign of autistic spectrum disorder (ASD).
A lack of social smile by age three months is considered abnormal and could indicate a social, visual, or cognitive problem. However, it may also signal ASD in some cases.
Parallel play is normal behavior for two-year-olds. They will happily play next to each other but rarely play with each other. It isn’t until the age of three when they usually start to involve other children in playing.
Separation anxiety from parents or carers at age ten months is normal behavior. Children can become upset if they are not with their parents or carer until the new person becomes more familiar to them, usually between the ages of six months and three years.
Temper tantrums at age 18 months are normal behavior. However, if these tantrums persist into later childhood, it could indicate a social or developmental problem.
-
This question is part of the following fields:
- Paediatrics
-
-
Question 20
Incorrect
-
A 15-year-old Scottish resident presents to your Scottish Emergency Department with a 10-hour history of acute right-sided abdominal pain. On examination, she has acute appendicitis. She is keen to proceed with the recommended surgery. You are unable to contact a parent or any other contact given by the patient.
What do you need in order to proceed?Your Answer: A court order; the patient is not able to consent, and it is not possible to contact a responsible person
Correct Answer: Nothing; in Scotland, a 16-year-old person is deemed capable of consenting to treatment
Explanation:Capacity to Consent to Treatment in Scotland for 16-Year-Olds
In Scotland, the Age of Legal Capacity (Scotland) Act 1991 states that all people aged 16 and over are presumed in law to have the capacity to consent to treatment unless there is evidence to the contrary. This means that a 16-year-old person is deemed capable of consenting to treatment without the need for a court order or assessment of competence.
Furthermore, social workers do not have the power to consent on behalf of any patient, regardless of age. It is important to note that even if it is believed to be in the best interests of the person to have the surgery performed, it cannot be done without their consent if they are over 16 and have capacity.
Overall, the law in Scotland is clear regarding the age at which a person is deemed to have capacity to consent, providing clarity and protection for 16-year-olds seeking medical treatment.
-
This question is part of the following fields:
- Ethics And Legal
-
-
Question 21
Incorrect
-
What is the supply of the inferior mesenteric artery?
Your Answer: The last two thirds of the rectum
Correct Answer: From the splenic flexure to the first third of the rectum
Explanation:Arterial Supply to the Digestive Tract
The digestive tract is supplied by three main arteries: the coeliac axis, the superior mesenteric artery, and the inferior mesenteric artery. The coeliac axis supplies the liver and stomach, as well as the oesophagus to the first half of the duodenum. The superior mesenteric artery supplies the second half of the duodenum to the first two thirds of the transverse colon. The inferior mesenteric artery supplies the last third of the transverse colon to the first third of the rectum. Finally, the middle rectal artery supplies the last two thirds of the rectum.
It is important to note that the greater curvature of the stomach is supplied by branches of the splenic artery, which itself comes from the coeliac axis. the arterial supply to the digestive tract is crucial for medical professionals in diagnosing and treating various gastrointestinal conditions.
-
This question is part of the following fields:
- Clinical Sciences
-
-
Question 22
Incorrect
-
You arrive with the ambulance crew to the scene of a high-energy road traffic accident involving a 30-year-old man. He has an open fracture of his right femur and is unconscious. He appears to be struggling to breathe. On initial observation, you see a large pool of blood gathered around his abdomen coming from a wide wound.
Which of the following is the first step in his immediate management?Your Answer: Undress the patient to assess the wounds and then cover with blankets to prevent hypothermia
Correct Answer: Apply pressure to the abdominal wound to minimise bleeding
Explanation:Prioritizing Medical Interventions in Trauma Cases
In cases of trauma, it is crucial to prioritize medical interventions in order to save the patient’s life. The
ABCDE approach is commonly used, with standing for catastrophic bleeding. If there is evidence of catastrophic bleeding, it must be addressed immediately to minimize blood loss. Once bleeding is under control, the airway must be secured and breathing must be managed. In cases where the patient is unconscious, C-spine immobilization is necessary. Assessment of wounds and exposure of the patient should only be done after the primary survey is completed. Fluid resuscitation through two large-bore cannulae is necessary to stabilize the patient’s condition. However, this should only be done after the airway and breathing have been assessed and managed.
While morphine may provide pain relief, it presents a risk of sedation and respiratory depression. Therefore, it should not be administered until the patient’s breathing is stable. By prioritizing medical interventions in trauma cases, healthcare professionals can increase the chances of saving the patient’s life.
-
This question is part of the following fields:
- Trauma
-
-
Question 23
Correct
-
You are requested to evaluate a 28-year-old patient in a joint medical/obstetric clinic who has recently been diagnosed with gestational diabetes. Her pregnancy has been complicated by a diagnosis of gestational diabetes through routine screening and she now takes metformin 500 mg three times a day.
She is currently 26 weeks pregnant and has just undergone a scan that revealed an estimated foetal weight of 900g (99th percentile). She reports feeling well and has been tolerating the metformin without any issues. A fasting blood glucose level is taken at the clinic and compared to her previous results:
6 weeks ago: 6.0mmol/L
4 weeks ago: 6.1 mmol/L
Today: 7.5mmol/L
Based on the above information, what changes would you make to the management of this patient?Your Answer: Continue metformin and add insulin
Explanation:If blood glucose targets are not achieved through diet and metformin in gestational diabetes, insulin should be added to the treatment plan. This patient was initially advised to make lifestyle changes and follow a specific diet for two weeks, as her fasting blood glucose was below 7 mmol/L. However, since she did not meet the targets, she was started on metformin monotherapy. Insulin therapy was not initiated earlier because her fasting blood glucose was below 7 mmol/L. According to NICE guidelines, if metformin monotherapy fails to achieve the desired results, insulin should be started, and lifestyle changes should be emphasized. Therefore, the correct answer is to continue metformin and add insulin to the patient’s treatment plan. The other options, such as increasing the dose of metformin, stopping metformin and starting insulin, adding gliclazide, or prescribing high-dose folic acid, are incorrect.
Gestational diabetes is a common medical disorder affecting around 4% of pregnancies. Risk factors include a high BMI, previous gestational diabetes, and family history of diabetes. Screening is done through an oral glucose tolerance test, and diagnostic thresholds have recently been updated. Management includes self-monitoring of blood glucose, diet and exercise advice, and medication if necessary. For pre-existing diabetes, weight loss and insulin are recommended, and tight glycemic control is important. Targets for self-monitoring include fasting glucose of 5.3 mmol/l and 1-2 hour post-meal glucose levels.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 24
Correct
-
A 45-year-old patient presents to their GP with a 3-month history of worsening dyspepsia, epigastric pain, and drenching night sweats on a background of recurrent gastric ulcers. The GP urgently refers the patient for investigation. Following a gastroscopy with biopsies taken, a low grade gastric MALT lymphoma is diagnosed, and the presence of H. pylori was also noted on the biopsy report. The patient has no significant past medical history. What treatment plan is the doctor likely to recommend?
Your Answer: Omeprazole, amoxicillin and clarithromycin
Explanation:The recommended treatment for gastric MALT lymphoma associated with H. pylori infection is a combination of omeprazole, amoxicillin, and clarithromycin. This is because the majority of cases are linked to H. pylori, as suggested by the patient’s history of gastric ulcers. Low-grade cases can be treated with H. pylori eradication alone, but high-grade or atypical cases may require chemotherapy and/or radiotherapy. The answer choice of lansoprazole, clarithromycin, and doxycycline is incorrect, as doxycycline is not used in H. pylori eradication. Active monitoring may be an option in some cases, but when a clear cause like H. pylori is identified, treatment is recommended. Partial gastrectomy is not a standard treatment for gastric MALT lymphoma.
Gastric MALT Lymphoma: A Brief Overview
Gastric MALT lymphoma is a type of lymphoma that is commonly associated with H. pylori infection, which is present in 95% of cases. The good news is that this type of lymphoma has a good prognosis, especially if it is low grade. In fact, about 80% of patients with low-grade gastric MALT lymphoma respond well to H. pylori eradication.
One potential feature of gastric MALT lymphoma is the presence of paraproteinaemia, which is an abnormal protein in the blood. However, this is not always present and may not be a reliable indicator of the disease. Overall, gastric MALT lymphoma is a treatable form of lymphoma with a high likelihood of successful treatment.
-
This question is part of the following fields:
- Surgery
-
-
Question 25
Correct
-
A 76-year-old man comes to his doctor complaining of difficulty speaking, swallowing, and experiencing sudden emotional outbursts of laughter or tears. Upon examination, the doctor observes a spastic tongue, an exaggerated jaw jerk, normal gag reflex, and bilateral upper motor neuron signs. What is the most probable diagnosis?
Your Answer: Pseudobulbar palsy
Explanation:Understanding Pseudobulbar Palsy: Symptoms, Causes, and Differential Diagnosis
Pseudobulbar palsy is a neurological condition that results from lesions in the corticobulbar pathways connecting the cortex to the brainstem. This article aims to provide a comprehensive understanding of pseudobulbar palsy, including its symptoms, causes, and differential diagnosis.
Symptoms of Pseudobulbar Palsy
Patients with pseudobulbar palsy may experience emotional lability, difficulty swallowing, and spastic dysarthria, which can cause a husky or gravelly voice. On examination, patients may exhibit an exaggerated jaw jerk, weak muscles of mastication, a spastic immobile tongue, and bilateral upper motor neuron signs.Causes of Pseudobulbar Palsy
Pseudobulbar palsy can occur due to demyelination, such as in multiple sclerosis, motor neuron disease, and bilateral cerebrovascular disease. Other causes include traumatic brain injury, brain tumors, and infections.Differential Diagnosis
It is important to differentiate pseudobulbar palsy from other neurological conditions that may present with similar symptoms. For example, a frontal lobe tumor can cause emotional lability and personality changes, but it would not explain the bilateral upper motor neuron signs and voice changes seen in pseudobulbar palsy. Bulbar palsy, on the other hand, is caused by lower motor neuron disturbance and presents with nasal speech and tongue fasciculations, absent gag reflex, and lower motor neuron signs. Cerebellar infarcts and Huntington’s disease can also present with speech and motor impairments, but they have distinct clinical features that differentiate them from pseudobulbar palsy.Conclusion
Pseudobulbar palsy is a neurological condition that can cause emotional lability, difficulty swallowing, and spastic dysarthria. It is important to consider this diagnosis in patients presenting with these symptoms and to differentiate it from other neurological conditions that may have similar presentations. Early diagnosis and management can improve patient outcomes and quality of life. -
This question is part of the following fields:
- Neurology
-
-
Question 26
Incorrect
-
A 55-year-old man presents to the emergency department with complaints of severe diarrhoea and vomiting for the past week. During his initial assessment, an ECG is performed, which reveals a polymorphic ventricular tachycardia. His blood pressure is 120/70 mmHg, heart rate is 82 bpm, and GCS is 15/15. Routine blood tests are conducted, and the results are as follows:
- Sodium: 136 mmol/L (135 - 145)
- Potassium: 4 mmol/L (3.5 - 5.0)
- Bicarbonate: 24 mmol/L (22 - 29)
- Magnesium: 0.4 mmol/L (0.7-1.0)
- Urea: 6 mmol/L (2.0 - 7.0)
- Creatinine: 120 µmol/L (55 - 120)
What would be the initial management plan for this patient?Your Answer: Adenosine
Correct Answer: IV magnesium
Explanation:In cases of hypomagnesaemia, particularly if the patient’s magnesium levels are below 0.4 mmol/L or if they are experiencing symptoms such as tetany, arrhythmias, or seizures, IV magnesium is typically administered. This is the appropriate course of action for a patient who has presented with severe vomiting and diarrhea, as well as polymorphic ventricular tachycardia, as it is likely that their gastrointestinal losses have resulted in hypomagnesaemia, which has in turn led to torsades des pointes.
Understanding Hypomagnesaemia: Causes, Symptoms, and Treatment
Hypomagnesaemia is a condition characterized by low levels of magnesium in the blood. There are several causes of this condition, including the use of certain drugs such as diuretics and proton pump inhibitors, total parenteral nutrition, and chronic or acute diarrhoea. Alcohol consumption, hypokalaemia, hypercalcaemia, and metabolic disorders like Gitelman’s and Bartter’s can also lead to hypomagnesaemia. The symptoms of this condition may be similar to those of hypocalcaemia, including paraesthesia, tetany, seizures, and arrhythmias.
When the magnesium level drops below 0.4 mmol/L or when there are symptoms of tetany, arrhythmias, or seizures, intravenous magnesium replacement is commonly given. An example regime would be 40 mmol of magnesium sulphate over 24 hours. For magnesium levels above 0.4 mmol/L, oral magnesium salts are prescribed in divided doses of 10-20 mmol per day. However, diarrhoea can occur with oral magnesium salts. It is important to note that hypomagnesaemia can exacerbate digoxin toxicity.
-
This question is part of the following fields:
- Pharmacology
-
-
Question 27
Correct
-
You are the surgical FY1 discussing with a patient in her 50s about her upcoming vaginal hysterectomy with antero-posterior repair. What is a potential long-term complication of this procedure?
Your Answer: Vaginal vault prolapse
Explanation:Long-Term Complications of Vaginal Hysterectomy
Vaginal hysterectomy with antero-posterior repair is a common surgical procedure for women. However, it may lead to long-term complications such as enterocoele and vaginal vault prolapse. These conditions occur when the pelvic organs shift and push against the vaginal wall, causing discomfort and pain. While urinary retention may occur immediately after the surgery, it is not typically a chronic complication.
It is important for women who undergo vaginal hysterectomy to be aware of these potential complications and to discuss them with their healthcare provider. Regular check-ups and pelvic exams can help detect any issues early on and prevent further complications. Additionally, women can take steps to reduce their risk of developing these conditions by maintaining a healthy weight, avoiding heavy lifting, and practicing pelvic floor exercises. By being proactive and informed, women can minimize the impact of long-term complications and enjoy a better quality of life after surgery.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 28
Correct
-
A patient is admitted from clinic eight weeks following a renal transplant. Despite feeling well, his creatinine has increased from a baseline of 120 umol/l to 170 umol/l in just one week. After a normal ultrasound scan, he undergoes a transplant biopsy which reveals linear C4d staining along the peritubular capillaries and widespread glomerulitis with neutrophil and macrophage infiltration. What is the probable diagnosis?
Your Answer: Antibody mediated rejection
Explanation:C4d Staining as a Marker for Antibody Mediated Rejection
Linear staining for C4d is a useful tool in detecting complement activation via the classical pathway, which is mediated by antibodies. C4d is a breakdown component of C4 that binds to the basement membrane, indicating antibody mediated complement activation. In cases where antibody mediated rejection is suspected, C4d staining is highly sensitive for acute rejection. A serum sample for donor specific antibodies should be sent off urgently to confirm the diagnosis.
Chronic background antibody mediated rejection can also show C4d staining, but the presence of C4d along the peritubular capillaries is a strong indicator of acute antibody mediated rejection. This, along with the presence of glomerulitis and acute inflammatory infiltrate, supports the diagnosis of acute antibody mediated rejection.
Other conditions, such as acute tubular necrosis, bacterial pyelonephritis, acute viral infection, and acute cellular rejection, can be ruled out based on their distinct features. Acute tubular necrosis shows flattening of the tubular epithelium with sloughing of the cells, while bacterial pyelonephritis tends to cause a tubulointerstitial nephritis. Acute viral infection and acute cellular rejection both show lymphocytic infiltration rather than granulocyte infiltration, but can be distinguished through blood viral PCR and virus specific stains.
In summary, C4d staining is a valuable tool in detecting antibody mediated complement activation and can aid in the diagnosis of acute antibody mediated rejection. Other conditions can be ruled out based on their distinct features, and further testing may be necessary to confirm the diagnosis.
-
This question is part of the following fields:
- Nephrology
-
-
Question 29
Incorrect
-
You are requested to evaluate a 22-year-old man who had undergone an incision and drainage procedure for pilonidal abscess. The nursing staff is worried about his unusual behavior. He has admitted to social cannabis use in the past.
Upon arrival, you observe that he is forcefully sticking out his tongue and bending his neck to the left and right. His eyes are looking upwards, and his pupils are dilated. His blood glucose level is 5 mmol/L, and all routine observations are normal. He was given paracetamol and an anti-emetic ten minutes ago.
What is the most suitable course of treatment?Your Answer: Call security and the on-call psychiatrist
Correct Answer: Intravenous procyclidine
Explanation:Oculogyric Crisis
Oculogyric crisis is a type of acute dystonic reaction that is commonly associated with the use of neuroleptics and anti-emetic medications like metoclopramide. Unfortunately, the clinical spectrum of this condition is not well understood, which often leads to misdiagnosis as a psychogenic disorder. Symptoms of oculogyric crisis can occur suddenly or over several hours and may include restlessness, agitation, malaise, and a fixed stare. The most characteristic symptom is the upward deviation of the eyes, which may be sustained or accompanied by other eye movements like convergence or lateral deviation. Other associated symptoms may include neck flexion, mouth opening, tongue protrusion, and ocular pain. Fortunately, the symptoms of oculogyric crisis can be rapidly resolved with the use of medications like procyclidine.
-
This question is part of the following fields:
- Anaesthetics & ITU
-
-
Question 30
Incorrect
-
A study is conducted to investigate the relationship between age and development of heart failure. Age was categorized as ‘under 50’ or ‘50 and over’. The outcome measure was development of heart failure. 2000 individuals were included in the study, of which 300 have heart failure. A total of 60 with heart failure are under 50 years old; 40 without heart failure are under 50 years old. What is the odds ratio of getting heart failure in those under 50 years old versus those who are 50 and over?
Your Answer: 0.2
Correct Answer: 10.4
Explanation:Calculating Odds Ratio in a Contingency Table
Interpreting data presented in a contingency table can be useful in determining the odds ratio of a particular condition. The odds ratio is calculated by dividing the odds of contracting the condition in the exposed group by the odds of contracting the condition in the unexposed group. For example, if the contingency table shows that 30 cases of heart failure occurred in smokers and 120 cases occurred in non-smokers, while 20 controls were smokers and 830 controls were non-smokers, the odds ratio would be (30/20) / (120/830), which equals 10.4. This means that patients who smoke are over ten times more likely to develop heart failure compared to non-smokers. Other odds ratios can be calculated in a similar manner for different conditions and exposures.
-
This question is part of the following fields:
- Statistics
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)