-
Question 1
Incorrect
-
A 30-year-old man was admitted to the emergency department following a car crash. He was found to be in a profound coma and subsequently pronounced brain dead.
What is the accurate diagnosis in this case?Your Answer: Brain death testing should be undertaken by two separate doctors on separate occasions, one of them must be a member of the intensive care team
Correct Answer: Brain death testing should be undertaken by two separate doctors on separate occasions
Explanation:To ensure accuracy, brain death testing must be conducted by two experienced doctors who are knowledgeable in performing brain stem death testing. These doctors should have at least 5 years of post-graduate experience and must not be members of the transplant team if organ donation is being considered. The patient being tested should have normal electrolytes and no reversible causes, as well as a deep coma of known aetiology and no sedation. The knee jerk reflex is not used in brain death testing, instead, the corneal reflex and oculovestibular reflexes are tested through the caloric test. It is important to note that brain death testing should be conducted by two separate doctors on separate occasions.
Criteria and Testing for Brain Stem Death
Brain death occurs when the brain and brain stem cease to function, resulting in irreversible loss of consciousness and vital functions. To determine brain stem death, certain criteria must be met and specific tests must be performed. The patient must be in a deep coma of known cause, with reversible causes excluded and no sedation. Electrolyte levels must be normal.
The testing for brain stem death involves several assessments. The pupils must be fixed and unresponsive to changes in light intensity. The corneal reflex must be absent, and there should be no response to supraorbital pressure. The oculovestibular reflexes must be absent, which is tested by injecting ice-cold water into each ear. There should be no cough reflex to bronchial stimulation or gagging response to pharyngeal stimulation. Finally, there should be no observed respiratory effort in response to disconnection from the ventilator for at least five minutes, with adequate oxygenation ensured.
It is important that the testing is performed by two experienced doctors on two separate occasions, with at least one being a consultant. Neither doctor can be a member of the transplant team if organ donation is being considered. These criteria and tests are crucial in determining brain stem death and ensuring that the patient is beyond recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 2
Incorrect
-
Which of the following types of renal stones are radiolucent?
Your Answer: Triple phosphate stones
Correct Answer: Xanthine stones
Explanation:On an x-ray, cystine stones appear semi-opaque while urate and xanthine stones are radiolucent.
Types of Renal Stones and their Appearance on X-ray
Renal stones, also known as kidney stones, are solid masses that form in the kidneys due to the accumulation of certain substances. There are different types of renal stones, each with a unique appearance on x-ray. Calcium oxalate stones are the most common, accounting for 40% of cases, and appear opaque on x-ray. Mixed calcium oxalate/phosphate stones and calcium phosphate stones also appear opaque and make up 25% and 10% of cases, respectively. Triple phosphate stones, which develop in alkaline urine and are composed of struvite, account for 10% of cases and appear opaque as well. Urate stones, which are radiolucent, make up 5-10% of cases. Cystine stones, which have a semi-opaque, ‘ground-glass’ appearance, are rare and only account for 1% of cases. Xanthine stones are the least common, accounting for less than 1% of cases, and are also radiolucent. Staghorn calculi, which involve the renal pelvis and extend into at least 2 calyces, are composed of triple phosphate and are more likely to develop in alkaline urine. Infections with Ureaplasma urealyticum and Proteus can increase the risk of their formation.
-
This question is part of the following fields:
- Surgery
-
-
Question 3
Incorrect
-
A 50-year-old man is at his pre-operative assessment for his scheduled hernia repair next week. During the consultation, he informs the anaesthetist that his father and brother had a reaction to an anaesthetic in the past, which was later diagnosed as malignant hyperthermia.
What medication should the anaesthetist avoid administering in this situation?Your Answer: Ketamine
Correct Answer: Suxamethonium
Explanation:Out of the drugs listed, suxamethonium is the only one that can trigger malignant hyperthermia. The rest of the drugs are considered safe for use in individuals with this condition.
Malignant Hyperthermia: A Condition Triggered by Anaesthetic Agents
Malignant hyperthermia is a medical condition that often occurs after the administration of anaesthetic agents. It is characterized by hyperpyrexia and muscle rigidity, which is caused by the excessive release of calcium ions from the sarcoplasmic reticulum of skeletal muscle. This condition is associated with defects in a gene on chromosome 19 that encodes the ryanodine receptor, which controls calcium release from the sarcoplasmic reticulum. Susceptibility to malignant hyperthermia is inherited in an autosomal dominant fashion. It is worth noting that neuroleptic malignant syndrome may have a similar aetiology.
The causative agents of malignant hyperthermia include halothane, suxamethonium, and other drugs such as antipsychotics (which can trigger neuroleptic malignant syndrome). To diagnose this condition, doctors may perform tests such as checking for elevated levels of creatine kinase and conducting contracture tests with halothane and caffeine.
The management of malignant hyperthermia involves the use of dantrolene, which prevents the release of calcium ions from the sarcoplasmic reticulum. With prompt and appropriate treatment, patients with malignant hyperthermia can recover fully. Therefore, it is essential to be aware of the risk factors and symptoms of this condition, especially when administering anaesthetic agents.
-
This question is part of the following fields:
- Surgery
-
-
Question 4
Correct
-
A 26-year-old man has arrived at the Emergency Department with sudden-onset, deteriorating right lower quadrant abdominal pain. He has a significantly decreased appetite and has vomited multiple times in the past few days. During the examination, there is notable tenderness upon palpation in the right iliac fossa. A CT scan of the abdomen confirms the diagnosis of acute appendicitis. After consulting with a surgeon, it is decided that an emergency open appendectomy is necessary. What is the most suitable preoperative management for this patient?
Your Answer: A single dose of intravenous (iv) Tazocin® 30 minutes before the procedure
Explanation:Preoperative Management for Gastrointestinal Surgery
Surgical site infections are a common complication of gastrointestinal surgery, with up to 60% of emergency procedures resulting in infections. To prevent this, a single dose of broad-spectrum antibiotics, such as Tazocin®, should be given intravenously 30 minutes before the procedure. Patients should also be hydrated with iv fluids and be nil by mouth for at least six hours before surgery. In cases of potential post-operative intestinal obstruction or ileus, a nasogastric tube may be necessary. However, narrow-spectrum antibiotics like iv flucloxacillin are not appropriate for prophylaxis in this case. Finally, VTE prophylaxis with LMWH should be given preoperatively but stopped 12 hours before the procedure.
-
This question is part of the following fields:
- Surgery
-
-
Question 5
Incorrect
-
To which bone does Sever's disease refer, and at what age is it commonly diagnosed?
Your Answer: Radius
Correct Answer: Calcaneum
Explanation:Sever’s Disease
Sever’s disease is a condition that causes pain in one or both heels when walking or standing. It occurs due to a disturbance or interruption in the growth plates located at the back of the heel bone, also known as the calcaneus. This condition typically affects children between the ages of 8 and 13 years old.
The pain associated with Sever’s disease can occur after general activities such as running, jumping, or playing sports like netball, basketball, and football. Symptoms include extreme pain when placing the heel on the ground, which can be alleviated when the child walks on their tiptoes.
In summary, Sever’s disease is a common condition that affects children during their growth and development. It is important to recognize the symptoms and seek medical attention if necessary to ensure proper treatment and management of the condition.
-
This question is part of the following fields:
- Surgery
-
-
Question 6
Correct
-
You are the F2 in general practice. You see a 75-year-old man who is complaining of changes in the appearance of his legs. On examination, you can see areas of brown on the legs, dry skin, and the calves appear significantly wider at the knee than the ankle.
What is the man most at risk of?Your Answer: Venous ulcers
Explanation:Chronic venous insufficiency is indicated by brown pigmentation (haemosiderin), lipodermatosclerosis (resembling champagne bottle legs), and eczema. These symptoms increase the likelihood of developing venous ulcers, which typically appear above the medial malleolus. Arterial ulcers are more commonly associated with peripheral arterial disease, while neuropathic ulcers are prevalent in individuals with diabetes.
Venous leg ulcers are the most common and are caused by venous hypertension. Arterial ulcers occur on the toes and heel and are painful without palpable pulses. Neuropathic ulcers commonly occur over the plantar surface and can lead to amputation in diabetic patients. Marjolin’s ulcers are squamous cell carcinomas that occur at sites of chronic inflammation. Pyoderma gangrenosum is associated with inflammatory bowel disease and presents as erythematosus nodules or pustules that ulcerate. Management varies depending on the type of ulcer.
-
This question is part of the following fields:
- Surgery
-
-
Question 7
Correct
-
A 65-year-old woman with a T4N0M0 primary triple-negative breast carcinoma is attending a pre-operative breast oncology clinic. The oncologist recommends neo-adjuvant chemotherapy (NACT) as a beneficial course of treatment. What should the patient be informed of when considering whether to undergo NACT?
Your Answer: NACT can downsize the primary tumour, meaning that breast conserving surgery can be performed instead of a mastectomy
Explanation:One of the main reasons for considering neo-adjuvant chemotherapy in breast cancer treatment is to shrink the size of the tumor before surgery. This can potentially allow for breast conserving surgery instead of a mastectomy, which has several benefits. Firstly, it is a less invasive surgical procedure, reducing the risks associated with surgery. Additionally, it can lead to better cosmetic outcomes for the patient.
It is important to note that both NACT and surgery have their own set of side effects, which cannot be compared with each other. However, there is an exciting new area of breast cancer research that focuses on immunomodulation. Some trials have shown that anti-tumor immunity can be induced following cryoablation/radiotherapy and administration of immunomodulating drugs. Unfortunately, NACT does not have this effect.
One common side effect of NACT is nausea. The effect of NACT on overall survival rates has been mixed, but its main indication remains downsizing of the primary tumor.
Reference:
Nice guideline NG101 (2018).Breast cancer management varies depending on the stage of the cancer, type of tumor, and patient’s medical history. Treatment options may include surgery, radiotherapy, hormone therapy, biological therapy, and chemotherapy. Surgery is typically the first option for most patients, except for elderly patients with metastatic disease who may benefit more from hormonal therapy. Prior to surgery, an axillary ultrasound is recommended for patients without palpable axillary lymphadenopathy, while those with clinically palpable lymphadenopathy require axillary node clearance. The type of surgery offered depends on various factors, such as tumor size, location, and type. Breast reconstruction is also an option for patients who have undergone a mastectomy.
Radiotherapy is recommended after a wide-local excision to reduce the risk of recurrence, while mastectomy patients may receive radiotherapy for T3-T4 tumors or those with four or more positive axillary nodes. Hormonal therapy is offered if tumors are positive for hormone receptors, with tamoxifen being used in pre- and perimenopausal women and aromatase inhibitors like anastrozole in postmenopausal women. Tamoxifen may increase the risk of endometrial cancer, venous thromboembolism, and menopausal symptoms. Biological therapy, such as trastuzumab, is used for HER2-positive tumors but cannot be used in patients with a history of heart disorders. Chemotherapy may be used before or after surgery, depending on the stage of the tumor and the presence of axillary node disease. FEC-D is commonly used in the latter case.
-
This question is part of the following fields:
- Surgery
-
-
Question 8
Correct
-
A 50-year-old woman arrives at the Emergency Department complaining of cramp-like abdominal pain, nausea, and vomiting that started 4 hours ago. She describes the pain as intermittent and has experienced similar pain before, but not as severe as this time. The patient has a history of chronic obstructive pulmonary disease, which is well-controlled with inhalers, and has been a smoker for 25 pack years.
Her vital signs are heart rate 110/min, respiratory rate 20/min, blood pressure 130/84 mmHg, temperature 38.6ºC, and oxygen saturation of 99% on room air. Upon examination, the patient appears very ill and sweaty, with some yellowing of the eyes. Palpation of the abdomen reveals tenderness in the right upper quadrant.
What is the most likely cause of the patient's symptoms?Your Answer: Ascending cholangitis
Explanation:Cholangitis can occur even in the absence of stones, although they are commonly associated with the condition. ERCP can be used to drain the biliary tree, but surgical exploration of the common bile duct may be necessary in certain cases.
Understanding Ascending Cholangitis
Ascending cholangitis is a bacterial infection that affects the biliary tree, with E. coli being the most common culprit. This condition is often associated with gallstones, which can predispose individuals to the infection. Patients with ascending cholangitis may present with Charcot’s triad, which includes fever, right upper quadrant pain, and jaundice. However, this triad is only present in 20-50% of cases. Other common symptoms include hypotension and confusion. In severe cases, Reynolds’ pentad may be observed, which includes the additional symptoms of hypotension and confusion.
To diagnose ascending cholangitis, ultrasound is typically used as a first-line investigation to look for bile duct dilation and stones. Raised inflammatory markers may also be observed. Treatment involves intravenous antibiotics and endoscopic retrograde cholangiopancreatography (ERCP) after 24-48 hours to relieve any obstruction.
Overall, ascending cholangitis is a serious condition that requires prompt diagnosis and treatment. Understanding the symptoms and risk factors associated with this condition can help individuals seek medical attention early and improve their chances of a successful recovery.
-
This question is part of the following fields:
- Surgery
-
-
Question 9
Correct
-
A 62-year-old man presents to the pre-admission clinic for assessment prior to an elective prostatectomy. You find no adverse past medical history and examination is unremarkable. An electrocardiogram (ECG) is indicated in all pre-operative patients undergoing major surgery who are over the age of 60. The ECG is shown below.
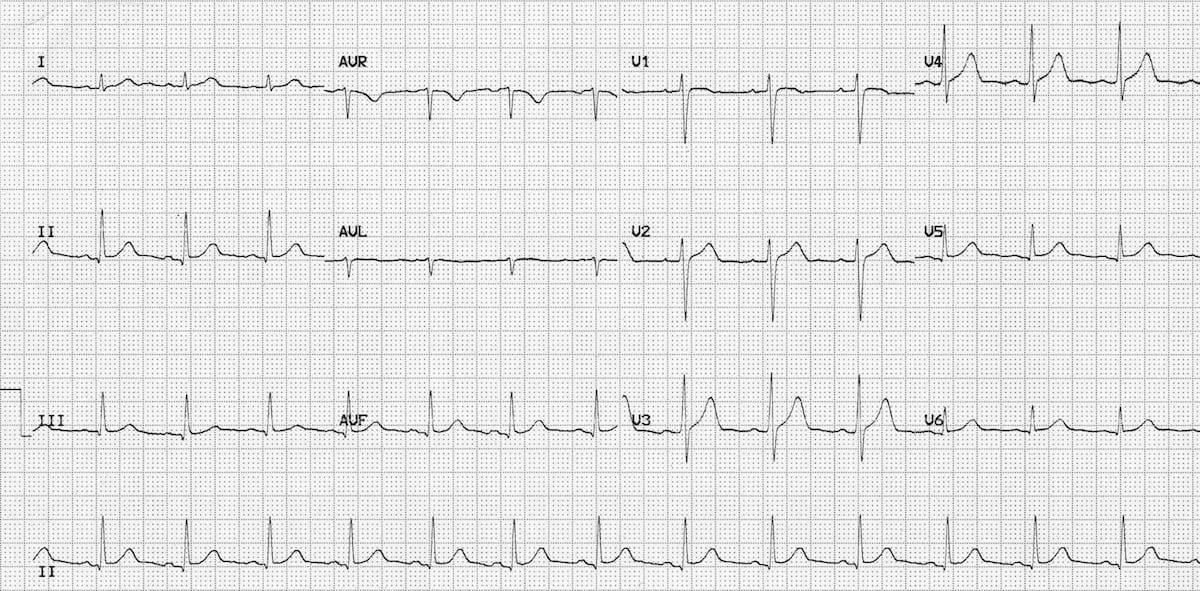 After having reviewed the ECG, what is the next best step to take with this patient?
After having reviewed the ECG, what is the next best step to take with this patient? Your Answer: No further assessment is required
Explanation:Assessing Cardiac Risk in Preoperative Patients: Common Misconceptions
There are several misconceptions when it comes to assessing cardiac risk in preoperative patients. One common mistake is assuming that all patients require extensive cardiac testing, even when there are no significant risk factors or symptoms present. For example, if a patient has no significant past medical history and their examination is unremarkable, an echocardiogram is not necessary.
On the other hand, some clinicians may be too cautious and cancel a patient’s procedure based on a perceived cardiac risk that is not supported by evidence. If the patient’s ECG is normal and there are no cardiac risk factors, cancelling the procedure would be unreasonable.
It is important to recognise that not all preoperative patients require extensive cardiac testing. Instead, clinicians should focus on identifying patients with specific cardiac conditions that require closer monitoring and management. By avoiding unnecessary testing and interventions, clinicians can improve patient outcomes and reduce healthcare costs.
-
This question is part of the following fields:
- Surgery
-
-
Question 10
Incorrect
-
A 45-year-old man is recovering on the surgical ward three days after a laparotomy and right hemicolectomy for cancer. You are asked to see him as he has developed a temperature of 38.5ºC and is tachycardic at 120 bpm and tachypnoeic at 25 breaths per minute. On examination his abdomen is soft and not distended but tender around his midline wound. There is some discharge seeping through the dressing. His chest is clear and he has no signs of a deep vein thrombosis.
What is the most probable cause of this man's elevated temperature?Your Answer: Physiological response to surgery
Correct Answer: Wound infection
Explanation:Abdominal wound infections can lead to post-operative fevers after a few days and may be accompanied by signs of systemic infection. This is a common urgent call for junior surgeons, and the two main differentials to consider are infection and thrombosis, as they are the most serious causes of post-operative fever. Given that the operation involved the bowel and was not sterile, a wound infection is the most likely differential, especially with the presence of discharge and tenderness. While an anastomotic leak is possible, it would typically present with a painful, firm abdomen and severe sepsis. There are no indications of a chest pathology from the patient’s history or examination. A physiological cause of fever would not be associated with systemic inflammation symptoms, as seen in this case.
Post-operative pyrexia, or fever, can occur after surgery and can be caused by various factors. Early causes of post-op pyrexia, which typically occur within the first five days after surgery, include blood transfusion, cellulitis, urinary tract infection, and a physiological systemic inflammatory reaction that usually occurs within a day following the operation. Pulmonary atelectasis is also often listed as an early cause, but the evidence to support this link is limited. Late causes of post-op pyrexia, which occur more than five days after surgery, include venous thromboembolism, pneumonia, wound infection, and anastomotic leak.
To remember the possible causes of post-op pyrexia, it is helpful to use the memory aid of the 4 W’s: wind, water, wound, and what did we do? (iatrogenic). This means that the causes can be related to respiratory issues (wind), urinary tract or other fluid-related problems (water), wound infections or complications (wound), or something that was done during the surgery or post-operative care (iatrogenic). It is important to identify the cause of post-op pyrexia and treat it promptly to prevent further complications. This information is based on a peer-reviewed publication available on the National Center for Biotechnology Information website.
-
This question is part of the following fields:
- Surgery
-
00
Correct
00
Incorrect
00
:
00
:
00
Session Time
00
:
00
Average Question Time (
Secs)